Quality of Life of Patients with Metastatic Breast Cancer Treated with Epirubicin and Docetaxel
350
some improvement. However, the quality of life did not
return to baseline level although there was a trend to-
wards improved emotional functioning at the end of the
treatment. Our assessment was more comprehensive and
detailed using validated quality of life questionnaires.
Due to the differences in the methods, it is somewhat
difficult to compare the results between the studies. In
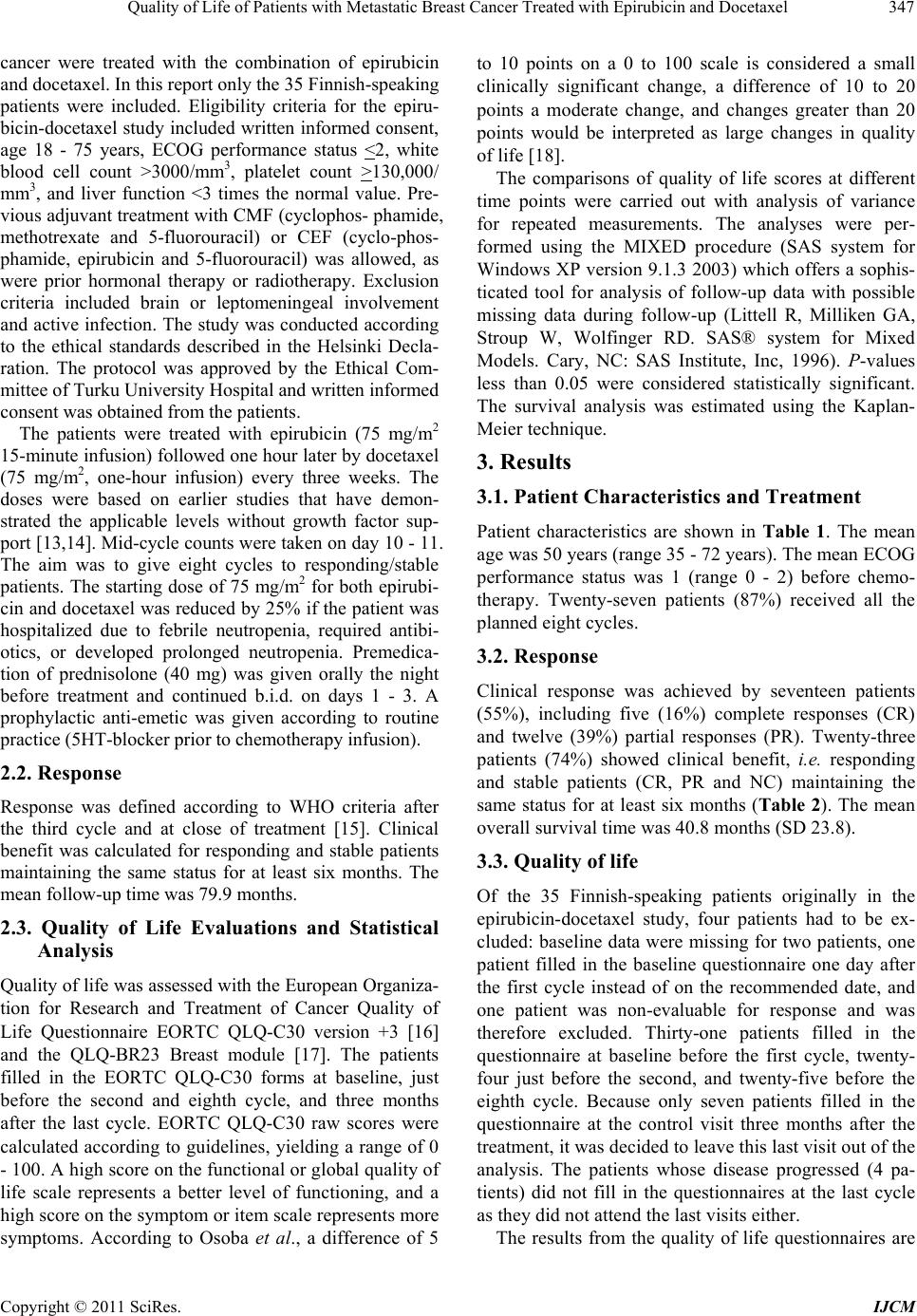
terms of physical functioning, our results are quite simi-
lar, but we found no statistically significant changes in
terms of pain, nausea or appetite. The results concern-
ing emotional functioning were different during the
chemotherapy. Nevertheless, in both studies, there was a
trend towards better emotional functioning at the end of
the treatment.
