Incidence of Incidental Thyroid Nodules on Computed Tomography (CT) Scan of the Chest Performed for 265
Reasons Other than Thyroid Disease
malignant which has potential clinical significance.
In summary, previous studies have shown an ap-
proximately 16% incidence of incidental thyroid nodules
on CT scan of the head/neck and thorax combined.
However, no study to date has been performed to iden-
tify incidental thyroid nodules on CT scan of the thorax
alone.
We conducted a retrospective study to evaluate 500
CT scans of the chest performed at Erlanger Health
System to first determine the incidence of incidental
thyroid nodules (non-dominant 5 - 10 mm and dominant
> 10mm) on CT scan of the chest done for indications
other than thyroid disease and second, to determine
whether those subjects with incidental thyroid nodule
were further evaluated with thyroid function testing,
ultrasonography, fine needle aspiration, and/or nuclear
medicine scintigraphy. We will comment as to whether
or not incidental nodules are considered significant, i.e.
pursued with further evaluation. This will be included in
our final discussion.
Our hypothesis is that with the increased use of CT
scans of the chest, the incidence of incidental thyroid
nodules found will be higher than previously reported on
CT head/neck imaging.
2. Methods and Design
500 CT scans of the chest (both contrast and non-con-
trast) performed at Erlanger Health Science Center for
reasons other than thyroid pathology were reviewed ret-
rospectively to identify thyroid nodules. These CT Scans
were performed from October 2007 to October 2008 and
selected from the PACS. For patients with positive nod-
ules on the CT scans, medical records were reviewed to
document if further evaluation (thyroid function testing,
ultrasound, radioactive iodine uptake, nuclear medicine,
and/or scintigraphy) was performed for positive nodules.
CT scans of patients with predetermined and docu-
mented thyroid pathology in their medical records were
excluded. The study refers to incidental thyroid nodules,
with non-dominant nodules measuring less than 10 mm
and dominant nodules measuring greater than 10 mm.
This distinction was performed because of a suspected
higher malignant potential of a dominant nodule. No
patient identification was recorded during image view-
ing and comparison with medical record. Data was iden-
tified as a numerical number, 1 - 500 on an excel spread-
sheet.
All evaluators were initially trained by a board certi-
fied Radiologist regarding the CT criteria for thyroid
nodules. Also, all evaluators reviewed the anatomy of
the thyroid region with special attention to imaging
through Brant & Helms Diagnostic Imaging. After in-
dependent data collection and analyses by the individual
evaluators, all the positive and questionable negative
findings were reviewed collectively by the evaluators in
order to address inter-observer variability.
The supervising radiology faculty did a final read to
confirm the positive findings and review any question-
able negatives. Using Statistical Analysis System (SAS)
software, prevalence, frequency, and cross-tabulation
data were determined. Data was further categorized by
age, gender and race, size, location and number of nod-
ules, +/– contrast, further evaluation of positive nodules,
and negligible, partial, or complete imaging of the thy-
roid.
The inclusion criteria were 500 CT scans of the chest
or including the chest, for non-thyroid etiologies, in-
cluding scans with no thyroid, partial thyroid, or full
thyroid. The exclusion criteria were 1) CT scans per-
formed for suspected thyroid disease as indicated on
ordering diagnosis; 2) CT scan performed in patient with
known thyroid disease if indicated on order; 3) CT scan
of inadequate quality for thyroid gland evaluation; 4)
Repeat studies of same patient; 5) High resolution CT,
as they tend to be exams of the lung parenchyma.
The criteria for positive thyroid nodule identification
are as detailed below:
1) <0.5 cm (5 mm) incidental thyroid nodule is con-
sidered non viable in this study.
2) 0.5 cm - 1.0 cm (5 mm - 10 mm) incidental thyroid
nodule is included as a non-dominant nodule
3) >1.0 cm (10 mm) incidental thyroid nodule is in-
cluded as a dominant nodule
3. Result
500 CT scans of the chest were reviewed in our study.
The frequency of contrast use was 254 (50.8%) com-
pared to non-contrast study 246 (49.2%). The age range
was 18 and 93 with mean of 58.3. Mean number of nod-
ules 1.7 and mean nodule size of 13.7 mm. The male-
female ration in this study was 257:243.
Sixty-one (12.2 %) of 500 h ad ITNs (Table 1 and Fig-
ure 1(a)-(d)), of which 28 were males and 33 females.
