Open Journal of Therapy and Rehabilitation
Vol.2 No.1(2014), Article ID:42923,8 pages DOI:10.4236/ojtr.2014.21006
Benefits of laptop computer ergonomics education to graduate students
![]()
Division of Occupational Therapy, College of Health Professions, Medical University of South Carolina, Charleston, USA; *Corresponding Author: bowmanpj@musc.edu
Copyright © 2014 Peter J. Bowman et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In accordance of the Creative Commons Attribution License all Copyrights © 2014 are reserved for SCIRP and the owner of the intellectual property Peter J. Bowman et al. All Copyright © 2014 are guarded by law and by SCIRP as a guardian.
Received 19 December 2013; revised 21 January 2014; accepted 29 January 2014
KEYWORDS
Laptop; Ergonomics; Education; Posture
ABSTRACT
Laptop computers are used more often than desktop computers, especially among graduate students. Many common laptop habits can have severe physiological effects on the user ranging from eye strain, poor posture, upper extremity pain, and overuse injuries. Thus, it is important to educate students on the best ergonomic position to use laptops. This study investigates the efficacy of a laptop ergonomic education session and its effects on graduate students’ knowledge and behaviors regarding proper laptop use. A convenience sample of control and experimental groups was used and consisted of 83 occupational therapy (OT), 63 physical therapy (PT), and 26 nurse anesthesia (NA) graduate students. The sample size was 172, with 94 graduate students in the control group and 78 graduate students in the experimental. All study participants completed an initial ergonomics questionnaire. The experimental group was given an ergonomics education session following the questionnaire. Approximately 4 weeks after both groups completed the initial questionnaire; a follow up questionnaire was administered. Results showed that subjects demonstrated a statistically significant improvement in ergonomics knowledge after they completed the ergonomic educational session. Some participants reported making adaptations to laptop positioning and equipment use following the educational session. Thus, participating in ergonomic education can positively influence awareness of body mechanics relative to laptop workstation design.
1. INTRODUCTION
In the last decade, computer usage has shifted from desktops to laptops, especially among college and graduate students. Jacobs et al. [1] report that laptop sales comprise at least a quarter of the overall computer market, with these numbers jumping to 75.8% among college and graduate students. Such an increase in laptop use has sparked research on usage revealing that many common laptop habits can have severe physiological effects ranging from eye strain, poor posture, upper extremity pain, and other injuries resulting from overuse. However, students, even those in an allied health science university, are often unaware of the negative consequences that can result from lack of ergonomic knowledge.
Previous studies established that preventative education is a possible solution for minimizing the occurrence of such musculoskeletal disorders in accordance with laptop use. However, while some researchers have studied the effect of ergonomic education on desktop computer use, research is lacking on the efficacy of this type of instruction on laptop use. Research on the ergonomic effects of laptop use is essential because of their popularity. Current and future health care professionals must contribute to such research because these providers will potentially treat such ailments, and they must be able to assess, teach and model proper ergonomics use. Educating this population is important because health care professionals will potentially be treating such ailments and modeling proper ergonomic use. Ergonomic education that addresses correct posture, work station design, and work habits has been shown to prevent injury and promote healthy computing habits.
Previous studies [1-3] found notable ergonomic improvements in participants following such ergonomic educational sessions. Subjects reported increased awareness and decreased musculoskeletal problems during laptop use.
Moffet et al. [4] conducted a study to determine the cause of musculoskeletal pain related to laptop use and found positioning a laptop on a desktop resulted in less head flexion and backwards trunk inclination and more upper arm elevation. When the laptop was positioned in the subject’s lap, an increase in discomfort in the neck and shoulder regions was reported. Both laptop positions resulted in high muscle load levels in the trapezius and deltoid muscles.
Berkhout et al. [5] studied the effect of load on the neck using a laptop compared to a laptop in a laptop docking station in 10 males with no report of preexisting musculoskeletal complaints and found that laptop docking stations resulted in an improvement in work productivity, decrease torque in C7-T1, and less strain on the neck.
The purpose of this study is to investigate the efficacy and effect of laptop ergonomic education on graduate students’ knowledge and behaviors regarding proper laptop use. The educational sessions were designed to address specific objectives aimed at laptop trends among an allied health student population in order to increase students’ awareness of their current laptop habits and evoke a beneficial change to minimize injury risk.
2. LITERATURE REVIEW
Hamilton, Jacobs, and Orsmond [6] found that 82% of the 72 college-aged subjects in their study used a computer up to 6 hours a day, with 11% using a computer more than 8 hours a day. Data analysis from self-reported questionnaires revealed that laptop computers are associated with a higher rate of musculoskeletal complaints, with 90.1% of laptop users reporting discomfort versus 80.6% among desktop users.
Moras [7] conducted a study to determine the consequences of a university-wide laptop program and its ergonomic impact, focusing on musculoskeletal discomfort in fingers, hands, arms, shoulders, neck, and back. A survey was administered to a random-cross section of 361 undergraduate students at the beginning of each class to assess levels of discomfort, previous laptop use, major and non-musculoskeletal problems such as eye pain and headaches. Neck pain was the most common complaint, followed by upper and lower back.
The Bureau of Labor Statistics [8] reported that 34% of all work-related injuries resulting in 1 or more days away from work were musculoskeletal disorders. Bohr [2] confirms these findings stating that though reconfiguring the design of a work site might be the most effective form of injury prevention, it is often impossible due to financial constraints.
Though research has determined that ergonomic education relative to laptop use among students is effective in improving their understanding of postural and physiologic needs, Williams and Jacobs [7] noted that an increase in knowledge and awareness of practice does not necessarily translate into a reduction in risk behavior.
