Drug-Eluting Stent for the Treatment of Early Fistula Failure199
were reported by Turmel and Manninen [5,18]. Stent-
graft placement has been also proposed as solution to the
complication of restenosis caused by neo-intimal hyper-
plasia only along the venous outflow.
Although arterial restenosis appears to be significantly
less common compared to the situation that currently
occurs in the venous system, larger studies showed a
40% primary patency rate at 12 months after arterial PTA
(performed with POBA) [17]. This means that about 60%
of patients could have been submitted to a new interven-
tion at 12 months. Moreover, flow-limiting restenosis
could be considered the primum movens to the AVF
thrombosis followed by its failure. For these reasons,
restenosis should be avoided, in particular for older pa-
tients to who could be difficult to find a new access and
who do not tolerate the onset of a new su b-optimal dialy-
sis session. The use of drug-eluting stents could be pro-
posed to ensure a better primary patency rate. Indeed,
although arterial restenosis appears to be different in
each arterial district, the experience coming from the
percutaneous treatments of the coronary artery disease
can be useful also for the treatment of the arterial vessels
disease in the upper limbs. This suggests that the use of
drug-eluting stents might reduce neointimal proliferation
also in this district, ensuring a better primary AVF patency
for these patients.
Endeavor® Resolute drug-eluting stent, which we used
in our case, has a proprietary new biocompatible polymer
called BioLinx. The BioLinx polymer is designed to
confer the same biocompatibility as the Endeavor stent’s
phosphorylcholine (PC) polymer while extending the
duration of drug exposure (Zotarolimus) in the vessel.
Developed by Medtronic scientists, BioLinx is the first
polymer specifically created for use on a drug-eluting
stent. The BioLinx polymer features a unique blend of
hydrophilic and hydrophobic elements for optimal per-
formance. Extensive preclinical studies have established
the biocompatibility and drug delivery capabilities of the
BioLinx polymer. Patients treated with the Endeavor
Resolute stent in the RESOLUTE clinical trial required
no repeat procedures through 9 months and had experi-
enced no protocol-defined stent thrombosis through 12
months of follow-up. Instent late lumen loss at 9 months,
the study’s primary endpoint, was met at 0.22 0.27 mm,
providing assurance of vessel healing in the targeted
range while preventing repeat procedures. Among the
trial’s 130 patients, only one required clinically-driven
Target Lesion Revascularition (TLR) or Target Vessel
Revascularization (TVR) through 12 months. The inci-
dence of major adverse cardiac events was 8.5 through
12 months [19].
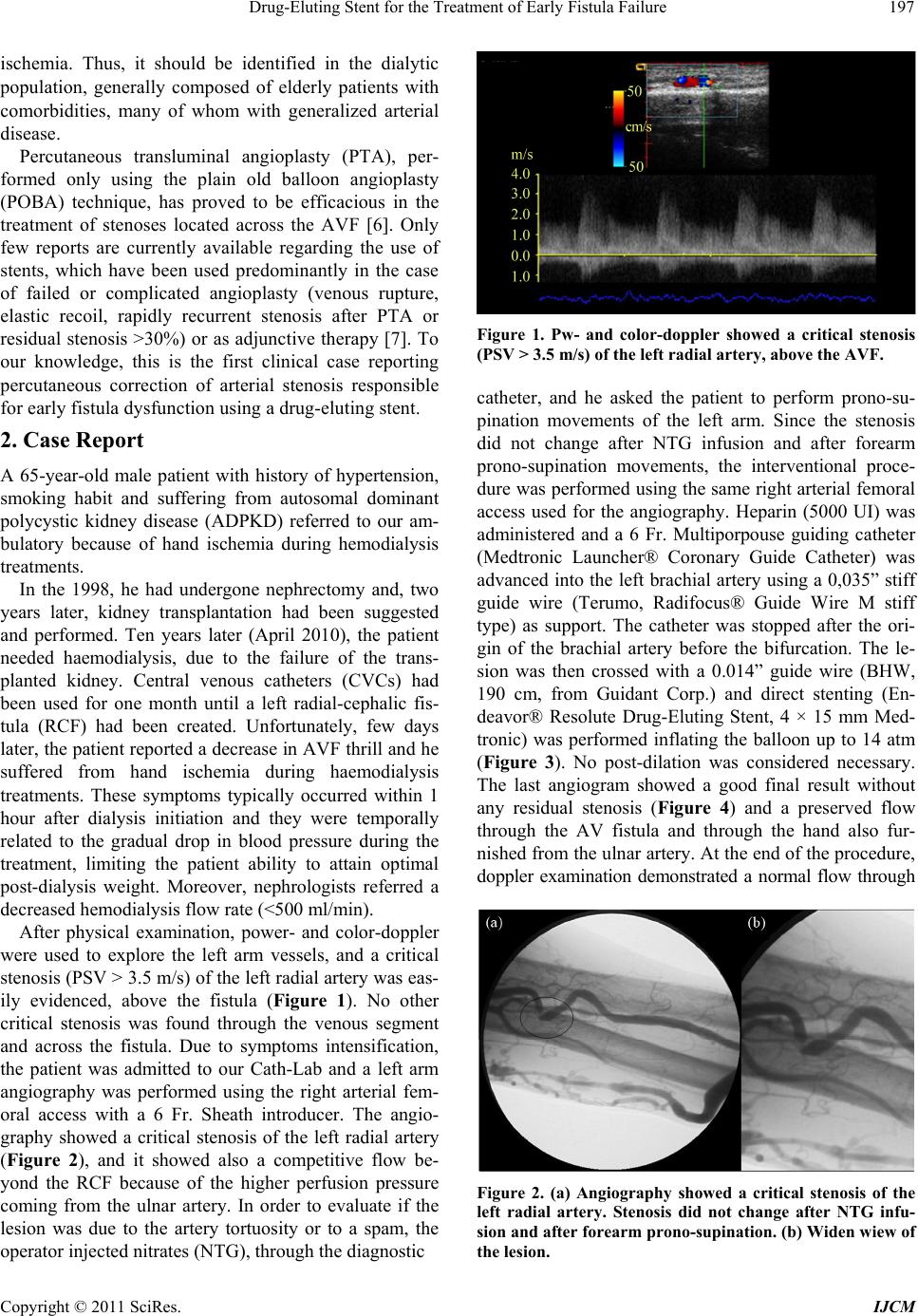
We report the case of a patient who was suffering from
