S. Kim et al. / Health 3 (2011) 432-436
Copyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/
435
of mHBT on fatigue, future studies would benefit from
manipulating fatigue induction and evaluating the effects
in participants undergoing similar physical load.
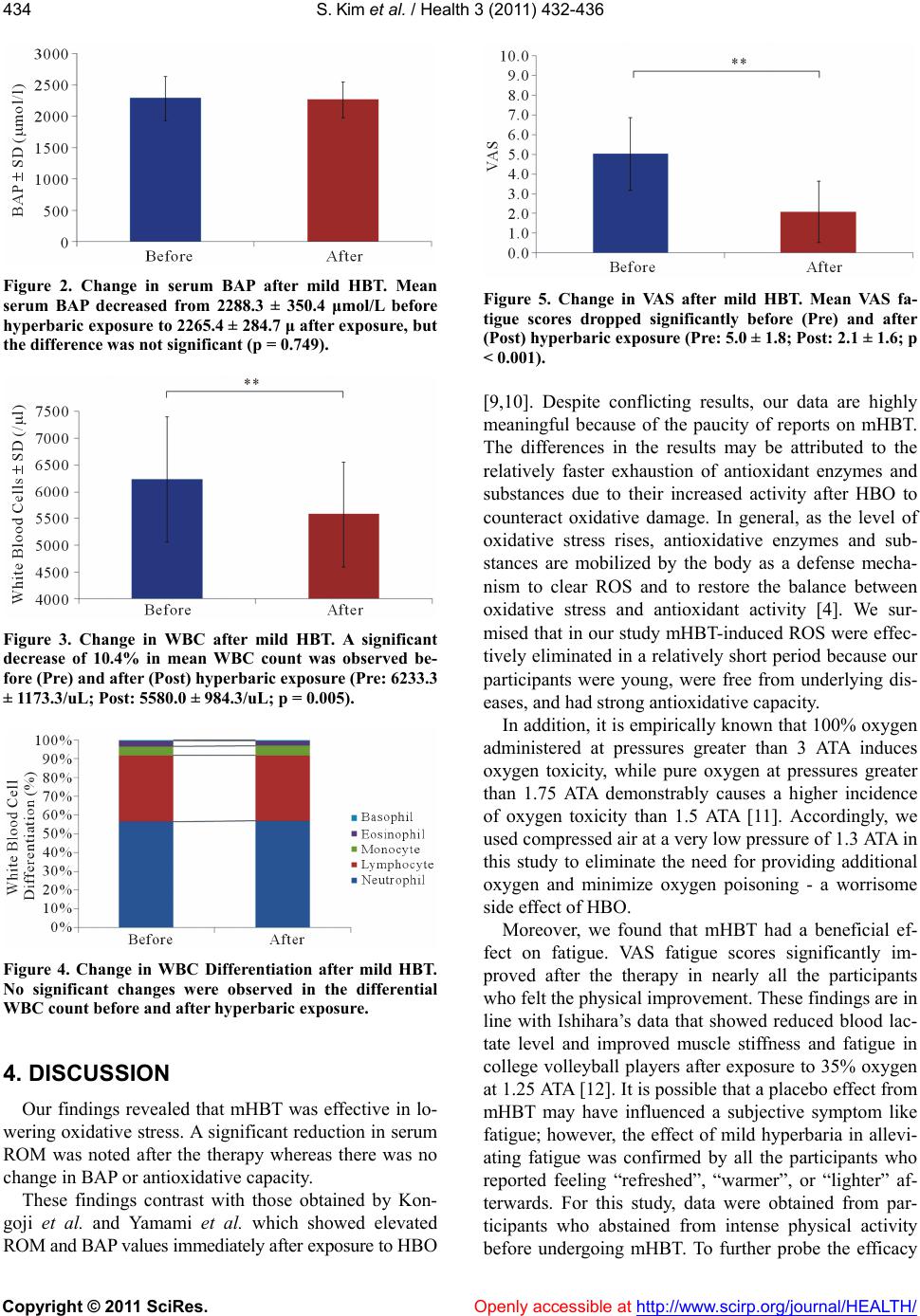
Although WBC count significantly decreased after
mHBT, WBC differential did not show a remarkable
change. These findings are congruent with Osbourne et
al.’s data which showed a decrease in WBC count by
32% and 13% in rats exposed to hyperbaric pressures at
4 ATA with 100% oxygen for 90 minutes and at 4 ATA
with 21% oxygen for 90 minutes, respectively. Addi-
tionally, the investigators hypothesized that stress from
HBO induced greater adrenal cortisol secretion, which in
turn caused a decrease in WBCs [13]. In this study
WBCs decreased in almost all the participants after
mHBT; however, WBC differential did not change in
response to the therapy. A re-evaluation of the latter 4-6
hours after the exposure is warranted as differential leu-
kocyte activity is known to change over time.