Bohr [2], therefore, designed a study to determine the efficacy of such prevention programs in 154 reservation employees at an international transportation company. A control group received no education while an education group received a one-hour ergonomic information session consisting of lecture and handouts. A participatory education group received similar information in the form of active participation discussion and problem-solving tasks, as well as opportunities to problem solve ergonomic issues in their own workstations. In post-intervention surveys, participants in the educational groups reported less upper extremity pain and work stress than the control group and further reported an increased sense of general well-being, with no differences in the two educational groups.
A similar study conducted by Gravina et al. [3], using a single-subject, multiple baseline design with five participants found that ergonomic education paired with workstation and behavioral adjustment improved employees’ body awareness and correct ergonomic posture when seated at their workstation. An inter-professional team of “behavioral-based safety specialists” and an occupational therapist provided employees with an ergonomic evaluation, particularly noting the percentage of time employees assumed correct body posture in their office. The study included workstation adaptations following baseline, peer observations, and graphic feedback to assess improvements in an employee’s safety behavior. Results indicate that ergonomic education paired with workstation and behavioral adaptation contributes to improvements in correct body posture, educational ergonomics should include evaluation of workstation and behavioral adaptation.
Despite ergonomic evidence, cumulative trauma disorders remain common among laptop users. Shinn et al. [9] suggested a possible solution by advocating preventative education. Their data were collected during 9 inservice sessions over 2 days highlighting proper body mechanics and ergonomics for computer workstations in 117 middle-school students. The in-service sessions included lectures and demonstrations of adaptive techniques, stretching methods, and rest periods. Preand post-questionnaires were distributed to students and an environmental checklist was implemented, noting heights and distances of objects at the workstation. Results indicated a statistically significant difference between preand post-test scores following ergonomic educational in-services, further evidence for offering interactive, preventative education in the classroom: as well as implementing of preand post-tests.
Sotoyama et al. [10] sent questionnaires to 100 elementary, junior high, and high schools, asking how often and in what environment computers are used, whether any instructions are given for their use, the children’s working posture, and the effect on their overall health. They found most schools are slow in developing instructive programs about environment and ergonomics in relation to the computer workspace. Although children currently were not experiencing musculoskeletal problems, a concern for future problems with the prospected rise in use of computers in the classroom was expressed. This rise in computer use can lead to physical problems if measures are not taken to improve ergonomic positioning.
Ketola et al. [11] examined the effect of an intensive ergonomic education on workstation changes and musculoskeletal disorders among 124 subjects who were evaluated using questionnaires, diaries of discomfort, measurements of workload, and ergonomic ratings of workstations. The intensive ergonomics group used an ergonomic checklist to customize the layout and environment of their work areas and tracked recommended rest breaks throughout the day. The ergonomic education groups attended a 1-hour training session in addition to using the checklist and were encouraged to evaluate their workstations and implement changes. In a third group, subjects were supplied with a short educational reference along with a take-home handout. Results showed that ergonomics education helped reduce discomfort; however, the best results were achieved by cooperative planning in which both workers and practitioners were involved.
3. METHODS
A convenience sample of control and participant groups with 83 occupational therapy (OT), 63 physical therapy (PT), and 26 nurse anesthesia (NA) graduate students participated. The Institutional Review board approved this research as exempt. All study participants used laptop computers for classroom and laboratory activities on tables and plinths, in an on campus location. The classrooms were not specially adapted in any way. The participants answered an initial ergonomics questionnaire (see Figures 1(a) and (b)), with 7 multiple choice questions, 2 true/false questions, and 7 pictures in which participants identified “good” or “bad” ergonomic laptop computer positioning. The questionnaire assessed participant knowledge about viewing distance and positioning, as well as frequency of rest and eye breaks. Questions included the correct head, neck, elbow, and back positioning when using a laptop and hand movements and wrist placement relative to the keyboard.
The control group was administered an initial ergonomics questionnaire without an ergonomics educational session (see Figure 1(a)). The experimental group was then given an ergonomics education session that consisted of a PowerPoint presentation, a final review, and an educational handout with the same content (see Figure 1(b)). The educational session defined ergonomics; correct individual positioning when using a laptop computer; equipment that can be used and adaptations (such as a foot rest, adjustable chair, laptop stands, and a separate keyboard) that can be made to help achieve the ideal position; frequency of eye breaks; some eye exercises; and frequency of rest breaks.
Four weeks after the initial questionnaire was completed and an educational session provided for the participant group, both groups completed a follow-up questionnaire. This questionnaire for the control group consisted of the same 16 questions from the initial questionnaire (see Figure 1(b)), as well as 9 additional questions asking about any changes participants made with regards to laptop use positioning and frequency of breaks since the initial questionnaire. The questionnaire asked if students had improved their ergonomic positioning as a result of the initial questionnaire; if they were more aware of body mechanics and their positioning; if they had purchased any computer accessories to improve their ergonomics; and if they had begun taking breaks and, if so, which kind (eye, rest, exercise, and micro). One question listed 12 body parts such as head and feet and asked students to place a check next to the body part they had modified or adjusted. The final 2 questions asked participants to rate their laptop computer ergonomics’ use prior to and after the initial questionnaire on a 0 - 10 scale with “0” being the “least ergonomically correct” and “10” being the “most ergonomically correct”.
The follow-up questionnaire for the participant group consisted of the same 16 questions from the initial questionnaire (see Figure 1(b)) as well as the 9 additional questions. This questionnaire, however, asked about changes made since the education session instead of the initial questionnaire. All initial and follow-up questionnaires were assessed for changes in knowledge and behavior to quantify specific ergonomic behaviors and positional changes.
