M. F. Weiner et al. / Open Journal of Psychiatry 1 (2011) 49-55
Copyright © 2011 SciRes. OJPsych
[31]. We plan to re-test a subgroup of DHS-2 subjects
with additional brief measures that may increase sensi-
tivity to executive and memory function and we will also
follow them prospectively to examine the rate of cogni-
tive change.
Although the MoCA samples many of the same cog-
nitive areas than less sensitive instruments, several less
sensitive instruments have shown stronger correlations
of global cognitive function with cardiovascular risk
factors, including age and apoE status. Our failure to
find correlations of similar strength may be attributable
to some limitation of the MoCA, the relative youth of
the population we studied or differences between per-
sons with presymptomatic and symptomatic cardiovas-
cular disease.
REFERENCES
[1] Beeri, M.S., Ravona-Springer, R., Silverman, J.M. and
Haroutunian, V. (2009) The effects of cardiovascular risk
factors on cognitive compromise. Dialogues in Clinical
Neuroscience, 11, 201-212.
[2] Middleton, L.E., Barnes, D.E., Lui, L.Y. and Yaffe, K.
(2010) Physical activity over the life course and its asso-
ciation with cognitive performance and impairment in old
age. Journal of the American Geriatrics Society, 58,
1322-1326. doi:10.1111/j.1532-5415.2010.02903.x
[3] Yaffe, K., Vittinghoff, E., Lindquist, K., et al. (2010)
Posttraumatic stress disorder and risk of dementia among
us veterans. Archives of General Psychiatry, 67,
608-613. doi:10.1001/archgenpsychiatry.2010.61
[4] Tzourio, C. , D uf oui l, C ., D uc im etier e, P. and Alperovitch,
A. (1999) Cognitive decline in individuals with high
blood pressure: A longitudinal study in the elderly. Eva
study group. Epidemiology of vascular aging. Neurology,
53, 1948-1952.
[5] Mielke, M. M., Rosenbe r g, P. B., Tschanz, J., et al. (2007)
Vascular factors predict rate of progression in alzheimer
disease. Neurology, 69, 1850-1858.
doi:10.1212/01.wnl.0000279520.59792.fe
[6] Solomon, A., Kareholt, I., Ngandu, T., et al. (2007) Serum
cholesterol changes after midlife and late-life cognition:
Twenty-one-year follow-up study. Neurology, 68, 751-756.
doi:10.1212/01.wnl.0000256368.57375.b7
[7] Yaffe, K., Barr ett-Connor , E., Lin, F. and Grady , D . (2002)
Serum lipoprotein levels, statin use, and cognitive func-
tion in older women. Archives of Neurology, 59, 378-384.
doi:10.1001/archneur.59.3.378
[8] Reitz, C., Luchsinger, J., Tang, M.X., Manly, J. and
Mayeux, R. (2005) Impact of plasma lipids and time on
memory performance in healthy elderly withou t dementia.
Neurology, 64, 1378-1383.
doi:10.1212/01.WNL.0000158274.31318.3C
[9] Whitmer, R. A., Sidney, S., Selby, J., Johnston, S. C. and
Yaffe, K. (2005) Midlife cardiovascular risk factors and
risk of dementia in late life. Neurology, 64, 277-281.
doi:10.1212/01.WNL.0000149519.47454.F2
[10] Schnaider Beeri, M., Goldbour t, U., Silverman, J. M., et al.
(2004) Diabetes mellitus in midlife and the risk of de-
mentia three decades later. Neurology, 63, 1902-1907.
[11] Yaffe, K., Kanaya, A., Lindquist, K., et al. (2004) The
metabolic syndrome, inflammation, and risk of cognitive
decline. Journal of the American Medical Association,
292, 2237-2242. doi:10.1001/jama.292.18.2237
[12] Pfeiffer, E. (1975) A short portable mental status ques-
tionnaire for the assessment of organic brain deficit in
elderly patients. Journal of the American Geriatrics So-
ciety, 23, 433-441.
[13] Folstein, M.F., Folstein, S.E. and McHugh, P.R. (1975)
“Mini-mental state”. A practical method for grading the
cognitive state of patients for the clinician. Journal of
Psychiatric R es earch, 12, 189-198.
doi:10.1016/0022-3956(75)90026-6
[14] Nasreddine, Z.S., Phillips, N. A ., Bedirian, V., et al. (2005)
The montreal cognitive assessment, moca: A brief
screening tool for mild cognitive impairment. Journal of
the American Geriatrics Soci ety, 53, 695-699.
doi:10.1111/j.1532-5415.2005.53221.x
[15] Smith, T., Gildeh, N. and Holmes , C. (2007) The montreal
cognitive assessment: Validity and utility in a memory
clinic setting. Canadian Journal of Psychiatry, 52,
329-332.
