Open Journal of Nephrology
Vol.3 No.1(2013), Article ID:29070,4 pages DOI:10.4236/ojneph.2013.31006
Estimation of GFR by MDRD Formula and Its Correlation to Cockcroft-Gault Equation in Five Stages of Chronic Kidney Disease
1Department of Medicine, Aga Khan University, Karachi, Pakistan
2Liaquat National Hospital, Karachi, Pakistan
Email: *draliabsar@yahoo.com
Received December 7, 2012; revised February 9, 2013; accepted March 11, 2013
Keywords: MDRD; Cockcroft-Gault; Chronic kidney disease; CKD
ABSTRACT
Background: Purpose of our study was to find out correlation between estimated Glomerular Filtration Rate (GFR) by Modification of Diet in Renal Disease (MDRD) formula and Glomerular Filtration Rate by Cockcroft-Gault equations, in patients with chronic kidney disease (CKD), and to see whether they can be used interchangeably. Methods: We conducted a cross section study of 70 patients presented to the nephrology clinic over a period of one year. We compared the Glomerular Filtration Rate by these two formulas in five stages of Chronic Kidney Disease. Abbreviated 4 variable Modification of Diet in Renal Disease formula was used. Results: Age range was 15 - 79 years; Male 49%, Female 51%. The correlation (r) between eGFR by MDRD and eGFR by Cockcroft-Gault equation for CKD stages 1 to 5 was 0.64; 0.31; 0.32; 0.67; and 0.45 respectively. The correlation (r) between creatinine clearance by 24 hour urine collection and MDRD formula was 0.84 (P: 0.001). The correlation (r) between creatinine clearance by 24 hour urine collection Cockcroft-Gault equation was 0.79 (P: 0.001). Conclusion: We conclude that Cockcroft-Gault equation correlates best with MDRD formula at CKD stages 4 and one. Cockcroft-Gault equation underestimated eGFR in stages 1, 2 and 3 of chronic Kidney Disease.
1. Introduction
Modification of Diet in Renal Disease (MDRD) formula and Cockcroft-Gault equation are commonly used for estimation of Glomerular Filtration Rate (GFR). Creatinine clearance measurement using 24 hours urine collection is largely abandoned in favor of the MDRD and Cockcroft-Gault formulas, mainly because of the inherited difficulties in accurate collection of 24 hours urine.
Cockcroft-Gault equation remained the most common method for bedside estimation of GFR because it is very easy to use without a calculator or computer. This advantage of Cockcroft-Gault formula is keeping it alive in spite of the rapid popularity of MDRD formula. Numerous studies are done to compare these two equations in various settings. However the data from Asia especially from Pakistan is scanty [1].
Purpose of our study was to find out correlation between the two equations in chronic kidney disease (CKD) in our setting and to see whether they can be used interchangeably. A review of similar studies from other georophical location is also presented.
2. Methods
We conducted a cross section study of 70 patients of age 15 and above who presented to the nephrology clinic of a tertiary care hospital in Karachi Pakistan over a period of 1 year.
Abbreviated four variable MDRD formula was used to estimate GFR using the equation: 186 × [serum creatinine (mg/dl)]−1.154 × (age)−0.203 × (0.742 if female). Estimated GFR using the Cockcroft-Gault equation was calculated as follows: (140 − age) × (weight in kg)/serum creatinine (mg/dl) × 72 × (0.85 if female). Measured creatinine clearance was calculated by 24 hour urine collection and using the formula: creatinine excretion (mg/kg/day) divided by serum creatinine (mg/dl) divided by 14.4 (min/d per dl/ml).
Patients with acute renal failure were excluded. All the patients in the study were divided into five groups corresponding to the five stages of chronic kidney disease as follows: Group 1: GFR > 90; Group 2: GFR 90 - 60; Group 3: GFR 30 - 59; Group 4: GFR 15 - 29 and group 5: GFR < 15 ml/min/1.73m2 [2]. Data was analyzed using SPSS software.