4. RESULTS
The survey data were analyzed by a paired t-test for equality of means including an independent samples test and analysis using ANOVA. The ANOVA was used to show changes/improvements in knowledge following the ergonomic educational session. No significant differences
 (a)
(a)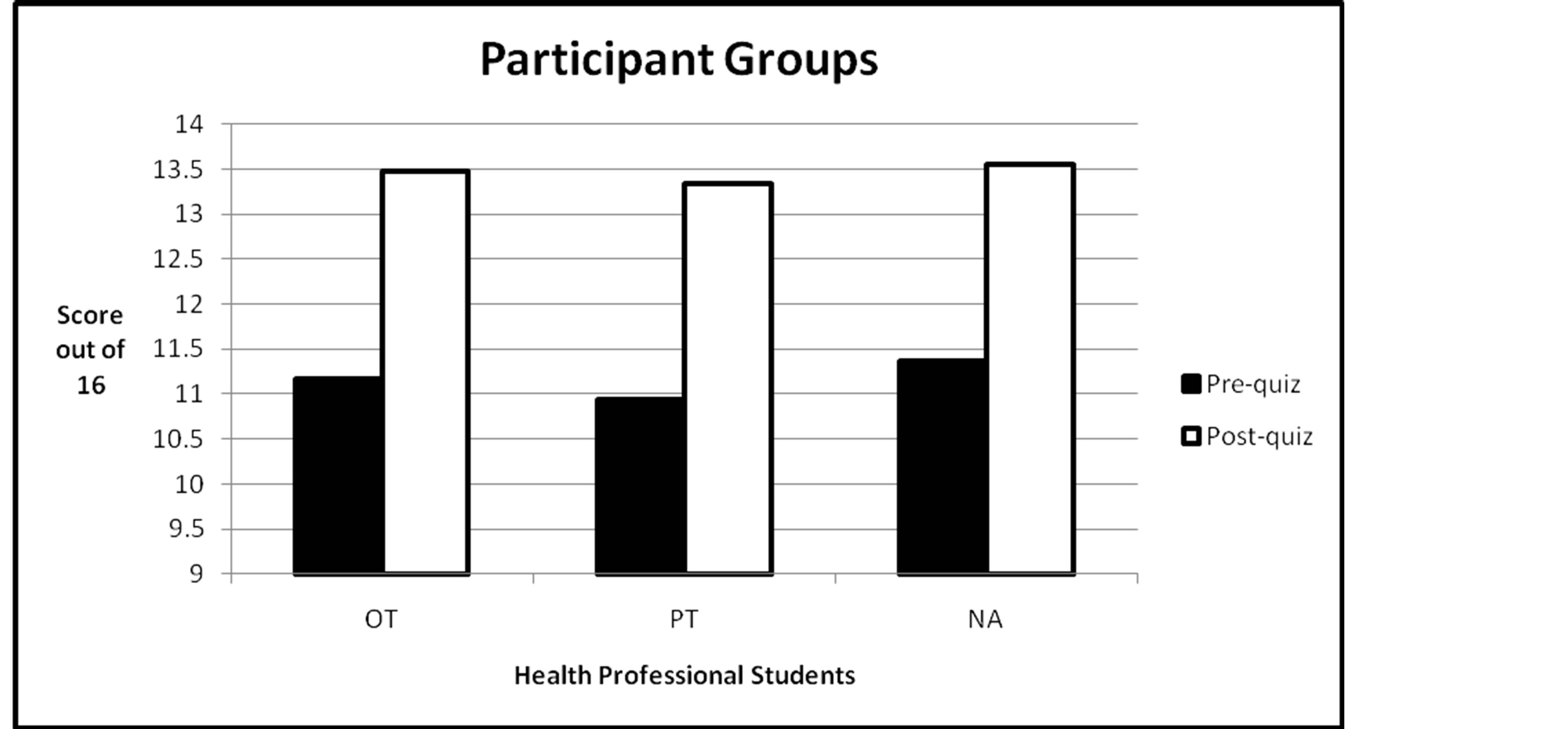 (b)
(b)
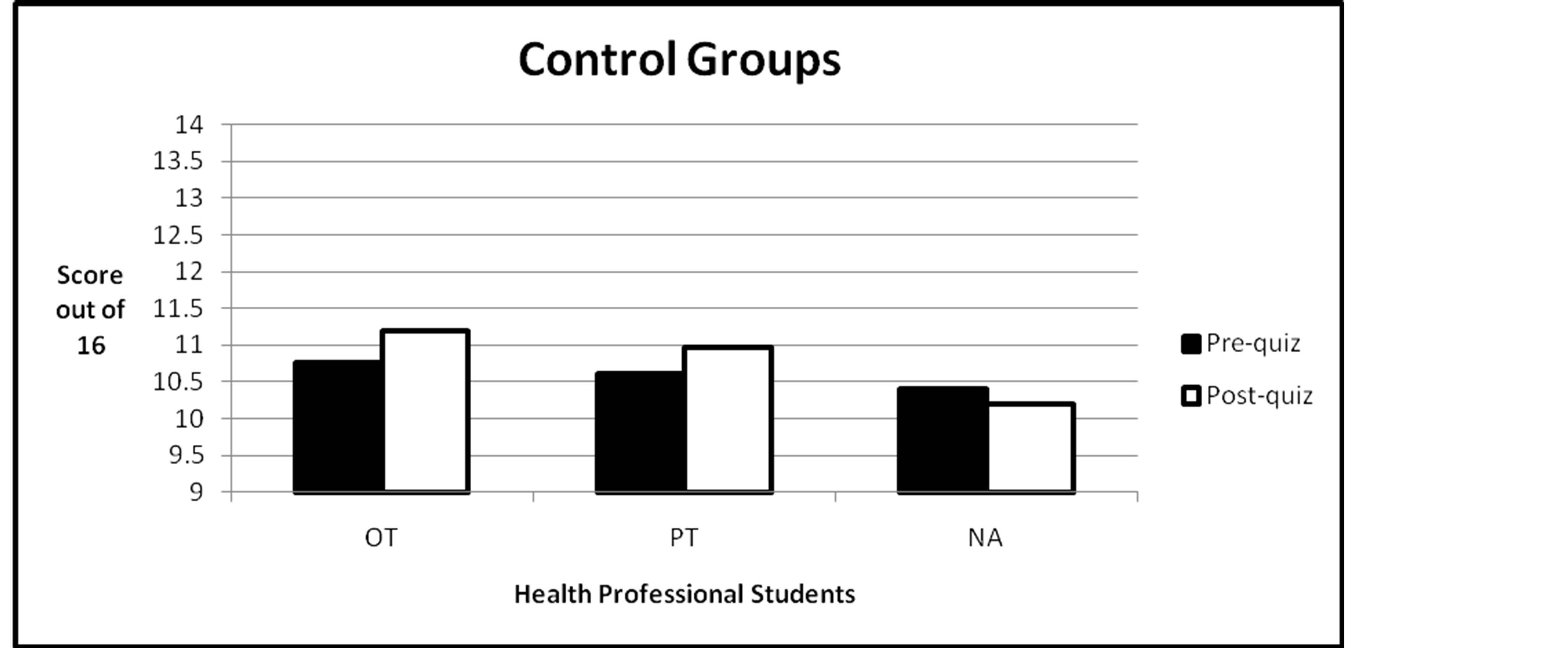
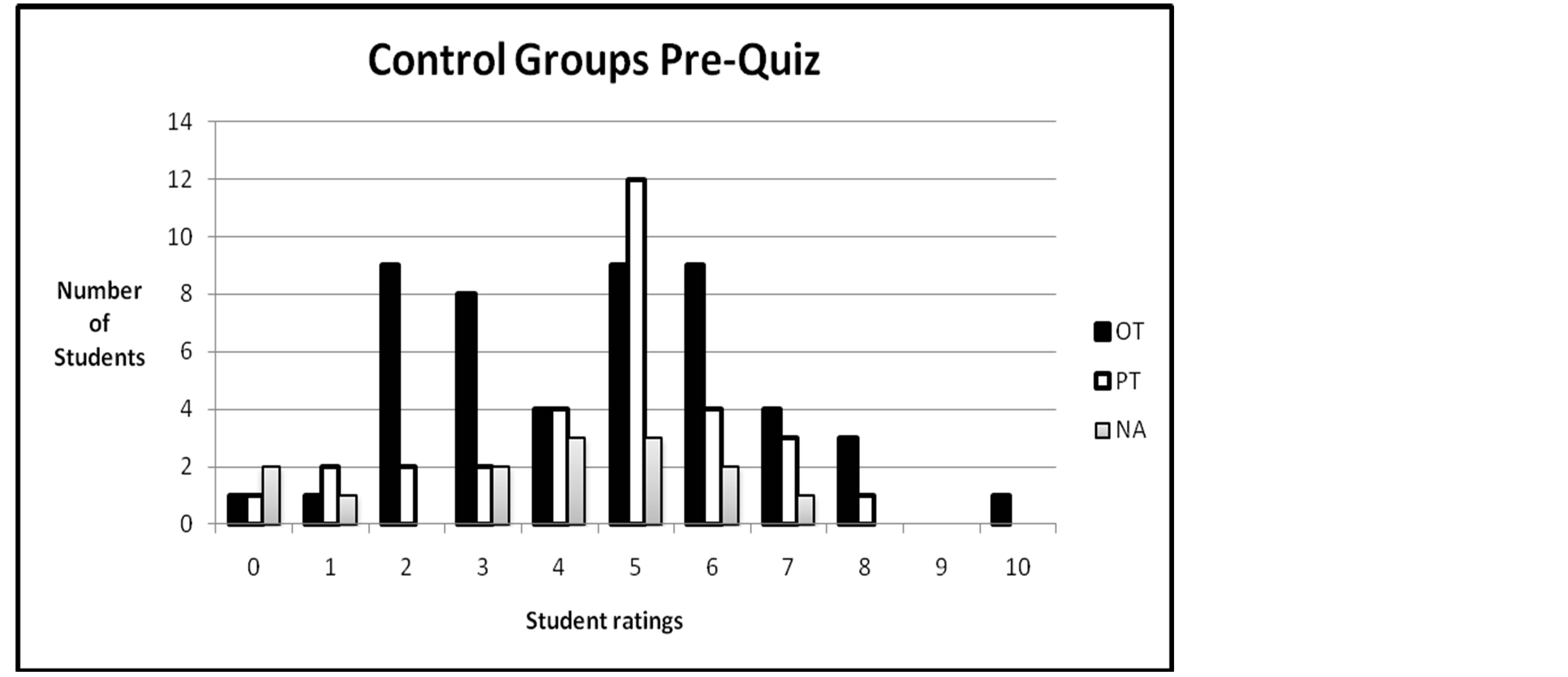
Figure 1. (a) The number of multiple choice questions answered correctly on the pre-/post-ergonomic quiz for the control groups of all health professional students; (b) The number of multiple choice questions answered correctly on the pre-/post-ergonomic quiz for the participant groups of all health professional students.
were identified among OT, PT, and NA students (see Figure 1(b)). These results suggest that there is high rate of inter-subject reliability that is not dependent on the specific health profession.
The two-tailed t-test compared the control groups and participant groups among all subjects on the change and/ or improvement in knowledge about ergonomics. The results showed that participants demonstrated significant improvement in knowledge on ergonomics after they had completed the ergonomic educational session. A significant difference, where p < 0.01, was found in comparing pre-test and post-test scores among all subjects with the results of p = 0.00.
Table 1 shows the mean differences in scores between the initial questionnaire and follow up questionnaire responses for the Occupation Therapy (OT), Physical Therapy (PT) and Nurse Anesthesia (NA) students as either control group members, who did not receive an educational session and participants who did receive additional education.
The data were analyzed for the three different health professional students (OT = 83, PT = 63, NA = 26) (see Figures 1(a) and (b) Pre Quiz). All participant groups demonstrated a significant improvement in ergonomic knowledge after completing the ergonomic educational session (see Figures 1(a) and (b) Post Quiz).
