Open Journal of Anesthesiology
Vol.3 No.1(2013), Article ID:27623,5 pages DOI:10.4236/ojanes.2013.31006
The Effect of Tramadol on Blood Glucose Levels in Rats
![]()
1Department of Anesthesiology and Reanimation, Dokuz Eylül University Medical School, İzmir, Turkey; 2Department of Pharmacology, Dokuz Eylül University Medical School, İzmir, Turkey; 3Department of Biochemistry, Dokuz Eylül University Medical School, İzmir, Turkey.
Email: *ayse.karci@deu.edu.tr
Received October 20th, 2012; revised November 24th, 2012; accepted December 19th, 2012
Keywords: Hyperglycemia; Tramadol; a2-Antagonist; Antinociceptive Effect; Yohimbine; Idazoxan; Rat
ABSTRACT
The Background: Tramadol, is a central acting analgesic that possesses weak affinity for the µ-opioid receptor and modifies transmission of nociceptive impulses through inhibition of monoamine reuptake. This study was designed to determine the effect of tramadol on blood glucose levels and also to investigate whether or not alpha-2 adrenergic receptors were responsible for this effect. Methods: Twenty-five Wistar male rats were assigned to four groups to receive: Group I: saline; Group II: tramadol (1 mg∙kg−1); Group III and Group IV: pretreatment with a2-receptor antagonist drugs yohimbine (1 mg∙kg−1) or idazoxan (1 mg∙kg−1), 30 min before administration of tramadol (1 mg∙kg−1). Samples for plasma glucose measurement were withdrawn at 0, 30, 60, 90 and 120 minutes of the experiment. Results: A significant rise in blood glucose levels was observed following administration of i.v. tramadol. Pretreatment with both yohimbine and idazoxan (1 mg∙kg−1) significantly attenuated tramadol-induced hyperglycemia. Conclusion: The results of the study indicate that, tramadol administered at an analgesic dose of 1 mg∙kg−1 produces hyperglycemia in diethyl ether anesthetized rats. Reversal of this effect with a2-adrenoceptor blocking agents suggests that monoaminergic pathways which contribute to the analgesic action of tramadol, may have a role in the hyperglycemic action of the drug.
1. Introduction
The central acting, synthetic analgesic tramadol [tramadol hydrochloride is (±) cis-2-[(dimethylamino) methyl]- 1-(3-methoxyphenyl) cyclohexanol hydrochloride] has a low affinity for μ-opioid receptors which may not adequately explain its analgesic and antinociceptive potency and its effects are distinct from those of the pure opioid agonists available in clinical practice [1-3].
Besides the known opioid involvement in modulation of pain, a supraspinal monoaminergic neuronal system that modulates nociceptive processes in the spinal cord has been documented [3]. Experimental data suggests that tramadol may exert part of its analgesic effect through activation of central monoaminergic pathways [3-5]. Additionally, in studies performed to establish a possible involvement of the endogenous adrenergic system, a significant reduction in the antinociceptive effect of tramadol has been demonstrated following pretreatment with the non-selective a2-adrenoceptor antagonist yohimbine [3,4] and selective a2-adrenoceptor antagonist idazoxan [4]. The monoaminergic and opioid systems possess receptors and transmitters located on the same cells and, as shown in receptor blocking studies, the synergistic activity of these two systems achieve an antinociceptive effect [2,4,6-8].
Both adrenaline a mixed adrenergic agonist and clonidine an a2-adrenergic agonist, induce an increase in blood glucose levels through activation of a2-adrenoceptors. The hyperglycemic response to adrenaline in the presence of a1- and b-adrenoceptor blockade indicates that the response is mediated through a2-adrenoceptors [9-11]. Furthermore, Angel et al. [10] have suggested that this hyperglycemic response to adrenaline was in agreement with the pharmacological profile corresponding to a2A-adrenoceptors. Results of previous studies have shown that a2-adrenoceptor induced hyperglycemia was abolished in animals pretreated with a2-adrenoceptor antagonists [10,12,13].
Contribution of monoaminergic transmission to the antinociceptive effects of tramadol and reversal of this effect using a2-adrenergic antagonists suggest that tramadol partly achieves modulation of pain through indirect activation of a2-adrenoceptors. Since several in vitro studies have shown the role of a2-adrenoceptors in induction of hyperglycemia and reversal of this effect by a2-adrenoceptor antagonists we hypothesized that tramadol may cause hyperglycemia mediated through the same pathway. The aim of this study was to investigate 1) the effect of antinociceptive dose of tramadol on blood glucose levels; and 2) the possible role of a2-adrenoceptors in this effect.
