 Open Journal of Psychiatry, 2011, 1, 40-48 OJPsych doi:10.4236/ojpsych 2011.12007 Published Online July 2011 (http://www.SciRP.org/journal/OJPsych/). Published Onl ine July 2011 in SciRes. http://www.sc irp.org/ journal/OJPsych Subjective symptoms related to depression and suicidal risk in a Japanese community: a cross-sectional study* Shigeki Takemura1, Kouichi Yo shimasu1, Jin Fukumoto1, Hir oichi Yamamoto2, Kazuhisa Miyashita1 1Department of Hygiene, School of Medicine, Wa kay ama Medical University, Wakayama, Japan ; 2Osaka Occupational Health Service Center, Japan Industrial Safety and Health Association, Osaka, Japan. E-mail:steakmmi@hotmail.com Received 16 May 2011; revised 20 June 2011; accepted 29 June 2011 . ABSTRACT BACKGROUND: This cross-sectional study aimed to assess the association between self-reported somatic and mental symptoms and the presence of major de- pressive disorder (MDD) and suicidal risk among community dwellers in Japan. METHODS: From two locations in Japan, we recruited 732 community dwellers who underwent an annual health screening. Basic symptoms of MDD, dysthymia, and the pres- ence of associated suicidal risk were determined us- ing a brief structured diagnostic psychiatric interview, Mini International Neur opsychiatric Interview (MINI). Information regarding self-reported somatic and mental symptoms was obtained from a self-administered questionnaire used in the annual health check-up. Suicidal risk was evaluated on the basis of six relevant questions asked in MINI. Logis- tic regression model was used to calculate age- and gender-adjusted odds ratios (ORs) and 95% confi- dence intervals (CIs) for MDD. Further adjustment fo r basic symptoms of MDD was performed to calcu- late ORs and C Is for suicidal risk. RESULTS: A my- riad of somatic symptoms, including headache , heavy headedness, eye strain, and shoulder stiffness [ad- justed OR (95% CI), 11.4 (1.22 - 107) at location 1; 5.17 (1.23 - 21.7) at location 2], were associated with the presence of MDD. Dysmenorrhea [6.07 (1.14 - 32.3) at location 1] and dysesthesia, arthralgia, and swelling in the extremities [2.72 (1.14 - 6.47) at loca- tion 2] were significantly associated with an increase in suicidal risk, independent of the presence of basic symptoms of MDD. CONCLUSION: Several somatic symptoms, especially pain-related ones, may serve as possible signs of depression and suicidal risk among community dwellers. Keywords: Epidemiolog y; Somatic Symptoms; Depression; Suicide; Community Dwellers 1. INTRODUCTION More than 30,000 Japanese people die from suicide every year, and suicide is becoming a serious public health problem. Several epidemiological studies in general populations have indicated personal and social risk factors for suicide such as depression, severe an- xiety, substance abuse, and poor interpersonal rela- tionships including social isolation, inability to main- tain a job, anhedonia, somatic diseases, financial prob- lems, and personal or familial history of suicide [1-7]. Suicide is attributed to many causes including depres- sion and other emotional disorders [8]. Mood disorders account for 30.2% of completed suicide cases [9]. Depressive symptoms are accompanied by several somatic symptoms such as fatigue, insomnia, nau- sea/vomiting, back pain and so forth [10]. Among these symp t oms, pain-related symptoms have been associated with depression [11-15] and suicide [11,16-20]. Ac- cording to a Japanese government survey, the preva- lence of somatic symptoms, particularly pain-r elated symptoms, is higher among older Japanese people. Moreover, suicides in people aged ≥40 years account for >70 % of all su icide cas es in Japan, with the h ighest suicide rate in the sixth decade among men. The relationship between somatic symptoms and de- pression/suicidal risk can be explained with two as- sumptions. One is that people suffering from somatic disorders tend to develop depression or suicidal idea- tion. The other is that those who have depression or suicidal ideation with non-severe somatic disorders are likely to express their mental strain as transformed so- matic symptoms. Although several studies support both these assumptions [21-24], we adopted the latter one for the present study for the following reasons. About two-thirds of patients with depression first * This work was supported by a Grant-in- Aid for Scientific Research from the Japan Society for the Promotion of Science (JSPS KAKEN- HI) 19590645.  