Results of the 0 - 10 scale rating from the least ergonomically correct to the most ergonomically correct ways of using laptop computers are shown in Figures 2(a)-(d) and Table 2. This shows the number of students
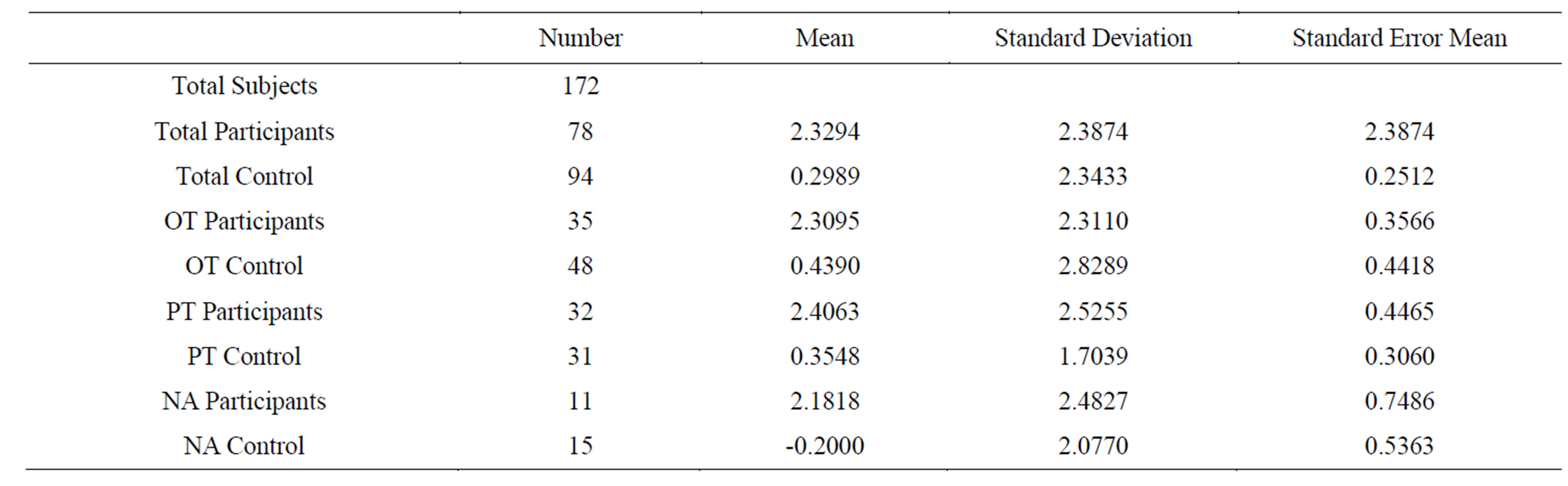
Table 1. Mean for score changes between first and second questionnaire administration for participants and control groups.
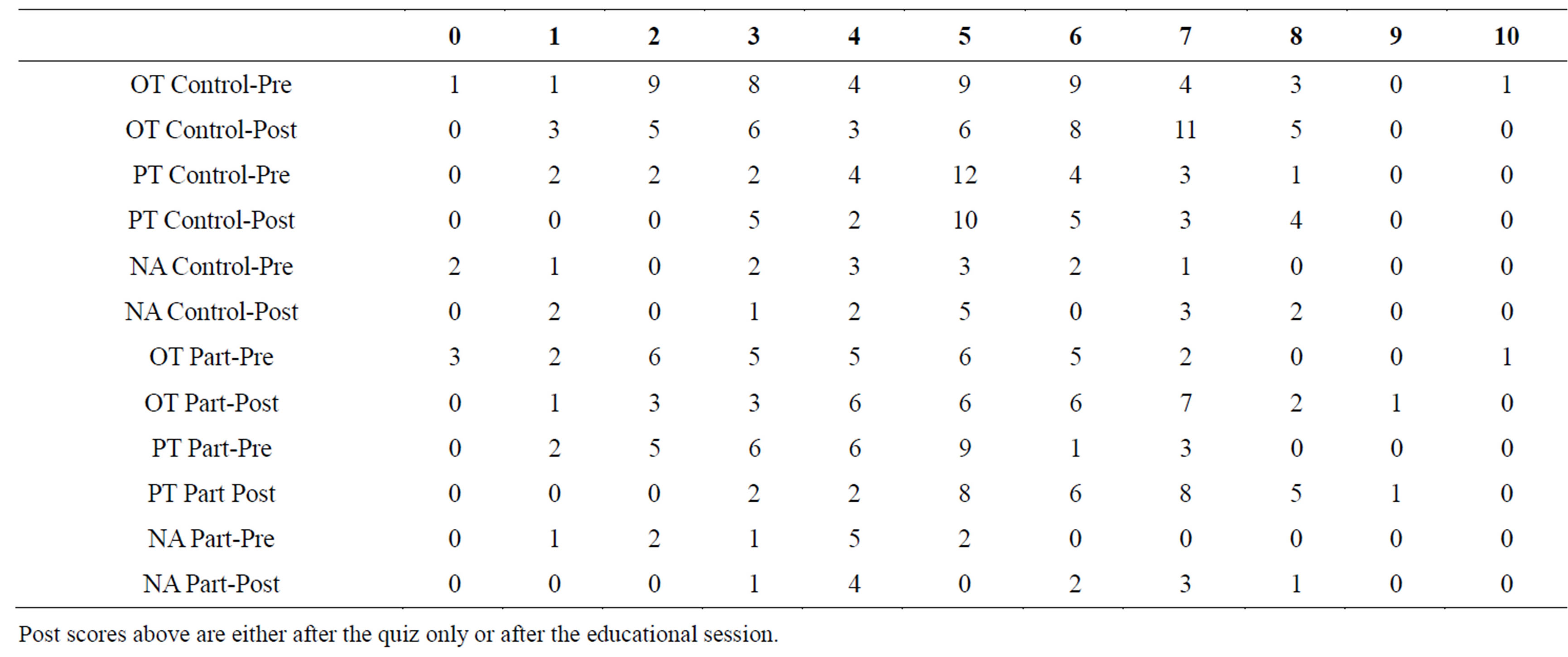
Table 2. Pre and post student ratings of perceived ergonomic laptop use, prior to (pre) and after the second quiz (post). Using a scale of 0 (least ergonomically correct laptop use) to 10 (most ergonomically correct).