3. Results
Age range was 15 - 79 years. Male were 49%, female were 51%. Mean GFR by MDRD formula for CKD stages 1 to 5 was 111 ± 30, 77 ± 24, 39 ± 9, 21 ± 6 and 13 ± 4 ml/min/1.73m2 respectively. Mean GFR by Cockcroft-Gault equation for CKD stage 1 to 5 was 119 ± 28, 78 ± 13, 43 ± 7, 23 ± 3 and 12 ± 2 ml/min/1.73m2 respectively (table 1). The correlation coefficient (r) between eGFR by MDRD and eGFR by Cockcroft-Gault for CKD stages 1 - 5 was 0.64; 0.31; 0.32; 0.67; and 0.45 respectively (table 2).
Mean and median eGFR by MDRD was 48 ± 40 and 32 (58-7) ml/min/1.73m2 respectively for all patients. Mean and median eGFR by Cockcroft-Gault was 52 ± 42 and 36 (197-7) ml/min/1.73m2 respectively for all patients (table 3).
The Cockcroft-Gault equation correlated best with MDRD formula at CKD stage four followed by the stage one. The creatinine clearance by 24 urine collection was correlated to the eGFR by MDRD formula. The r value was 0.84 with p value of 0.001. Similarly the creatinine clearance by 24 urine collection was correlated to the eGFR by Cockcroft-Gault equation. The r value was 0.79 with p value of 0.001 (Table 4).
Table 1. Mean estimated GFR in each group.
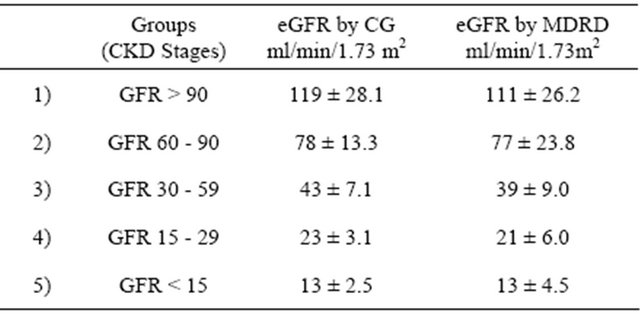
CG: Cockcroft-Gault; MDRD: modification of diet in renal disease; CKD: chronic kidney disease.
Table 2. Correlation between eGFR by CG and eGFR by MDRD.
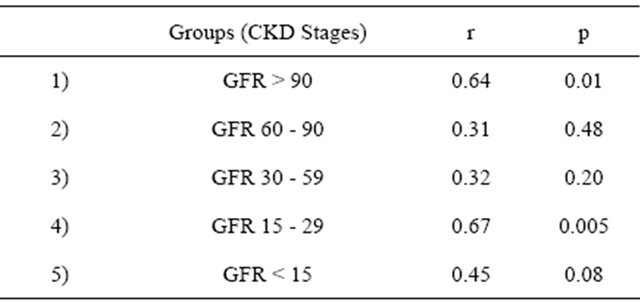
CG: Cockcroft-Gault; MDRD: modification of diet in renal disease.
Table 3. Overall average eGFR by CG and MDRD formulas.
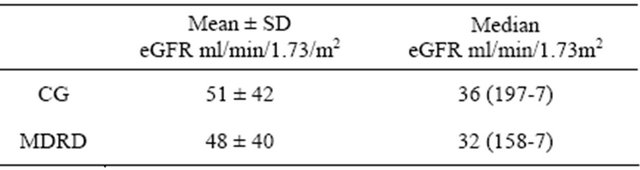
CG: Cockcroft-Gault; MDRD: modification of diet in renal disease; eGFR: estimated glomerular filtration rate.
Table 4. Correlation between “24 Hour Urine CrCl” and eGFR by Cockcroft-Gault and MDRD formulas.
