International Journal of Otolaryngology and Head & Neck Surgery
Vol. 1 No. 3 (2012) , Article ID: 25100 , 3 pages DOI:10.4236/ijohns.2012.13017
Angiosarcoma of Maxillary Sinus: A Case Report
Department of Otorhinolaryngology, Yashoda Hospital, Secunderabad, India
Email: *aarticlinic@yahoo.com
Received June 27, 2012; revised July 28, 2012; accepted August 22, 2012
Keywords: Angiosarcoma of Maxilla; Sarcoma
ABSTRACT
Purpose: To describe a rare malignancy involving the sinonasal cavities. To discuss the clinical, diagnostic, and treatment modalities. Study Design: A case report including histopathological, radiological analysis and review of literature. Method: A case report is described from a tertiary care centre. Histopathological and radiological details are reviewed. Results: This case report presents a 29 year old male with 3 days history of bleeding from the left nostril, blood stained saliva with post nasal discharge and head ache. Biopsy demonstrated poorly differentiated Angiosarcoma. On immune stains the tumor cells showed diffuse strong cytoplasmic membrane positivity with CD 31 and few cells are positive for CD34. FLI-1 is also positive. Conclusion: Angiosarcoma is a rare malignancy involving the sinonasal cavities. Multidisciplinary approach is essential to obtain clear diagnoses and appropriate treatment plans.
1. Introduction
Angiosarcoma is uncommon, accounting for less than 1% of all sinonasal tract malignancies .They occur in all ages, with a peak in the 5th decade, and a male predilection (male:female = 2:1). Females tend to be younger at presentation by up to a decade. Angiosarcomas are malignant neoplasias of rapid growth that develop from endothelial cells [1]. Since 1977 only 17 cases have been reported in literature. They present as a mass lesion with or without epistaxis and airway obstruction [2]. Complete surgical excision is the treatment of choice especially with well delineated and solitary tumours [1]. Radiotherapy and chemotherapy may be of benefit in multifocal, ill-defined tumors [3]. Consideration of angiosarcoma in the differential diagnosis of mass lesions involving the sinonasal cavities with or without bleeding is critical.
2. Case Report
A 29-year-old male patient presented with a 3 day history of bleeding from the left nasal cavity, blood stained post nasal discharge with occasional nasal block and head ache. Patient had a past history of cauterization in the nasal cavity elsewhere 6 months back. On clinical examination, there is deviation of the nasal septum to left side with spur. Small reddish area over the septum about 1 cm from the columella on left side. There is no active anterior bleeding but post nasal discharge with blood was observed, CT scan of paranasal sinuses revealed left maxillary sinus opacity with lesion measuring 3.45 cm, 2.85 cm, and 3 cm, Figure 1 and demineralization of medial wall of maxillary sinus Figure 2. Patient was treated in the form of uncinectomy, followed by a large middle meatal antrostomy and anterior ethmoidectomy. Pedunculated mass arising from left maxillary sinus anterolateral wall excised in toto. Histopathological examination of specimen demonstrated poorly differentiated angiosarcoma. The microscopic view showed mucosal fragments that are focally ulcerated with areas of hemorrhage and necrosis. A neoplastic proliferation of cells is seen composed of spindle to ovoid cells arranged around slit-like vascular spaces and dissecting the collagen on the deeper aspect where they are seen like intercommunicating spaces. They have vesicular nuclei with nucleoli and show mild to moderate pleomorphism with many mitosis. On immune stains, the tumour cells showed diffuse strong cytoplasmic membrane positivity with CD31 and few cells (about 10%) are positive for CD34. FLI-1 is also positive. Patient was advised to undergo total maxillectomy, but patient lost for follow up.
3. Discussion
Angiosarcoma (malignant haemangioendothelioma) [4] are defined as malignant neoplasms of vascular phenotype whose constituent tumour cells have endothelial features. It is a very rare tumor, only 17 cases have been reported since 1977. They tend to be nodular or ulcerative, ill-defined with a bluish red colour. Etiology is unknown and has been associated to certain risk factors

Figure 1. CT PNS coronal section showing opacity in left maxillary sinus.

Figure 2. CT PNS Axial section showing opacity in left maxillary sinus with destruction of the medial wall.
such as chronic lymphedema, radiation exposure, thorotrast, arsenic and vinyl chloride trauma and telangiectatic skin lesions are reported risk factors. The maxillary sinus is most frequently affected. Other sites that may be involved primarily or secondarily include the nasal cavity and other paranasal sinuses.
Patients present with recurrent epistaxis, profound pallor, a mass lesion, pain (including headache, otalgia, toothache), nasal obstruction, sinusitis, nasal discharge (often described as foul smelling and blood tinged), paraesthesia and/or loose teeth. The duration of symptoms ranges from weeks to months, but is generally short (median, 4 months). Lymph node and distant metastasis is not common at presentation.