from each discipline and how they rated their ergonomic laptop use prior to the quiz and after the educational session for the participation group and after the second quiz for the control group. The participant group reported an increase in rating on the 0 - 10 scale, indicating that they felt they were using more ergonomically appropriate laptop computer methods.
After the ergonomic educational session, the participant group responded to open-ended questions. Four OT students have made changes in their study area at home. Six OT and PT students reported that they had peer conversations and individually researched the internet on the topic of proper laptop ergonomics. Twenty one % of OT, 59% of PT, and 55% of NA stated they now use their laptop using good ergonomic postural positioning “some of the time”. As a result of attending the ergonomic educational session, the participant group now put laptops on desk or higher surface rather than in lap, keep laptop screen at eye level, have better head and neck positioning, and adjust keyboard distance. Three OT students, 8 PT students, and 2 NA students reported purchasing a separate or detachable mouse. In addition, 1 PT student purchased a separate keyboard and another PT student purchased a new laptop stand. After attending the laptop educational session, 43% OT students, 31% PT students, and 45% NA students commented on their increased awareness of ergonomics, appropriate adjustments of laptop height, implementation of proper body positioning, and increased knowledge of proper ergonomics. One student from each program reported refusal to use wrist pads.
The control group was also asked to respond to some open ended questions. One of 31 PT students reported purchasing a detachable mouse after taking the ergonomic quiz. Forty-two per cent of OT students, 23% of PT students, and 53% of NA students changed laptop positioning to the following: proper positioning of laptop, straighter posture, wrists off laptop surface, and adjustment in the level of screen to reach eye level. Seventyfive percent of OT students, 61% of PT students, and
 (a)
(a)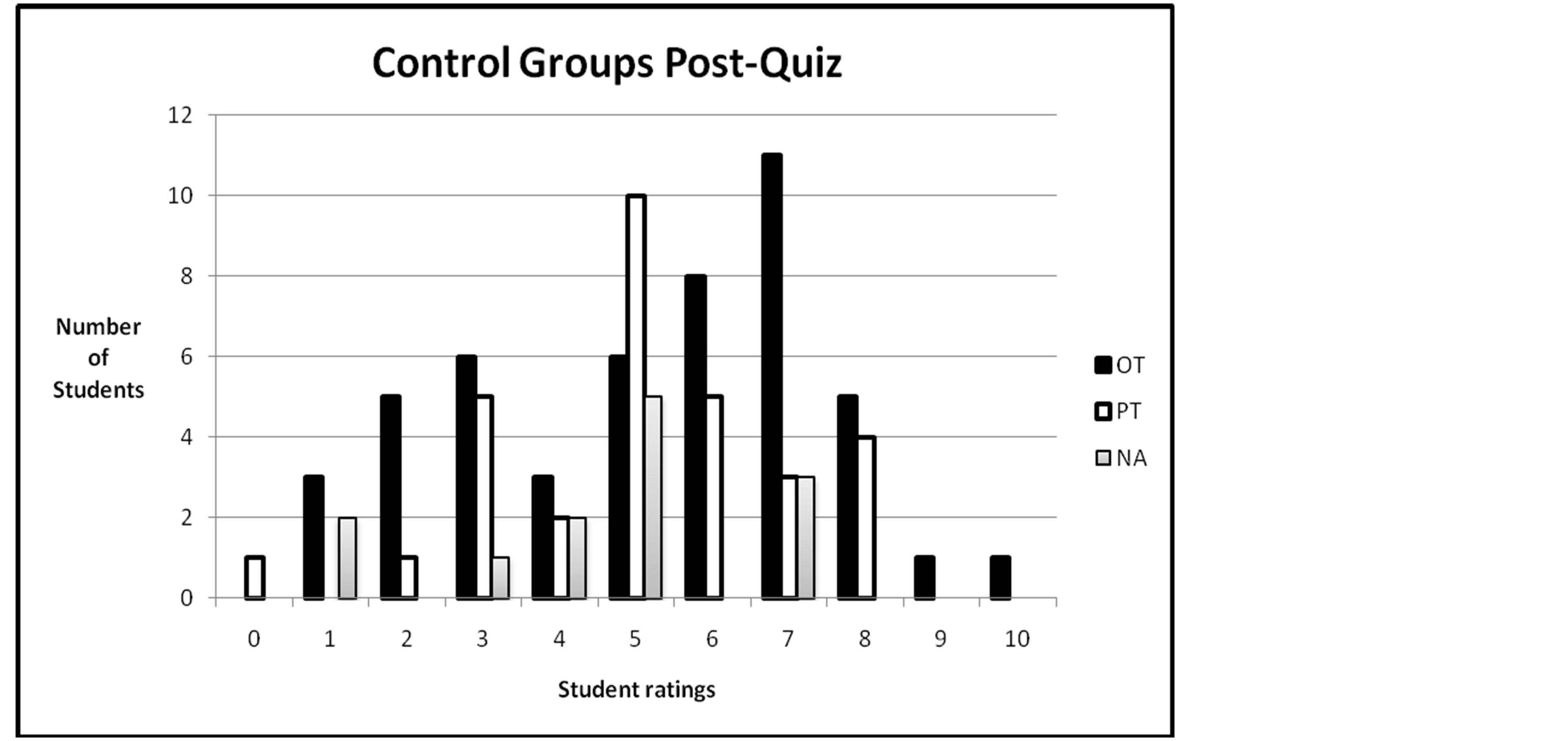 (b)
(b)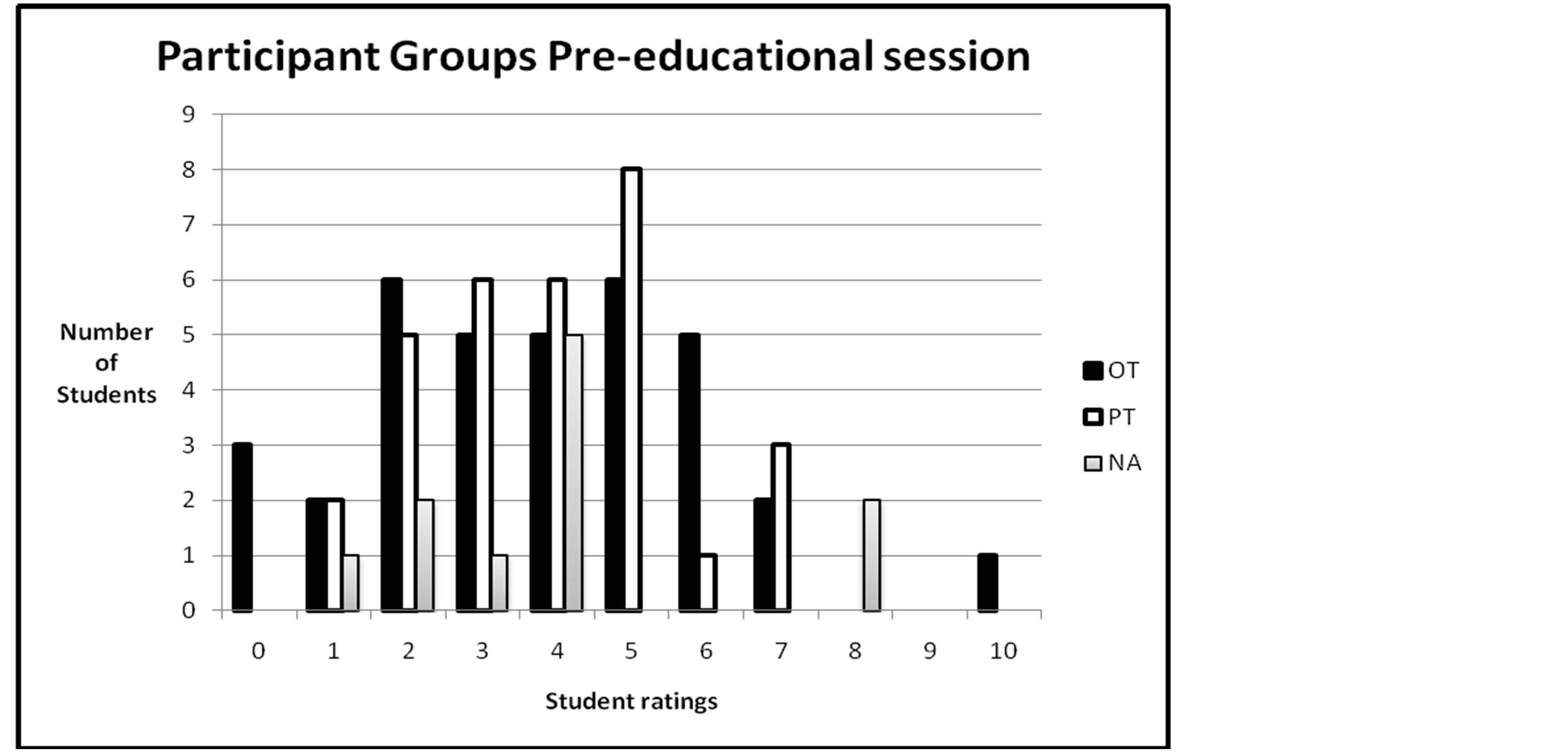 (c)
(c) (d)
(d)