left hand ischemia during sub-optimal haemodialysis
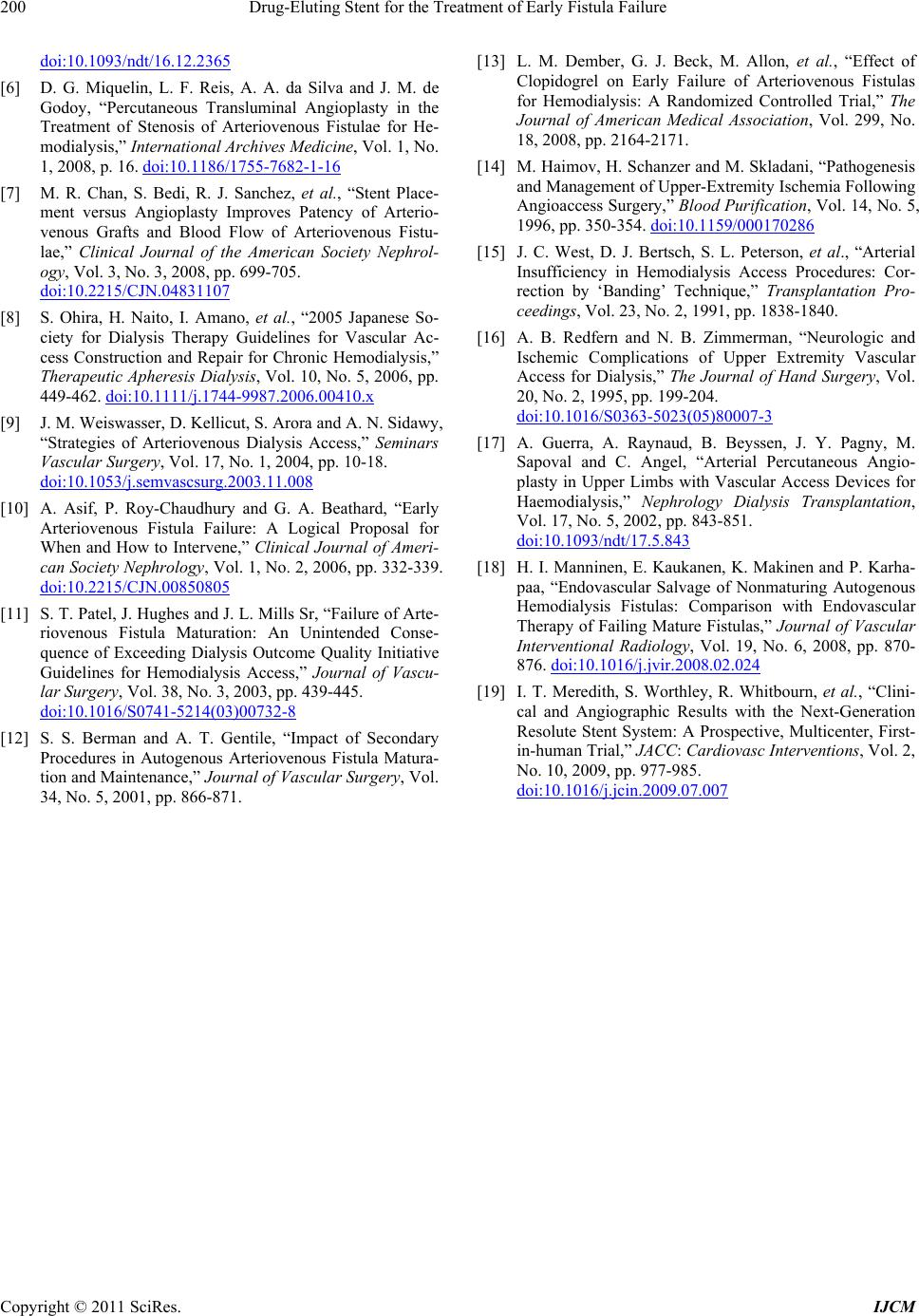
treatments. The interventional procedure was performed
without any complication and after direct stent implanta-
tion no further dilatation was necessary. Peri-procedural
Color-doppler examination showed a good final result
with complete stent struts apposition to the arterial wall.
The patient, after successful angioplasty of the pre-an-
astomotic inflow stenosis, had a significant increase in
fistula pressure. Adaptive remodelling and enhanced
blood flow in the fistula permitted hemodialysis to be
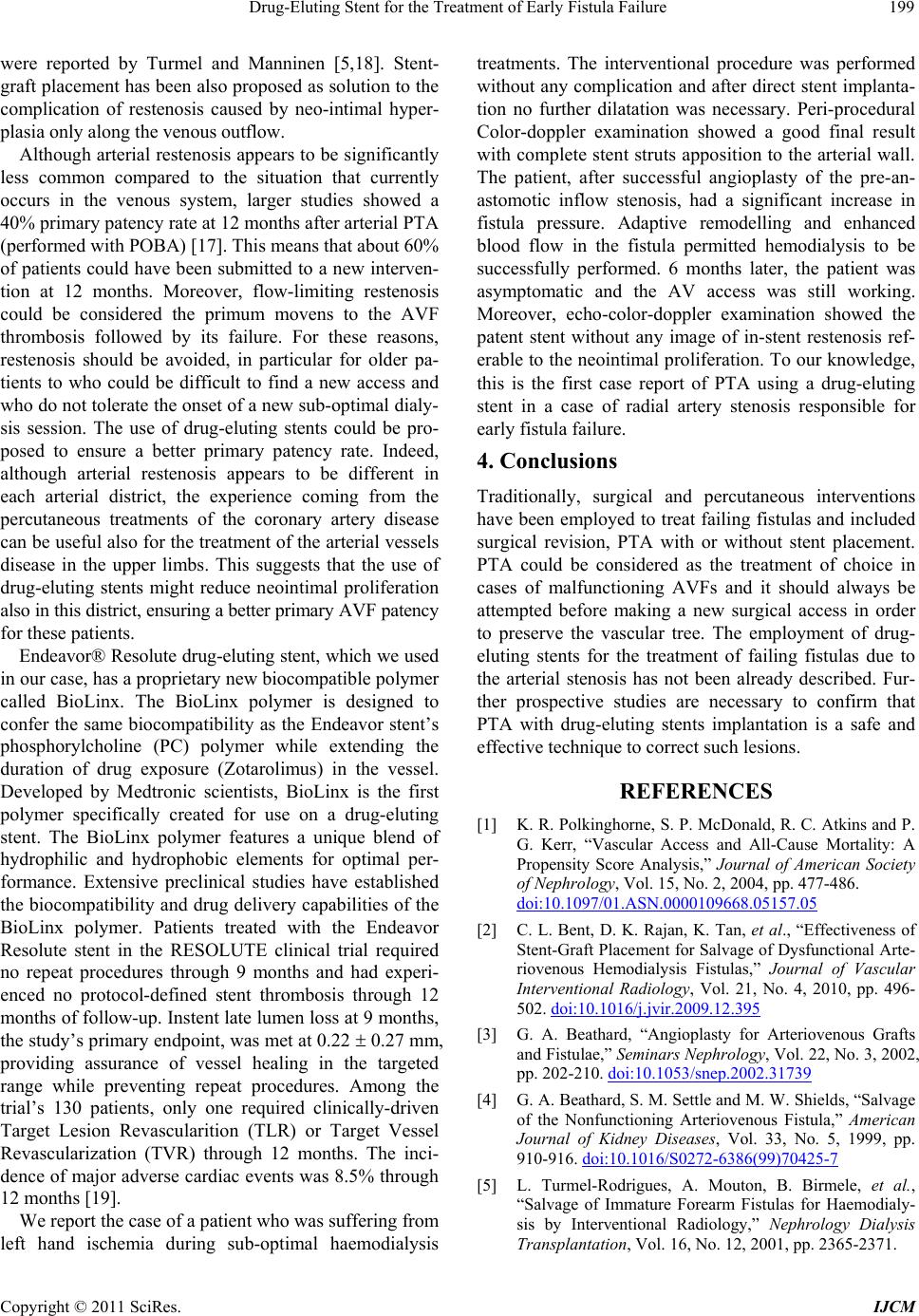
successfully performed. 6 months later, the patient was
asymptomatic and the AV access was still working.
Moreover, echo-color-doppler examination showed the
patent stent without any image of in-stent restenosis ref-
erable to the neointimal pro liferation. To our knowledge,
this is the first case report of PTA using a drug-eluting
stent in a case of radial artery stenosis responsible for
early fistula failure.
4. Conclusions
Traditionally, surgical and percutaneous interventions
have been employed to treat failing fistulas and included
surgical revision, PTA with or without stent placement.
PTA could be considered as the treatment of choice in
cases of malfunctioning AVFs and it should always be
attempted before making a new surgical access in order
to preserve the vascular tree. The employment of drug-