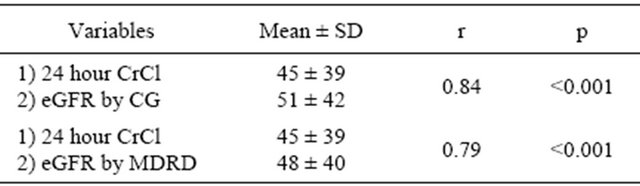
CrCl: creatinine clearance; CG: Cockcroft-Gault; MDRD: modification of diet in renal disease; eGFR: estimated glomerular filtration rate.
4. Discussion
Accurate measurement of GFR in chronic kidney disease can not be overemphasized. It is especially important when GFR reaches near stage 3 and 4. The important decision like making AV fistula and initiation of renal replacement therapy are taken at this time.
There are more than eight formulas available to estimate GFR but only two namely Cockcroft-Gault equation and MDRD got the acceptance by the medical community. The Cockcroft-Gault equation was proposed as early as 1976 [2]. Because of its simplicity and bedside use, it was readily accepted by the physicians. The Cockcroft-Gault equation enjoyed this monopoly till the MDRD equation was introduced in 1999 [3].
Twenty four hour urine collection for Creatinine clearance measurement is not the method of choice because of several pitfalls. The most important being the 24 hour urine collection is often not accurate. In addition increased tubular secretion of creatinine in renal failure results in overestimation of GFR.
Using Inulin clearance to measure GFR is very cumbersome and not practical for routine clinical practice. Alternatively, the radioactive and non-radioactive based markers e.g. Iothalamate, Iohexol, DTPA and EDTA are used. The isotope based GFR measurements are thought to be the most accurate but they are costly and not available in many laboratories. Therefore their utility is confined practically to research. Inulin and Isptope methods are used as a gold standard to validate the accuracy of eGFR by MDRD or Cockcroft-Gault equation equations. However we used the traditional 24 hour urine collection to calculate creatinine clearance and compare it with MDRD formula and Cockcroft-Gault equation because of the lack of resources. We were very particular and thorough in giving the instruction to the patients. The strong correlation of 24 hour creatinine clearance to eGFR by Cockcroft-Gault equation as well as MDRD formula goes in favor of our assumption that urine collections were accurate.
MDRD study equation originally required six variables namely Serum Creatinine, Serum Albumin, Serum Urea Nitrogen, Gender, Age and Race. Later a simpler four variable equation was proposed and is considered to be a good as six variable equation [4]. This abbreviated MDRD equation requires Serum Creatinine, Age, Gender and Race only. It does not require Serum Albumin and Serum Urea Nitrogen. The use of standardized serum creatinine in re-expressed 4 variable MDRD formula improves the accuracy [5,6]. Studies have shown that adjustment for body surface area improves the accuracy of Cockcroft-Gault formula [7,8]. The need of this simpler four variable MDRD equation raised due to difficulty of using 6 variable equation on bedside. However still its main drawback remains the need of a computer.
There are a number of studies comparing the MDRD to Cockcroft-Gault formula with variable results. Following is the review of some important studies.
MDRD equation provides unbiased and reasonably accurate estimates across wide range of subgroups when GFR is less than 60 i.e. in CKD Stage 3, 4 and 5 [9]. They also proved to be reliable for follow-up in CKD patients in longitudinal studies [10].
MDRD equation performed better than CockcroftGault equation equation in CKD, when GFR was less than 60 ml/min/1.73m2. On the other hand CockcroftGault equation performed better in healthy kidney donors [11]. Cockcroft-Gault equation formula was less precise than MDRD equation in most cases with median GFR of 59.8 ml/ min/1.73m2 [12].
In another study, estimation of GFR in older patients with CKD and mean GFR of 53 ml/min/1.73m2, the Cockcroft-Gault equation was more precise than MDR formula [13]. In diabetic patients MDRD as well as Cockcroft-Gault equation correlated well with isotopic GFR measurements but MDRD equation turned-out to be more accurate [14].