Figure 2. (a) Health professional student ratings of correct ergonomic laptop use pre-ergonomic quiz. Ratings were on a scale of 0 - 10, “0” being the least ergonomically correct use of laptop and “10” being the most ergonomically correct use of laptop; (b) Health professional student ratings of correct ergonomic laptop use post-ergonomic quiz. Ratings were on a scale of 0 - 10, “0” being the least ergonomically correct use of laptop and “10” being the most ergonomically correct use of laptop; (c) Health professional student ratings of correct ergonomic laptop use preeducational session. Ratings were on a scale of 0 - 10, “0” being the least ergonomically correct use of laptop and “10” being the most ergonomically correct use of laptop; (d) Health professional student ratings of correct ergonomic laptop use post-educational session. Ratings were on a scale of 0 - 10, “0” being the least ergonomically correct use of laptop and “10” being the most ergonomically correct use of laptop.
53% of NA students stated that they use their laptops in the same position as they did prior to taking the ergonomic quiz.
Eight per cent of OT students and 6% of PT students commented that they had not made any changes, but were occasionally more aware of their positioning after taking the ergonomic quiz. Fifteen per cent of OT students, 10% of PT students, and 7% NA students reported that they needed to increase their awareness, become more knowledgeable, and be more diligent in carrying out the proper ergonomics of laptop positioning. Three of 48 in the OT control group reported using other educational resources such as schoolwork, the internet, and musculoskeletal class.
5. DISCUSSION
Based on the results, our research team concludes that receiving ergonomic education can positively influence awareness of body mechanics relative to laptop workstation design. The control group made a limited number of changes in response to the completion of the ergonomic quiz. However, there were also students who did not make any changes, yet were more aware of their positioning after taking the ergonomic quiz. Additional studies might examine longitudinal effects of such education and studies could be conducted on the improved ergonomic effects following in-service presentation in the workplace. Finally studies need to be conducted with a larger cohort of students using a larger sample size and looking at longer term effects of education on laptop computer usage.