2. Material and Method
After approval from the Ethics Committee of Research of Laboratory Animals of Dokuz Eylül University Medical School the study was performed on 25 Wistar male rats.
2.1. Animals
Male rats weighing 200 - 350 g were obtained from the Ege University Medical School Experimental Surgery and Research Laboratories. All animal procedures were performed according to the Guide for the Care and Use of Laboratory Animals of the National Institutes of Health. The rats were allowed to get accustomed to the environment at least 3 days before the start of the experiments. They were kept under standardized conditions of temperature (21˚C - 22˚C) and illumination (12 hours light/12 hours darkness). All rats were kept in cages with mesh bottoms and free access to tap water and pelleted food. The animals were fasted for 12 - 18 hours before the experiment, but had free access to water right up to the beginning of the experiment. All experiments were carried out in a tranquil environment and at the same time period of the day to minimize circadian variations.
2.2. Experimental Design
Rats were assigned to five groups randomly.
Group I (n = 4) received 200 μL saline and this constituted the control group.
Group II (n = 7) received an antinociceptive dose of tramadol (Contramal® Abdi İbrahim, Turkey) (1 mg∙kg−1)
Group III (n = 7) received yohimbine (Sigma Chemical Co, St. Louis, MO), (1 mg∙kg−1) as a2-adrenoceptor antagonist 30 minutes before tramadol administration.
Group IV (n = 7) received selective a2-adrenoceptor antagonist idazoxan (Research Biochemical Inc., Natich, MA), (1 mg∙kg−1) 30 minutes before tramadol administration.
Rats were anesthetized with diethyl-ether inhalation, using a jar containing cotton soaked in diethyl ether. Polyethylene catheters (0.58 mm ID, Portex Ltd., Kent, UK) were inserted into the external jugular vein of each rat for drug administration and in the carotid artery for collecting blood samples. Catheterization and all experimental procedures were performed under diethyl-ether anesthesia.
Control samples for basal measurement of blood glucose levels were taken at the beginning of the experiment before injection of the study drug or the α-adrenoceptor blocking agents at the doses indicated. Blood samples were withdrawn into heparinized tubes at 30, 60, 90, and 120 minutes after administration of the drugs. Following each blood sample withdrawal, cannulae were flushed with saline (0.9%) containing heparin (100 U ml−1). Plasma glucose levels were measured by means of the glucose oxidase method (Roche Diagnostic, Germany) using a Hitachi (P-800, Japan) automated analyzer at the end of each experiment.
2.3. Drugs
Yohimbine and idazoxan were immediately dissolved in saline (0.9%) before use. The source of the drugs used were as follows: Tramadol HCL (ContramalÒ, Abdi İbrahim, Turkey), Yohimbine HCL (Sigma Chemical Co., St. Louis, MO), Idazoxan HCl (Research Biochemical Inc., Natich, MA).
2.4. Statistical Analysis
Statistical analyses were performed using SPSS 11.0 for Windows. All data are expressed as mean ± Standard Deviation (SD). Kruskal-Wallis variance analysis was used to compare differences between groups; paired comparisons were performed using the Mann Whitney U test to find out which group caused the difference. Wilcoxon Rank-Sum test was used to compare the periods in the same group. A value of p < 0.05 was considered statistically significant for all analyses.
3. Results
3.1. Effect of Tramadol on Blood Plasma Levels in Rats
Normal saline administered to rats in group I did not cause a change in plasma glucose levels compared to basal values. An elevation in plasma glucose levels was observed 30 minutes following administration of i.v tramadol 1 mg∙kg−1 to anesthetized rats. The increase in plasma glucose levels was observed to be statistically significant when compared with basal values at all periods (p < 0.05). Plasma glucose levels gradually increased from 121.86 ± 11.73 mg/dL (basal values) to 200.71 ± 36.00 mg/dL till the end of the investigation in Group II. The hyperglycemic response persisted at 120 minutes following administration of tramadol. Plasma glucose levels of all groups are shown in Figure 1.