The major limitation of our quality of life study, in
addition to the small sample size, is the number of
missing questionnaires. The most common reasons for
missing data were progressive disease (four patients)
and administrative factors such as incomplete collection
of questionnaires. In the literature, many other authors
have shown that institutional and administrative factors
tend to be more influential than patient factors at least
until performance status deteriorates [3,27,28]. The
dropout of the patients with progressive disease is of
major concern because it distorts the results. The num-
ber of dropouts overestimates the effect of therapy on
quality of life as patients with progressive disease and
poor performance tolerated treatments poorly. Missing
data form one of the greatest methodological challenges
in cancer quality of life research [29].
In conclusion, the combination of epirubicin and do-
cetaxel showed clinical benefit among a good number of
patients in first-line chemotherapy of metastatic breast
cancer with manageable adverse effects. During the
treatment the emotional functioning improved and con-
cerns about the future were relieved. Some aspects of
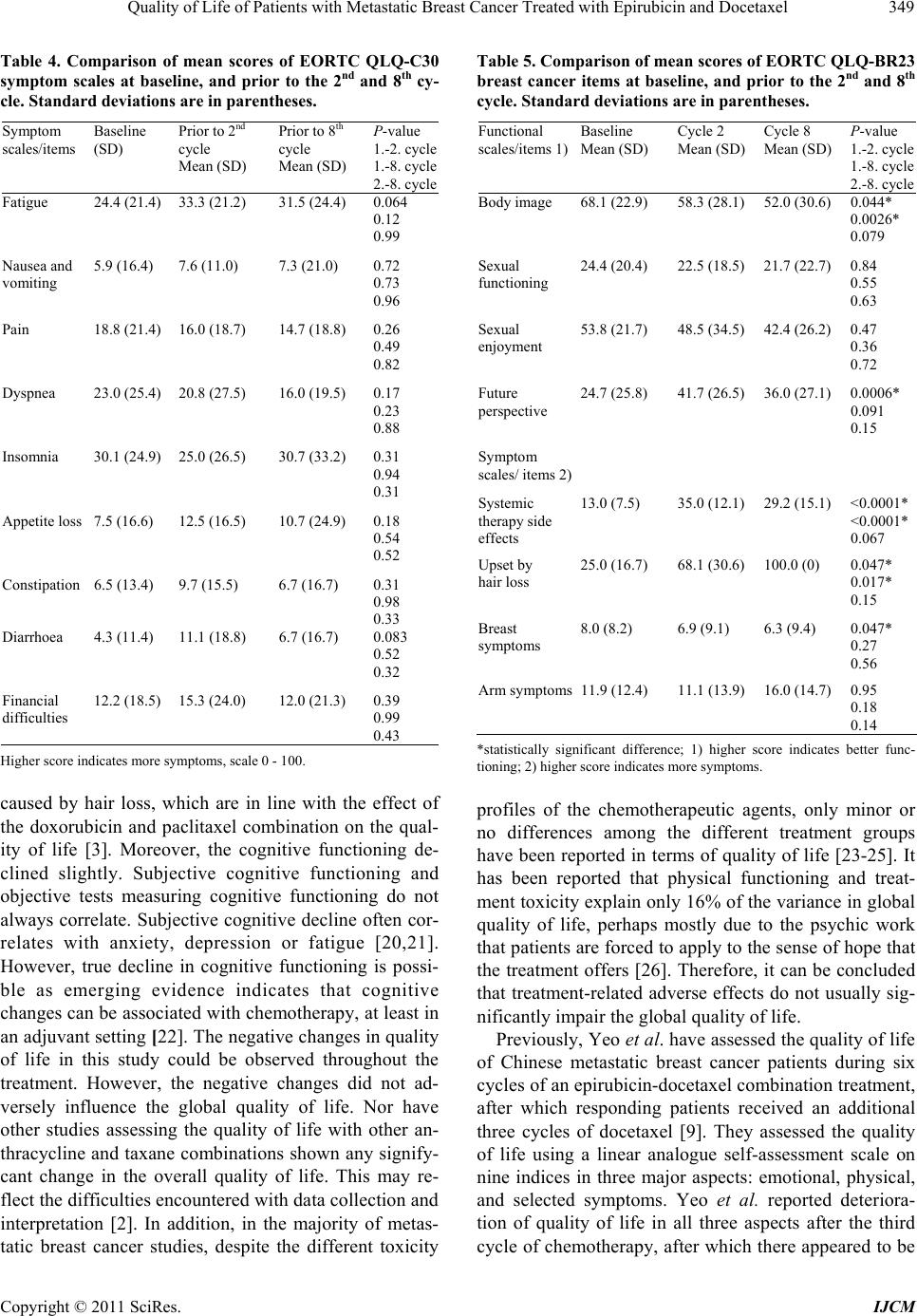
quality of life were impaired, with slightly decreased
physical and cognitive functioning, distress related to
changes in body image and hair loss, and other adverse
effects of chemotherapy. However, the global quality of
life was maintained.