Histologically, most of these tumours are low-grade. Includes a proliferation of ramifying and anastomosing vascular channels which dissect through the surrounding structures [3]. The endothelial cells lining the vascular spaces are plump, atypical, increased in number and pile up along the lumen creating papillations [3]. They demonstrate mitotic activity. The endothelial cells may appear spindled, epithelioid or polygonal [1] Figure 3. Im-
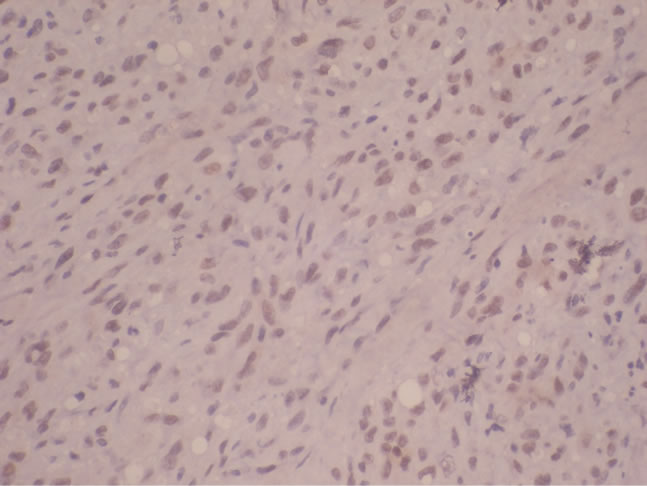
Figure 3. Histopathological section of angiosarcoma.
munohistochemical stains assist in the diagnosis. Reactivity is identified with either factor VIII related antigen [5], CD31 or CD34 [6].
The differential diagnoses include granulation tissue, intravascular papillary endothelial hyperplasia, hemangioma, nasopharyngeal angiofibroma, angiolymphoid hyperplasia with eosinophilia, glomangio pericytoma, Kaposi sarcoma, malignant melanoma, carcinoma and large cell lymphoma.
Complete surgical excision is the treatment of choice, especially with well delineated and solitary tumours [3]. Radiotherapy and chemotherapy may be of benefit in multifocal, ill-defined tumours [3]. Metastasis is uncommon, and the predilection sites are the lung, liver, spleen and bone marrow. Recurrences are common in approximately 50% of cases. It is likely due to incomplete excision or possible multifocality. The outcome is more favorable in case of angiosarcoma of maxilla when compared with the almost uniformly fatal outcome for cutaneous and soft tissue angiosarcomas.
4. Conclusion
Angiosarcoma is a malignant neoplasm of vascular phenotype. Etiology is unknown. Histologically, most of these tumours are low-grade. In this case it is of high grade with multifocality. Immunohistochemical stains assist in the diagnosis. Reactivity is identified with either factor VIII related antigen, CD31 or CD34. Complete surgical excision is the treatment of choice. Radiotherapy and chemotherapy may be of benefit in multifocal, illdefined tumours. Recurrences are common, likely due to incomplete excision or possible multifocality.
REFERENCES
- N. Zachariades and P. Economopoulou, “Maxillary Angiosarcoma,” International Journal of Oral and Maxillofacial Surgery, Vol. 15, No. 3, 1986, pp. 357-360. Hdoi:10.1016/S0300-9785(86)80101-6
- M. Bankaci, E. N. Myers, L. Barnes, et al., “Angiosarcoma of the Maxillary Sinus,” Head & Neck Surgery, Vol. 1, No. 3, 1979, pp. 274-280. Hdoi:10.1002/hed.2890010311
- D. M. F. Christopher, “Diagnostic Histopathology of Tumors,” Elsevier Health Sciences Imprint, Churchill Livingstone, Vol. 1, 2007, p. 131.
- M. Kurien, S. Nair and S. Thomas, “Angiosarcoma of the Nasal Cavity and Maxillary Antrum,” Journal of Laryngology & Otology, Vol. 103, No. 9, 1989, pp. 874-876. Hdoi:10.1017/S0022215100110369
- Y. Kimura, S. Tanaka and M. Furukawa, “Angiosarcoma of the Nasal Cavity,” Journal of Laryngology & Otology, Vol. 106, No. 4, 1992, pp. 368-369. Hdoi:10.1017/S0022215100119528
- B. L. Nelson and L. D. R. Thompson, “Sinonasal Tract Angiosarcoma: A Clinicopathologic and Immunophenotypic Study of 10 Cases with a Review of the Literature,” Head and Neck Pathology, Vol. 1, No. 1, 2007, pp. 1-12. Hdoi:10.1007/s12105-007-0017-2
NOTES
*Corresponding author.