3.2. The Effect of Tramadol (1 mg∙kg−1) on Plasma Glucose Levels in Rats Pretreated with (2-Antagonist Yohimbine
In group III, the non-selective a2-antagonist yohimbine 1 mg∙kg−1 did not cause a change in plasma glucose levels in 30 minutes compared to basal values (107.71 ± 22.01
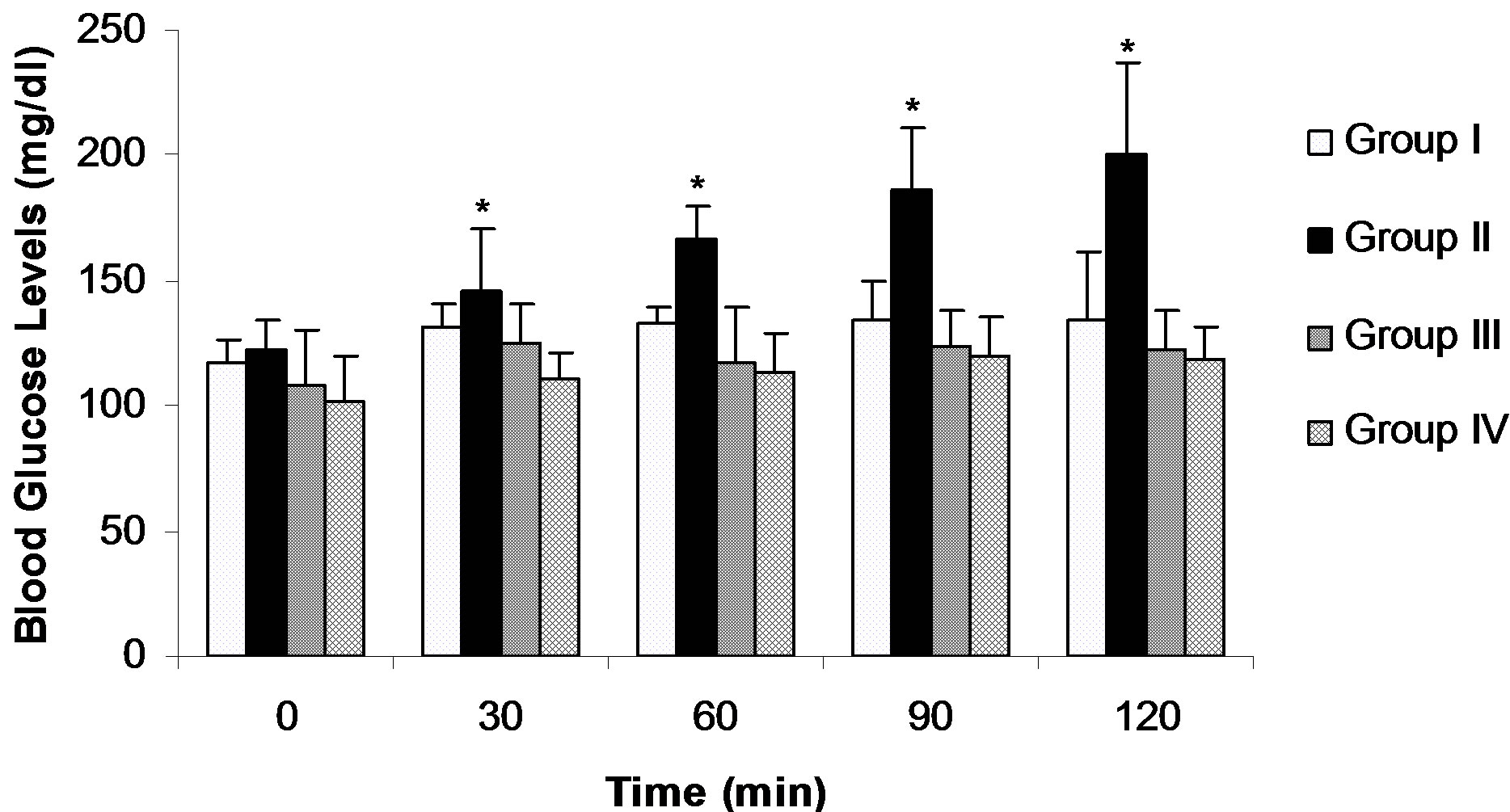
Figure 1. Effect of tramadol on blood glucose levels in normal and yohimbine and idazoxan pretreated rats. Data are the mean ± SD. *p < 0.05 comparison between groups.
mg/dL and 116.75 ± 9.84 mg/dL; respectively). Pretreatment with yohimbine caused a suppression of the hyperglycemic response to tramadol 1 mg∙kg−1 throughout the study period. The difference in plasma glucose levels between yohimbine pretreated rats and rats receiving only tramadol were insignificant at 30 minutes (125.00 ± 15.92 mg/dL versus 145.71 ± 24.93 mg/dL). Plasma glucose levels were significantly lower in yohimbine pretreated rats compared to Group II at 60, 90 and 120 minutes (p < 0.005). Additionally glycemia levels in yohimbine pretreated rats were not significantly different from basal values at any measurement (p > 0.05) (Figure 1).