S. Ta ke mura et al. / Open Journal of Psychiatry 1 (2011) 40-48 Copyright © 2011 SciRes. OJPsych seek help from a primary care physician rather than a psychiatrist because they develop both somatic and mental symptoms [25]. Nevertheless, ph ysicians do not always evaluate the risk of depression or suicide among their patients for fear of reinvoking patients’ suicidal ideation or making them feel guilty of thinking about suicide, which is considered a sin in many religions [26]. Moreover, Japanese patients feel hesitant to con- sult a psychiatrist because compared to Westerners, they are generally more likely to share a feeling of stigmatization toward mental disorders or suicidal ide- ation [27], and to suppress their emotions accordingly. This observation was partially supported by the World Mental Health Japan Survey, showing a lower preva- lence of mood and anxiety disorders in Japan than in the United States or Europe [28]. Hence, detection of people at a high risk of depressive disorder or suicide will be delayed in J apan. Together with the above-mentioned situations, early detection of mental health-related somatic symptoms may help promote not only the secondary prevention of depressive disorders but also the primary prevention of suicide. However, evidence has been chiefly obtained in clinical settings, which may not apply to community dwellers. The purpose of this study was to evaluate the asso ci- ations between various mental and somatic symptoms and MDD and suicidal risk in a Japanese community, and to establish the key contributing elements that would aid in detecting signs of MDD and suicidal risk in commu nit y dw eller s a t the pr ec lin ica l stag e. 2. METHODS 2.1. Study Population We conducted a cross-sectional study in the following two settings. (Location 1: Health check-up services, A City) A private medical corporation in A City (total popu- lation, approximately 26,000) located in the middle of Wakayama Prefecture, provides health check-up ser- vices for community dwellers and local company em- ployees. Six hundred and s ev en t y-s ix p eople underwent a health check-up at this service from January through March 2008. Out of them, 294 people were contacted and 280 people agreed to participate in the study. (Location 2: B and C Towns) B Town (total population, approximately 8000) and C Town (total population, approximately 7000) are both located in the middle of Wakayama Prefecture. To de tect chronic diseases including metabolic syndrome, these towns provide a health check-up program every year for self-employed community dwellers and their family me mber s each ag ed 40 - 74 years. In 2008, 3656 people aged 40 - 74 years (1809 in B Town; 1847 in C Town) were eligible for the annual health check-up program, and 686 (177 in B Town; 509 in C Town) underw ent a h ealth check -up from May through August, 2008. Of these, 452 people (146 in B Town; 306 in C Town) agreed to participate in the s tud y. Those who underwent a health check-up were asked to participate in the study via posters displayed at the check-up site. Later, they were led one-by-one to the interview room where the structured interviews were conducted. The participants received a detailed oral and written explanation of the study, i.e., regarding the purpose of the study, voluntarity of participation, and principal investigator’s contact address, from the inter- viewers. If they agreed to participate in the study, they gave wr i tten inf or med consent. This study was approved by the ethics committee of Wakayama Medica l Un iver s i ty. 2.2. Data Collection 2.2.1. Psy ch ia t ric Structu red In te rv i ew Mini-International Neuropsychiatric Interview (MINI) Japanese version 5.0.0 (2003) [29,30], a convenient structured diagnostic interview for mental disorders, was used for the interview survey. All questions in- cluded in MINI were coded as two categories on the basis of the respondents’ answers of yes/no. Reliability and validity of the Japanese version of MINI is satis- factory [31]. Nine interviewers (three at location 1 and nine at locat ion 2), al l of who were licens ed physicians or nurses, were enrolled as competent interviewers. They were trained by the second author (KY), a psy- chiatrist, for essential interview skills including didac- tic sessions of a general interview and a review of the instrument sections. Furthermore, the second author checked the interviewers and corrected them as the need arose during the interview sessions so that the interview could be appropriately conducted. MINI considers 17 Axis I mental disorders based on the standard 12-month prevalence of ≥0.5% [29]. Among these 17 disorders, we chose MDD, dysthymia, and suicidal ideation and attempts as candidate disord- ers strongly associated with increasing suicidal risk among community dwellers. Basic questions essential for a diagnosis of MDD (two questions) and dysthymia (one question) were asked to all subjects. If their answers to the basic ques- tions implied the possible presence of MDD or dys- thymia, more detailed questions were asked for a final diagnosis (seven more questions for MDD and up to nine more questions for dysthymia). Suicidal risk was measured on the basis of six rele- vant items included in MINI. Of these, five items con- sidered suicidal ideation and attempts within the pre-  S. Ta ke mura et al. / Open Journal of Psychiatry 1 (2011) 40-48 Copyright © 2011 SciRes. OJPsych vious month ([1] thinking that he/she would be better off dead, [2] thinking about self-harm, [3] thinking about suicide, [4] planning of suicide, and [5] expe- riences of suicide attempts), and the sixth item consi- dered lifetime experiences of suicide