eluting stents for the treatment of failing fistulas due to
the arterial stenosis has not been already described. Fur-
ther prospective studies are necessary to confirm that
PTA with drug-eluting stents implantation is a safe and
effective technique to correct such lesions.
REFERENCES
[1] K. R. Polkinghorne, S. P. McDonald, R. C. Atkins and P.
G. Kerr, “Vascular Access and All-Cause Mortality: A
Propensity Score Analysis,” Journal of American Society
of Nephrology, Vol. 15, No. 2, 2004, pp. 477-486.
doi:10.1097/01.ASN.0000109668.05157.05
[2] C. L. Bent, D. K. Rajan, K. Tan, et al., “Effectiveness of
Stent-Graft Placement for Salvage of Dysfunctional Arte-
riovenous Hemodialysis Fistulas,” Journal of Vascular
Interventional Radiology, Vol. 21, No. 4, 2010, pp. 496-
502. doi:10.1016/j.jvir.2009.12.395
[3] G. A. Beathard, “Angioplasty for Arteriovenous Grafts
and Fistulae,” Seminars Nephrology, Vol. 22, No. 3, 2002,
pp. 202-210. doi:10.1053/snep.2002.31739
[4] G. A. Beathard, S. M. Settle and M. W. Shields, “Salvage
of the Nonfunctioning Arteriovenous Fistula,” American
Journal of Kidney Diseases, Vol. 33, No. 5, 1999, pp.
910-916. doi:10.1016/S0272-6386(99)70425-7
[5] L. Turmel-Rodrigues, A. Mouton, B. Birmele, et al.,
“Salvage of Immature Forearm Fistulas for Haemodialy-
sis by Interventional Radiology,” Nephrology Dialysis
Transplantation, Vol. 16, No. 12, 2001, pp. 2365-2371.
Copyright © 2011 SciRes. IJCM