3.3. The Effect of Tramadol (1 mg∙kg−1) on Plasma Glucose Levels in Rats Pretreated with Selective (2-Antagonist Idazoxan
Plasma glucose levels did not show a significant difference from basal values in 30 minutes following administration of 1 mg∙kg−1 idazoxan (102.14 ± 17.77 mg/dL and 116.75 ± 9.84 mg/dL; respectively) (p > 0.05). This selective α2-antagonist, when given as pretreatment, suppressed the hyperglycemic response of the rats to tramadol, this effect was significantly different within 30 minutes of administration of tramadol. The significant difference in plasma glucose levels persisted at all time periods following administration of tramadol (p < 0.005) (Figure 1). Conversely, there was no significant difference in plasma glucose levels in rats which were pretreated with idazoxan and the group receiving only saline (102.14 ± 17.77 mg/dL versus 116.75 ± 9.84 mg/dL at 0 min; 111.00 ± 10.39 mg/dL versus 131.50 ± 8.54 at 30 min; 113.00 ± 16.04 mg/dL versus 132.50 ± 6.60 mg/dL at 60 min; 120.29 ± 14.60 mg/dL versus 134.75 ± 14.56 mg/dL at 90 min; and 118.00 ± 13.86 mg/dL versus 134.75 ± 26.39 mg/dL at 120 min).
4. Discussion
The results of this present study have shown that, tramadol hydrochloride; administered at an antinociceptive dose of 1 mg∙kg−1 induce a significant hyperglycemic response in normal fasted rats. Induction of hyperglycemia with this drug and blockade of this effect with both yohimbine and idazoxan may represent the activity of a a2-adrenoceptors in this effect on blood glucose levels.
In the current study the dose chosen (1 mg∙kg−1) to test the effect of tramadol on blood glucose levels was proposed to have potent antinociceptive effect in rats by Kayser et al. [4] Additionally, Raffa et al. [8] have demonstrated that the antinociceptive dose of tramadol in rats was in the range of 0.7 - 3.2 mg/kg. Thus this dose of tramadol has been widely used as an analgesic in experimental and clinical studies [14,15]; but its effect on blood glucose levels has not been investigated extensively.
Cheng et al. [16] reported a dose-dependent lowering of plasma glucose in the fasting streptozotocin (STZ)- induced diabetic rats after intravenous injection of tramadol 50 µg∙kg−1. They reported that plasma glucose lowering effect of tramadol was mediated by activation of opioid µ-receptors and was abolished by pretreatment with naloxone at doses sufficient to block opioid µ-receptors. According to their results activation of opioid receptors by tramadol could increase the utilization of glucose in peripheral tissues. However, no change in plasma glucose levels was found in normal rats receiving a similar injection of tramadol at the same dose.
Contrary to these results, we demonstrated a significant increase in plasma glucose levels following administration of tramadol 1 mg∙kg−1. There were two main methodological differences between these two investigations: first the dose they used was much lower than the one we used (50 µg∙kg−1 versus 1 mg∙kg−1). This dose had different effects in streptozotocin-induced diabetic rats and normal rats. Second, Cheng et al. used STZ-induced diabetic rats, whereas the rats in our study were not diabetized and had normal glycemia levels at the beginning of the experiment. Angel et al. [10] who studied the involvement of the pancreatic b-cells in hyperglycemic response to selective a2-adrenoceptor agonist UK 14,304 in rats treated with STZ, suggested that integrity of these cells is necessary for the induction of hyperglycemia by the a2-adrenoceptor agonist. Thus, in addition to difference in tramadol dose, destruction of pancreatic b-cells due to streptozocin in Cheng’s [16] study may explain the discrepancy in the results of the two experiments.