[16] Hoops, S., Nazem, S., Siderowf, A. D., et al. (2009) Va-
lidity of the MoCA and mmse in the detection of mci and
dementia in parkinson disease. Neurology, 73,
1738-1745. doi:10.1212/WNL.0b013e3181c34b47
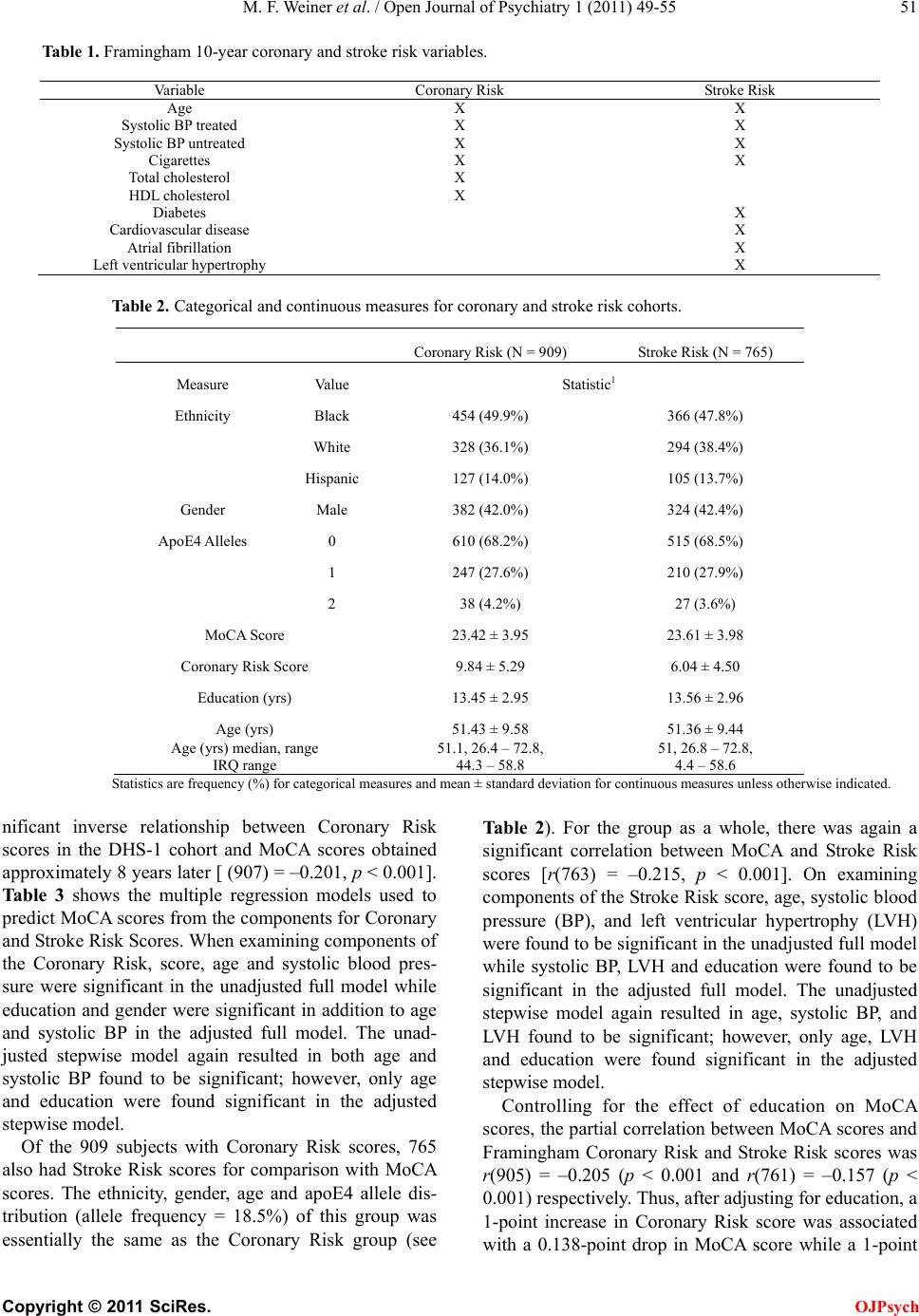
[17] D'Agostino, R. B., Sr., Grundy, S., Sullivan, L. M. and
Wilson, P. (2001) Validation of the framingham coronary
heart disease prediction scores: Results of a multiple eth-
nic groups investigation. Journal of the American Medical
Association, 286, 180-187. doi:10.1001/jama.286.2.180
[18] D’Agostino, R.B., Wolf, P.A., Belanger, A.J. and Kannel,
W.B. (1994) Stroke risk profile: Adjustment for antihy-
pertensive medication. The framingham study. Stroke, 25,
40-43. doi:10.1161/01.STR.25.1.40
[19] Victor , R. G., Hal ey, R. W., W illett, D . L., et al. (2004) The
dallas heart study: A population-based probability s ampl e
for the multidisciplinary study of ethnic differences in
cardiovascular health. American Journal of Cardiology,
93, 1473-1480.
[20] Wilson, P.W., D’Agostino, R.B., Levy, D., et al. (1998)
Prediction of coronary heart disease using risk factor
categories. Circulation, 97, 1837-1847.
[21] Aggarwal, A. and Kean, E. (2010) Comparison of the
folstein mini mental state examination (mmse) to the
montreal cognitive assessment (MoCA) as a cognitive
screening tool in an inpatient rehabilitation setting. Neu-
roscience and Medicine, 1, 39-42.
doi:10.4236/nm.2010.12006
[22] Bernstein, I.H., Lacritz, L., Barlow, C.E., Weiner, M.F.
and Defina, L. F. (2011) Psychometric evaluation of the
montreal cognitive assessment (MoCA) in three diverse
samples. Clinical Neuropsychology, 25, 119-126.
doi:10.1080/13854046.2010.533196
[23] McLennan, S.N., Mathias, J.L., Brennan, L.C. and Ste-
wart, S. (2010) Validity of the montreal cognitive as-
sessment (MoCA) as a screening test for mild cognitive
impairment (MCI) in a cardiovascular population. Journal
of Geriatric Psychiatry and Neurology, 24, 33-38.
[24] Kuczynski, B., Jagust, W., Chui, H.C. and Re ed, B. (2009)
An inverse association of cardiovascular risk and frontal