In sick hospitalized patients the performance of MDRD and Cockcroft-Gault equation was compared, using Iodine iothalamate as a control. MDRD equation performed better [15]. MDRD Formula as compare to Cockcroft-Gault formula underestimates GFR in healthy individuals [16].
MDRD formula was more accurate than CockcroftGault equation in ESRD patients. However MDRD formula underestimated GFR when inulin clearance was more than 8 ml/min/1.73m2 and overestimated GFR when inulin clearance was less than 8 ml/min/1.73m2. On the other hand Cockcroft-Gault overestimated GFR when inulin clearance was less than 13 ml/mim/11.73m2 [17].
In patients with CKD but normal serum creatinine, Cockcroft-Gault equation was found to be more accurate than MDRD formula. Measurement of GFR by endogenous and exogenous filtration markers might be the most prudent strategy [18].
5. Conclusion
We conclude that Cockcroft-Gault equation correlates best with MDRD formula at CKD stage 4 and one. Cockcroft-Gault equation overestimated GFR at stages 1, 2, 3. The two formulas may be used interchangeably at stages 4 and 1. Measurement of 24 hour urine creatinine clearance may still be reliable if patients are counseled properly. It is unlikely that MDRD formula will replace Cockcroft-Gault equation in bedside clinical practice soon because the dependency of MDRD formula upon a computer program.
REFERENCES
- T. H. Jafar, C. H. Schmid and A. S. Levey, “Serum Creatinine as Marker of Kidney Function in South Asia: A Study of Reduced GFR in Adults in Pakistan,” Clinical Journal of the American Society of Nephrology, Vol. 16, No. 5, 2005, pp. 1413-1419. doi:10.1681/ASN.2004121100
- G. Eknoyan and N. Levin (Co-Chairs Advisory Board of National Kidney Foundation), et al., “K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification,” American Journal of Kidney Diseases, Vol. 39, No. 5, 2002, pp. S1-S266. doi:10.1016/S0272-6386(02)70054-1
- A. S. Levey, J. P. Bosch, J. B. Levis, T. Greene, N. Rogers and D. Roth, “A More Accurate Method to Estimate Glomerular Filtration Rate from Serum Creatinine: A New Prediction Equation. Modification of Diet in Renal Disease Study Group,” Annals of Internal Medicine, Vol. 130, No. 6, 1999, pp. 461-470.
- D. W. Cockcroft and M. H. Gault, “Prediction of Creatinine Clearance from Serum Creatinine,” Nephron, Vol. 16, No. 1, 1976, pp. 31-41. doi:10.1159/000180580
- G. Rostoker, P. Andrivet, I. Pham, M. Griuncelli and S. Adnot, “A Modified Cockcroft-Gault Formula Taking into Account the Body Surface Area Gives a More Accurate Estimation of the Glomerular Filtration Rate,” Journal of Nephrology, Vol. 20, No. 5, 2007, pp. 576-585.
- A. Schoker, M. A. Hossain, T. Koru-Sengul, D. L. Raju and D. Cockcraft, “Performance of Creatinine Clearance Equation on the Original Cockcraft-Gault Population,” Clinical Nephrology, Vol. 66, No. 2, 2006, pp. 89-97.
- A. S. Levey, J. Coresh, T. Greene, J. Marsh, L. A. Stevens, J. W. Kusek and F. E. Van Lente, “Expressing the Modification of Diet in Renal Disease Study Equation for Estimating GFR with Standardized Serum Creatinine Values,” Clinical Chemistry, Vol. 53, No. 4, 2007, pp. 7666-7672. doi:10.1373/clinchem.2006.077180
- A. S. Levey, J. Coresh, T. Greene, L. A. Stevens, Y. Zhang, S. Hendriksen, et al., “Using Standardized Serum Creatinie Values in the Modification of Diet in Renal Disease Study. Equation for Estimating GFR,” Annals of Internal Medicine, Vol. 145, No. 4, 2006, pp. 247-254.