The physiological effect of catecholamines on insulin secretion appears to depend on a balance between stimulation mediated by β-adrenoceptors and an inhibition through α-adrenoceptor activation [9,12]. John et al. [12] showed that adrenaline-induced hyperglycemia was abolished by idazoxan and unaffected by propranolol in fasted normal rats. They also demonstrated that the selective a2-adrenoceptor agonist UK 14,304 elicited dosedependent hyperglycemic responses and this effect was blocked by idazoxan but not a1-adrenoceptor antagonist prazosin. Similarly Moratinos et al. [9] showed that infusions of a2-adrenoceptor antagonist inhibited the increase in blood glucose in rabbits induced by adrenaline or phenylephrine. Furthermore, Angel et al. [10] demonstrated that rats receiving prazosin and propranolol showed a significant hyperglycemic response to adrenaline. Thus, hyperglycemic response to adrenaline in the presence of a1- and β-adrenoceptor blockade and inhibition of this response by a2-adrenoceptor antagonists, indicate that the response is specifically mediated by a2- adrenoceptors in fasted rats [10,12,13].
In this study we used a2-antagonists, which were effective in both antagonizing hyperglycemic response to a2-adrenoceptor agonists and the antinociceptive effect of tramadol, to further evaluate the effect of tramadol on plasma glucose levels. In previous studies it is clearly reported that both a2-adrenoceptor antagonists idazoxan [10,12] and yohimbine [17] at 1 mg∙kg−1 doses caused no significant changes in basal plasma glucose levels. In agreement with these studies in the present study, administration of 1 mg∙kg−1 idazoxan and yohimbine 30 minutes before tramadol (1 mg∙kg−1) did not cause a significant change in blood glucose levels compared to basal values. Using yohimbine and idazoxan at the same doses others used to inhibit the hyperglycemic response to a2-adrenoceptor agonists we demonstrated that the hyperglycemic effects of tramadol in fasted rats were significantly diminished.
The dose of the antagonists and time interval before administration of tramadol were similar to studies investtigating the antinociceptive activity of tramadol and hyperglycemic effect of a2-adrenoceptor agonists. Kayser et al. [4] administered yohimbine and idazoxan in 0.5 - 1.0 mg∙kg−1 doses to investigate the noradrenergic component in the antinociceptive action of tramadol. They injected tramadol 30 minutes following each of the antagonists and showed a decrease in the antinociception. In studies investigating the hyperglycemic effects of the a2-adrenoceptor agonists such as adrenaline, UK 14,304 or phenilephrine, the a2-adrenoceptor antagonists were injected 20 - 40 minutes before injection of the agonists [10,11]. They reported abolishment of the hyperglycemic effect in 30 minutes. Thus we injected yohimbine or idazoxan 30 minutes before tramadol, which was the time period used both to antagonize antinociceptive and hyperglycemic effects of different drugs. The hyperglycemic effect of tramadol was not observed in rats receiving yohimbine and idozoxan, thus the antagonistic effect was evident in 30 minutes.
Both a2-antagonists having receptor selectivity for a2-adrenoceptor subtypes blocked the hyperglycemic response to tramadol and this effect remained till the end of the experiment. The effect was evident in 30 minutes similar to other studies investigating the effect of a2- adrenoceptor agonists on blood glucose levels. It was observed that the blockade of the hyperglycemic effect was inhibited earlier in rats receiving pretreatment with idazoxan. There is not enough evidence for the onset of action of the two antagonists; but Angel et al. [11] reported that idazoxan was 3- to 6-fold more potent on the a2A-site compared to the a2B-site the adrenoceptors. Perhaps the selectivity and potency of the drug for the a2A-adrenoceptors may explain the difference between the two antagonists.
In conclusion, we demonstrated an increase in blood glucose levels with an antinociceptive dose of tramadol and also inhibition of the plasma glucose increasing action of tramadol with a2-adrenoceptor antagonists yohimbine and idazoxan in fasted rats. The results of the present study provide evidence that monoaminergic activity responsible from the antinociceptive effect of tramadol could also play a role in the hyperglycemic response to an antinociceptive dose of the drug.
REFERENCES
- E. A. Shipton, “Tramadol—Present and Future,” Anaesthesia and Intensive Care, Vol. 28, No. 4, 2000, pp. 363- 374.