Much controversy currently exists over the efficacy of
mHBT. In May 2006, a panel entitled “Round table dis-
cussion on mild HBT” was held at the Third Annual
Meeting of Japanese Association for Clinical Hyperbaric
Oxygen and Diving (JACHOD). At this meeting, a vig-
orous debate over the efficacy of mHBT ensued between
JACHOD, an opponent of mHBT, and Japan Interna-
tional Hyperbaric Association Inc. (JIHA), a proponent
of mHBT. Although the main purpose of HBO is to raise
the levels of oxygen in body fluids, most oxygen carried
in the blood is bound to hemoglobin, rendering absolute
hemoglobin concentration as the limiting factor for oxy-
gen uptake. However, the mechanism of HBO rests on
Henry's Law that states a gas is dissolved by a liquid in
direct proportion to its partial pressure, i.e., HBO utilizes
increased atmospheric pressure to enhance oxygen dis-
solution in the plasma and resultant higher concentration
of liquefied oxygen to reverse hypoxia. Further, mHBT
was developed and based on the theory that liquefied
oxygen is more refined than conjugated oxygen and
therefore has a greater capacity to transport oxygen to
peripheral tissues. However, several studies have found
that mild hyperbaria at 1.3 ATA yields 0.57 mL/dL of
liquefied oxygen, which is significantly less than 2.0
mL/dL of liquefied oxygen from compressed air at 1.0
ATA, leading to some investigators to refute the ability
of mHBT (pressurized ambient air at 1.3 ATA) to deliver
the benefits of oxygen therapy [14-16].
Meanwhile, Ishii et al. studied the effects of various
hyperbaric pressures and discovered that lactate clear-
ance rate after maximal exercise at 1.3 ATA and 100%
oxygen was significantly greater than the rate at normal
atmosphere and room air; hence, the authors reported
that atmospheric pressure need not be raised to 2.0 ATA
because 1.3 ATA, which imposes comparatively less stress
than 2.0 ATA on the biological system, was sufficiently
effective [7]. Moreover, Ikeda et al. found that com-
pressed air at 1.3 ATA using Oasis O2 for the treatment
of acute lower leg muscle strain in professional soccer
players significantly reduced the time to return to sport
after injury, as observed from the difference in recovery
time between the non-treatment group versus the treat-
ment group (2.9 ± 1.4 weeks vs. 1.9 ± 0.5 weeks) [6]. It
appears that further research is necessary to clarify the
dearth of studies on the controversial effects of 1.3 ATA
5. CONCLUSIONS
Our findings suggest that mHBT is helpful in reducing
oxidative stress and improving fatigue while posing mi-
nimal risks, yet its effect on antioxidant capacity is less
clear. Research will be needed to examine the therapeu-
tic significance of 1.3 ATA in health promotion and dis-
ease prevention.
REFERENCES
[1] Cho, S. (2008) Oxigen toxicity and hyperbaric oxygen
therapy. Laser Interferometer Space Antenna, 15, 344-
349.
[2] Tamura, H. (2005) Indication of hyperbaric oxygen ther-
apy. Clinical Engineerin g, 16, 126-133.
[3] Narkowicz, C.K. (1993) Hyperbaric oxygen therapy
increases free radical level in the blood of humans. Free
Radical Research Communications, 19, 71-80.
doi:10.3109/10715769309056501
[4] Speit, G., et al. (2000) Induction of heme oxygenase-1
and adaptive protection against the induction of DNA
damage after hyperbaric oxygen treatment. Carcinogene-
sis, 21, 1795-1799. doi:10.1093/carcin/21.10.1795
[5] Saito, K. (2009) Effects of exposure time to hyperbaric
air chamber (HBA) on oxidative stress, peripheral blood
counta and blood filtration time in male students. Journal
of Japanese Association for Hyperbaric Oxygen and Di-
ving, 6, 27-30.
[6] Ikeda, H. (2005) Hyperbaric oxygen therapy for acute
muscle strain. Orthopaedic Surgery and Traumatology,
48, 955-958.
[7] Ishii, Y. (1995) The effect of hyperbaric oxygen therapy
on the lactate concentration after maximal exercise. The
Japanese Journal of Hyperbaric Medicine, 30, 109-114.
[8] Japanese Society of Fatigue Science (2008) Visual ana-
logue scale for fatigue.
http://www.hirougakkai.com/VAS.pdf
[9] Kongoji, J., et al. (2007) Reactive oxygen metabolites
and biological antioxidant potential in humans after a
single exposure to hyperbaric oxygen therapy. The Japa-
nese Journal of Hyperbaric and Undersea Medicine, 42,
23-29.
[10] Yamami, N., et al. (2007) A discussion on oxidative and
antioxidative markers under a hyperbaric oxygen envi-
ronment. The Japanese Journal of Hyperbaric and Un-
dersea Medicine, 42, 85-91.
[11] Nishii, Y. (2006) Expectation for the maintenance and