The abnormality was solitary in 43 patients (70.5%) and
multiple in 18 (29.5%). Of the 61 cases with thyroid
nodules, 33 (54.1%) were dominant thyroid nodules
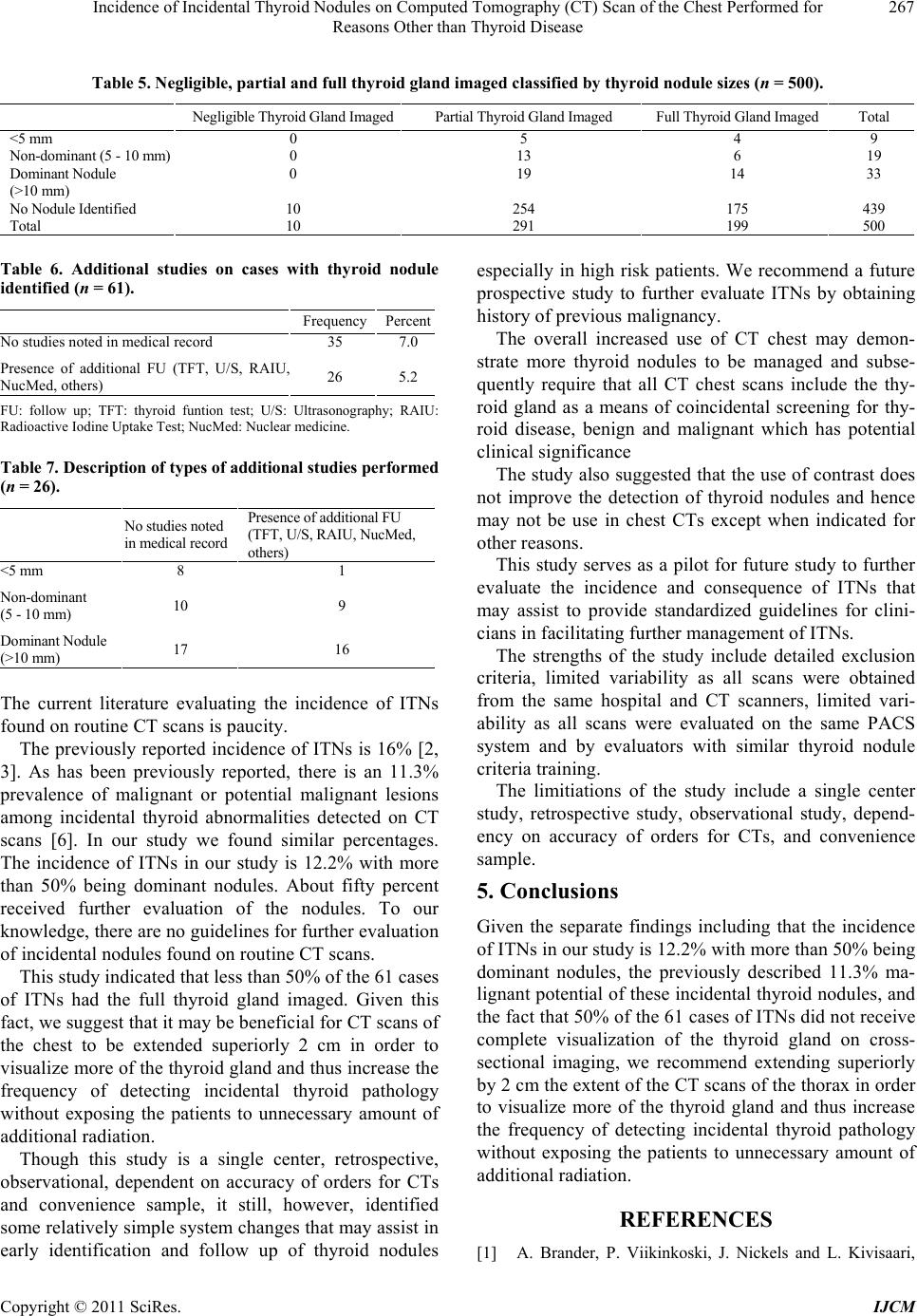
measuring greater than 1 cm (Table 2). Of the 500 total
CT scans, 10 did not include the thyroid gland, 291
(58.2%) included partial thyroid gland and only 199
(39.8%) included the full thyroid image (Table 3). The
majority of the nodules were found in the CTs with par-
tial thyroid image vs. full thyroid image 37 (60.7%) vs.
24 (39.3%) (Table 4). Furthermore 19 of the 33 (57.6%)
dominant thyroid nodules were found in the CT scans
Copyright © 2011 SciRes. IJCM