The initial data set a foundation upon which to build. These results may shape future action regarding ergonomic education, not just among graduate students, but across other populations that may benefit from our study. While the present education targeted a limited sample set, the results may prove to generalize to students of any age as well as professionals across various fields of work and, therefore, will have an impact on those in allied health who may impart ergonomic knowledge to these and other populations.
The proper ergonomic design of laptops workstations is one aspect of a holistic approach to health and wellness that spans across professions. Any health professional seeking to prevent injury of his or her clients will benefit from these results. The fields of medicine, rehabilitation science, chiropractic health, and engineering, to name only a few, will be enhanced by the knowledge that ergonomic education does and will make a positive change in the behaviors of computer users.
6. LIMITATIONS
The current study was four weeks in duration and as stated in the discussion would be improved upon by a more longitudinal study. Some unique challenges and limitations may have influenced the results. For example the convenience sample of graduate students in the College of Health Professions provides a narrow focus of research because this population may have a higher level of previous knowledge about ergonomics than the typical subject in a randomized sample. Additionally, researchers in this study were confronted with the possibility that knowledge gained by subjects during the educational session does not always translate to functional changes in workstation setup. Additional research should include a follow-up survey or evaluation to determine any initiation by subjects to use the new knowledge to make changes in their everyday use of laptops. Scores alone cannot predict the functional outcomes evidenced by improved body mechanics.
A traditional laptop needs additional equipment such as a detachable keyboard, separate mouse, footrest, and screen holder to ensure correct ergonomic positioning. Currently, the only other viable option is investing in a costly laptop with a separating screen and keyboard [12].
Ideally a laboratory that is designed for laptop use should provide separate and independent keyboards and raise the height of the scree to enable proper ergonomic use. In the current economy this provision is cost prohibitive. Perhaps students who understand the serious consequences of failing to use proper ergonomic positioning may adapt their laptop during use at off campus locations.
7. CONCLUSIONS
Educating graduate students does make a difference to laptop computer use methods and at least potentially enables use of technology using improved methodologies and equipment. As technology decreases the size of computers to computer tablets and cell phones that are increasing greatly in capability, the need for education will not diminish. There are major ergonomics and postural challenges involved in the use of all types of communication devices.
Studies such as this one need to be completed on the use of new computer technology equipment as it is developed to ensure that repetitive strain injuries in hands and postural positioning to the rest of the body do not cause major wear and tear issues on the user.
ACKNOWLEDGEMENTS
Brianna L. Bailey, MS, OTR/L Emily K. Chaka, MS, OTR/L Rebecca A. Harley, MS, OTR/L Alyssa V. Harris, MS, OTR/L Rachel C. Miron, MS, OTR/L Allison K. Strock, MS, OTR/L As Medical University of South Carolina OT students that participated in the development of this research project.
REFERENCES
- Jacobs, K., Johnson, P., Dennerlein, J., Peterson, D., Kaufman, J., Gold, J. and Pencina, M. (2009) University students’ notebook computer use. Applied Ergonomics, 40, 404-409. http://dx.doi.org/10.1016/j.apergo.2008.11.009
- Bohr, P.C. (2000) Efficacy ergonomics education. Journal of Occupational Rehabilitation, 10, 243-255. http://dx.doi.org/10.1023/A:1009464315358
- Gravina, N., Lindstrom-Hazel, D. and Austin, J. (2007) The effects of workstation changes and behavioral interventions on safe typing postures in an office. Journal of Prevention, Assessment and Rehabilitation, 29, 245-253.
- Moffet, H., Hagberg, M., Hansson-Risberg, E. and Karlqvist, L. (2002) Influence of laptop computer design and working position on physical exposure variables. Clinical Biomechanics, 17, 368-375. http://dx.doi.org/10.1016/S0021-9290(02)00062-3
- Berkhout, A.L., Hendriksson-Larsen, K. and Bongers, P. (2004) The effect of using a laptopstation compared to using a standard laptop PC on the cervical spine torque, perceived strain and productivity. Applied Ergonomics, 35, 147-152. http://dx.doi.org/10.1016/j.apergo.2003.11.008
- Hamilton, A.G., Jacobs, K. and Orsmond, G. (2005) The prevalence of computer-related musculoskeletal complaints in female college students. Work, 24, 387-394.
- Moras, R. and Gamarra T. (2007) A survey of ergonomics issues associated with a university laptop program. Journal of Education and Human Development, 1, 2.
- Bureau of Labor Statistics (2001) Table 11. Number of nonfatal occupational injuries and illnesses with days away from work involving musculoskeletal disorders by selected worker and case characteristics. http://www.bls.gov/iif/oshwc/osh/case/ostb1154.pdf
- Shinn, J., Romaine, K., Casimano, T. and Jacobs, K. (2002) The effectiveness of ergonomic intervention in the classroom. Journal of Prevention, Assessment and Rehabilitation, 18, 67-73.
- Sotoyama, M., Bergqvist, U., Jonai, H. and Saito, S. (2002) An ergonomic questionnaire survey on the use of computers in schools. Industrial Health, 40, 135-141. http://dx.doi.org/10.2486/indhealth.40.135
- Ketola, R., Toivonen, R., Hakkanen, M., Luukkonen, R., Takala, E. and Viikari-Juntura, E. (2002) Effects of ergonomic intervention in work with video display units. Scandinavian Journal of Work, Environment & Health, 28, 18-24. http://dx.doi.org/10.5271/sjweh.642
- Neo. (2005) Hot-screen saver. http://digital-lifestyles.info/2005/11/02/samsung-m70-hybrid-pc-with-detachable-screen-unveiled/