REFERENCES
[1] N. Wilcken and R. Dear, “Chemotherapy in Metastatic
Breast Cancer: A Summary of All Randomised Trials
Reported 2000-2007,” European Journal of Cancer, Vol.
44, No. 15, 2008, pp. 2218-2225.
doi:10.1016/j.ejca.2008.07.019
[2] D. Ghersi, N. Wilcken and R. J. Simes, “A Systematic
Review of Taxane-Containing Regimens for Metastatic
Breast Cancer,” British Journal of Cancer, Vol. 93, No. 3,
2005, pp. 293-301. doi:10.1038/sj.bjc.6602680
[3] A. Bottomley, L. Biganzoli, T. Cufer, et al., “Randomize d,
Controlled Trial Investigating Short-Term Health-Related
Quality of Life with Doxorubicin and Paclitaxel versus
Doxorubicin and Cyclophosphamide as First-Line Che-
motherapy in Patients with Metastatic Breast Cancer: Eu-
ropean Organization for Research and Treatment of Can-
cer Breast Cancer Group, Investigational Drug Branch for
Breast Cancer and the New Drug Development Group
Study,” Journal of Clinical Oncology, Vol. 22, No. 13,
2004, pp. 2576-2586. doi:10.1200/JCO.2004.02.037
[4] P. A. Cassier, S. Chabaud, V. Trillet-Lenoir, et al., “A
Phase-III Trial of Doxorubicin and Docetaxel versus
Doxorubicin and Paclitaxel in Metastatic Breast Cancer:
Results of the ERASME 3 Study,” Breast Cancer Re-
search and Treatment, Vol. 109, No. 2, 2008, pp. 343-
350. doi:10.1007/s10549-007-9651-3
[5] J. M. Nabholtz, C. Falkson, D. Campo, et al., “Docetaxel
and Doxorubicin Compared with Doxorubicin and
Cyclophosphamide as First-Line Chemotherapy for Me-
tastatic Breast Cancer: Results of a Randomized, Multi-
center, Phase III Trial,” Journal of Clinical Oncology,
Vol. 21, No. 6, 2003, pp. 968-975.
doi:10.1200/JCO.2003.04.040
[6] J. Jassem, T. Pienkowski, A. Pluzanska, et al., “Doxoru-
bicin and Paclitaxel versus Fluorouracil, Doxorubicin and
Cyclophosphamide as First-Line Therapy for Women with
Metastatic Breast Cancer: Final Results of a Randomized
Phase III Multicenter Trial,” Journal of Clinical Oncol-
ogy, Vol. 19, No. 6, 2001, pp. 1707-1715.
[7] G. W. Sledge, D. Neuberg, P. Bernardo, et al., “Phase III
Trial of Doxorubicin, Paclitaxel, and the Combination of
Doxorubicin and Paclitaxel as Front-Line Chemotherapy
for Metastatic Breast Cancer: An Intergroup Trial (E11-
93),” Journal of Clinical Oncology, Vol. 21, No. 4, 2003,
pp. 588-592. doi:10.1200/JCO.2003.08.013
[8] H. Svensson, Z. Einbeigi, H. Johansson, T. Hatschek and
Y. Brandberg, “Quality of Life in Women with Metastatic
Breast Cancer during 9 Months after Randomization in
the TEX Trial (Epirubicin and Paclitaxel w/o Capecit-
abine),” Breast Cancer Research and Treatment, Vol.
123, No. 3, 2010, pp. 785-793.
doi:10.1007/s10549-010-1084-8
[9] W. Yeo, T. S. Mok, K. K. Tse, et al., “Phase II Study of
Docetaxel and Epirubicin in Chinese Patients with Me-
tastatic Breast Cancer,” Anticancer Drugs, Vol. 13, No. 6,
2002, pp. 655-662.
doi:10.1097/00001813-200207000-00013
[10] J. Korpela and E. Salminen, “Neutropenic Infections Add
Significant Costs to Palliative Chemotherapy in Breast
Cancer,” Anticancer Research, Vol. 22, No. 2B, 2002, pp.
1337-1340.
[11] E. Salminen, J. Korpela, M. Varpula, et al., “Epirubi-
cin/Docetaxel Regimen in Progressive Breast Cancer-A
Phase II Study,” Anticancer Drugs, Vol. 13, No. 9, 2002,
pp. 925-929. doi:10.1097/00001813-200210000-00004
[12] E. Salminen, K. Syvanen, J. Korpela, et al., “Docetaxel
with Epirubicin-Investigations on Cardiac Safety,” Anti-
cancer Drugs, Vol. 14, No. 1, 2003, pp. 73-77.
doi:10.1097/00001813-200301000-00010
Copyright © 2011 SciRes. IJCM