- L. A. Stevens, J. Coresh, H. I. Feldman, T. Greene, J. P. Lash, R. G. Nelson, et al., “Evaluation of the Modification of Diet in Renal Diease Study Equation in a Large Diverse Population,” Journal of the American Society of Nephrology, Vol. 18, No. 10, 2007, pp. 2749-2757. doi:10.1681/ASN.2007020199
- X. Wang, J. Lewis, L. Appel, D. Cheek, G. Contreras, M. Faulkner, et al., “Validation of Creatinine Based Estimates of GFR When Evaluating Risk Factors in Longitudinal Studies of Kidney Disease,” Journal of the American Society of Nephrology, Vol. 17, No. 10, 2006, pp. 2900-2909. doi:10.1681/ASN.2005101106
- E. D. Poggio, X. Wang, T. Greene, F. Van Lente and P. M. Hall, “Performance of the Modification of Diet in Renal Disease and Cockcroft-Gault Equations in the Estimation of GFR in Health and in Chronic Kidney Disease,” Journal of the American Society of Nephrology, Vol. 16, No. 2, 2005, pp. 459-466. doi:10.1681/ASN.2004060447
- M. Froissart, J. Rossert, E. Jacquot, M. Paillard and P. Houillier, “Predictive Performance of the Modification of Diet in Renal Disease and Cockcroft-Gault Equations for Estimating Renal Function,” Journal of the American Society of Nephrology, Vol. 16, No. 3, 2005, pp. 763-773. doi:10.1681/ASN.2004070549
- E. J. Lamb, M. C. Webb, D. E. Simpson, A. J. Coakley, D. J. Newman and S. E. O’Riordan, “Estimation of GFR in Older Patients with Chronic Renal Insfufficiency: Is the MDRD Formula an Improvement,” Journal of the American Geriatrics Society, Vol. 51, No. 7, 2003, pp. 1012- 1017. doi:10.1046/j.1365-2389.2003.51330.x
- V. Rigalleau, C. Lasseur, C. Perlemonine, N. Barthe, C. Raffaitin and E. Liu, “Estimation of GFR in Diabetics: Cockcroft Formula or MDRD Study Equation,” Diabetes Care, Vol. 28, No. 4, 2005, pp. 838-843. doi:10.2337/diacare.28.4.838
- E. D. Poggio, P. C. Nef, X. Wang, T. Greene, F. Van Lente, V. W. Dennis and P. M. Hall, “Performance of Cockcroft-Gault and Modification of Diet in Renal Disease Equations in Estimating GFR in Ill Hospitalized Patients,” American Journal of Kidney Diseases, Vol. 46, No. 2, 2005, pp. 242-252. doi:10.1053/j.ajkd.2005.04.023
- A. D. Rule, T. S. Larson, E. J. Bergs Tralh, J. M. Slezak, S. J. Jacobsen and F. G. Cosio, “Using Serum Creatinine to Estimate GFR: Accuracy in Good Health and in Chronic Kidney Disease,” Annals of Internal Medicine, Vol. 141, No. 12, 2004, pp. 929-937.
- Y. Kuan, M. Hossain, J. Surman, A. M. El Nahas and J. Haylor, “GFR Prediction Using the MDRD and Cockcroft and Gault Equations in Patients with End Stage Renal Disease,” Nephrology Dialysis Transplantation, Vol. 20, No. 11, 2005, pp. 2394-2401. doi:10.1093/ndt/gfi076
- A. G. Boston, F. Kronenberg and E. Ritz, “Predictive Performance of Renal Function for Patients with Chronic Kidney Disease and Normal Serum Creatinine Levels,” Journal of the American Society of Nephrology, Vol. 13, No. 8, 2002, pp. 2140-2144. doi:10.1097/01.ASN.0000022011.35035.F3
NOTES
*Corresponding author.