- D. J. R. Duthie, “Remifentanil and Tramadol,” British Journal of Anaesthesia, Vol. 81, No. 1, 1998, pp. 51-57. doi:10.1093/bja/81.1.51
- J. A. Desmeules, V. Piguet, L. Collart and P. Dayer, “Contribution of Monoaminergic Modulation to the Analgesic Effect of Tramadol,” British Journal of Clinical Pharmacology, Vol. 41, No. 1, 1996, pp. 7-12. doi:10.1111/j.1365-2125.1996.tb00152.x
- V. Kayser, G. Guilbaud and J. M. Besson, “Potent Antinociceptive Effects of Clonidine Systemically Administered in an Experimental Model of Clinical Pain, the Arthritic Rat,” Brain Research, Vol. 593, No. 1, 1992, pp. 7-13. doi:10.1016/0006-8993(92)91255-D
- B. Driessen and W. Reimann, “Interaction of the Central Analgesic, Tramadol, with the Uptake and Release of 5-Hydroxytryptamine in the Rat Brain in Vitro,” British Journal of Pharmacology, Vol. 105, No. 1, 1992, pp. 147- 151. doi:10.1111/j.1476-5381.1992.tb14226.x
- B. C. Bloor, M. Maze and I. Segal, “Interaction between Adrenergic and Opioid Pathways,” In: F. G. Estafanous, Ed., Opioids in Anesthesia II, Reed Publishing, Stoneham, 1991, pp. 35-45.
- K. A. Eggers and I. Power, “Tramadol,” British Journal of Anaesthesia, Vol. 74, No. 3, 1995, pp. 247-249. doi:10.1093/bja/74.3.247
- R. B. Raffa, E. Friderichs, W. Reimann, R. P. Shank, E. E. Codd and J. L. Vaught, “Opioid and Nonopioid Components Independently Contribute to the Mechanism of Action of Tramadol, an ‘Atypical’ Opioid Analgesic,” Journal of Pharmacology and Experimental Therapeutics, Vol. 260, No. 1, 1992, pp. 275-285.
- J. Moratinos, B. Olmedilla, I. de Pablos and M. D. Vigueras, “Alpha-Adrenoceptor Involvement in Catecholamine-Induced Hyperglycaemia in Conscious Fasted Rabbits,” British Journal of Pharmacology, Vol. 89, No. 1, 1986, pp. 55-66. doi:10.1111/j.1476-5381.1986.tb11120.x
- I. Angel and S. Z. Langer, “Adrenergic-Induced Hyperglycemia in Anaesthetized Rats: Involvement of Peripheral Alpha 2-Adrenoceptors,” European Journal of Pharmacology, Vol. 154, No. 2, 1988, pp. 191-196. doi:10.1016/0014-2999(88)90097-0
- I. Angel, R. Niddam and S. Z. Langer, “Involvement of Alpha-2 Adrenergic Receptor Subtypes in Hyperglycemia,” Journal of Pharmacology and Experimental Therapeutics, Vol. 254, No. 3, 1990, pp. 877-882.
- G. W. John, J. C. Doxey, D. S. Walter and J. L. Reid, “The Role of Alphaand Beta-Adrenoceptor Subtypes in Mediating the Effects of Catecholamines on Fasting Glucose and Insulin Concentrations in the Rat,” British Journal of Pharmacology, Vol. 100, No. 4, 1990, pp. 699-704. doi:10.1111/j.1476-5381.1990.tb14078.x
- R. Niddam, I. Angel, S. Bidet and S. Z. Langer, “Pharmacological Characterization of Alpha-2 Adrenergic Receptor Subtype Involved in the Release of Insulin from Isolated Rat Pancreatic Islets,” Journal of Pharmacology and Experimental Therapeutics, Vol. 254, No. 3, 1990, pp. 883-887.
- K. Budd, “The Role of Tramadol in Acute Pain Management,” Acute Pain, Vol. 2, No. 4, 1999, pp. 189-196. doi:10.1016/S1366-0071(99)80019-9
- M. D. Vickers, D. O’Flaherty, S. M. Szekely, M. Read and J. Yoshizumi, “Tramadol: Pain Relief by an Opioid without Depression of Respiration,” Anaesthesia, Vol. 47, No. 4, 1992, pp. 291-296. doi:10.1111/j.1365-2044.1992.tb02166.x
- J. T. Cheng, I. M. Liu, T. C. Chi, T. F. Tzeng, F. H. Lu and C. J. Chang, “Plasma Glucose-Lowering Effect of Tramadol in Streptozotocin-İnduced Diabetic Rats,” Diabetes, Vol. 50, No. 12, 2001, pp. 2815-2821. doi:10.2337/diabetes.50.12.2815
- H. A. Abouazra and S. I. Sharif, “Hyperglycaemia: A Morphine-Like Effect Produced by Naloxone,” Clinical and Experimental Pharmacology and Physiology, Vol. 28, No. 4, 2001, pp. 300-305. doi:10.1046/j.1440-1681.2001.03442.x
NOTES
*Corresponding author.