attempts. Ac- cording to the weighted value of each question, points 1, 2, 6, 10, and 10 were allotted to each response to the former five questions, and point 4 was allotted to the last response regarding lifetime experiences of suicide attempts. Thus, a score of 33 was the maximum number of points for suicidal risk. A higher score indicates the presence of higher suicidal risk. 2.2.2. M edi cal Ex am inat ion s Each participant at both locations was asked to com- plete a self-administered questionnaire. This question- naire contained items regarding lifestyle factors, the presence or history of chronic diseases as well as their treatment status, and self-reported somatic and mental symptoms. The questionnaire was designed on the basis of a questionnaire proposed by the Ministry of Health, Labor, and Welfare, Japan [32]. Fasting blood samples were collected for biochemical examinations such as plasma glucose, serum LDL or HDL cholesterol, trigly- cerides, and hemoglobin. A urine test and chest radio- graphy were also conducted. A checklist for the self-reported symptoms included various somatic symptoms, such as respiratory, cardi- ovascular, digestive, musculoskeletal, nervous, and urogenital symptoms (21 items for location 1 and 18 items for location 2), and one mental symptom regard- ing agitation or anxiety. Because this checklist was a ready-made review of systems with current symptoms developed by the health check-up service provider, details such as precise duration or frequency and sever- ity of th ese symptoms could not be obtained. However, this checklist included two questions about anxie- ty-related mental and somatic symptoms and one ques- tion about general somatic symptoms from the Hamil- ton Depression Rating Scale (HAM-D17) [33]. Al- though these symptoms were mainly checked for the secondary prevention of chronic diseases, some of them were also considered to reflect the symptoms of soma- toform autonomic dysfunction, which might be related to depression. According to the corresponding res- ponses, the status of these symptoms was simply di- vided into presenc e or absence cat ego r ies. These medical examinations were conducted by a private medical corporation or a local health authority. Psychiatric interviewers were not involved in the med- ical examinations. 2.3. S tatistical Analysis The frequency of subjective symptoms and MDD/suicidal risk were calculated. Then logistic re- gression analysis was used to calculate odds ratios (ORs) and 95% confidence intervals (CIs). In the logis- tic regression analysis, the dependent variables were MDD and suicidal risk. The status of MDD was di- vided into positive and negative c ategories on the basis of MINI results. The status of suicidal risk was also divided into positive and negative categories on the basis of the total score on the corresponding questions included in MINI. Subjects with a zero score were re- garded as negative, and those with a score more than zero wer e regard ed as po sitive. In the s ame mann er, the independent variable was each subjective symptom or mental disorders including MDD. The subjective symptom was divided into positive or negative catego- ries. Each subjective symptom wa s r egard ed as po sitiv e if a subject reported the symptom. Univar iate models wer e created to eva luate th e asso- ciations between each symptom and MDD/s uicidal r isk. We adjusted for gender and age in the multivariate analysis of MDD. Age in years was div ided into t erti les according to the distribution of age in each location. For suicidal risk, we further adjusted for gender, age, and the presence of loss of interest or depressed mood, which are basic symptoms of MDD. These depres- sion-related mental symptoms might be potential con- founding factors regarding the association between somatic symptoms and suicidal risk. P values (two-sided) less than 0.05 were considered statistically significant. All computations were per- formed using the SAS software package, version 9.1.3 (SAS Institute Inc., Cary, NC, USA). 3. RESULTS Table 1 shows ch arac ter istic s of th e stud y sub jec ts. The average age was 45.4 years (range, 17 - 86) at location 1 and 62.5 years (range, 39 - 74) at location 2. The proportion of female subjects was 46% and 60% at locations 1 and 2, respectively. Of all symptoms, head- ache, heavy headedness, eye strain, and shoulder stiff- ness w ere h igh es t in frequency at both locations (26%). Ta b le 2 illustrates the MINI results. The prevalence of MDD was approximately 2% at both locations. The frequency of subjects with at least one of the two basic depressive symptoms was approximately 3% at both locations. Only three subjects (two at location 1 and one at location 2) were positive for dysthymia. Ap- proximately 6% of all study subjects showed suicidal risk. Table 3 revea l s ag e - and gender-adjusted ORs of MDD and dysthymia for suicidal risk. Both depressed mood and loss of interest were significantly associated with suicidal risks at both locations. Melancholic de- pression and dysthymia were also strongly associated 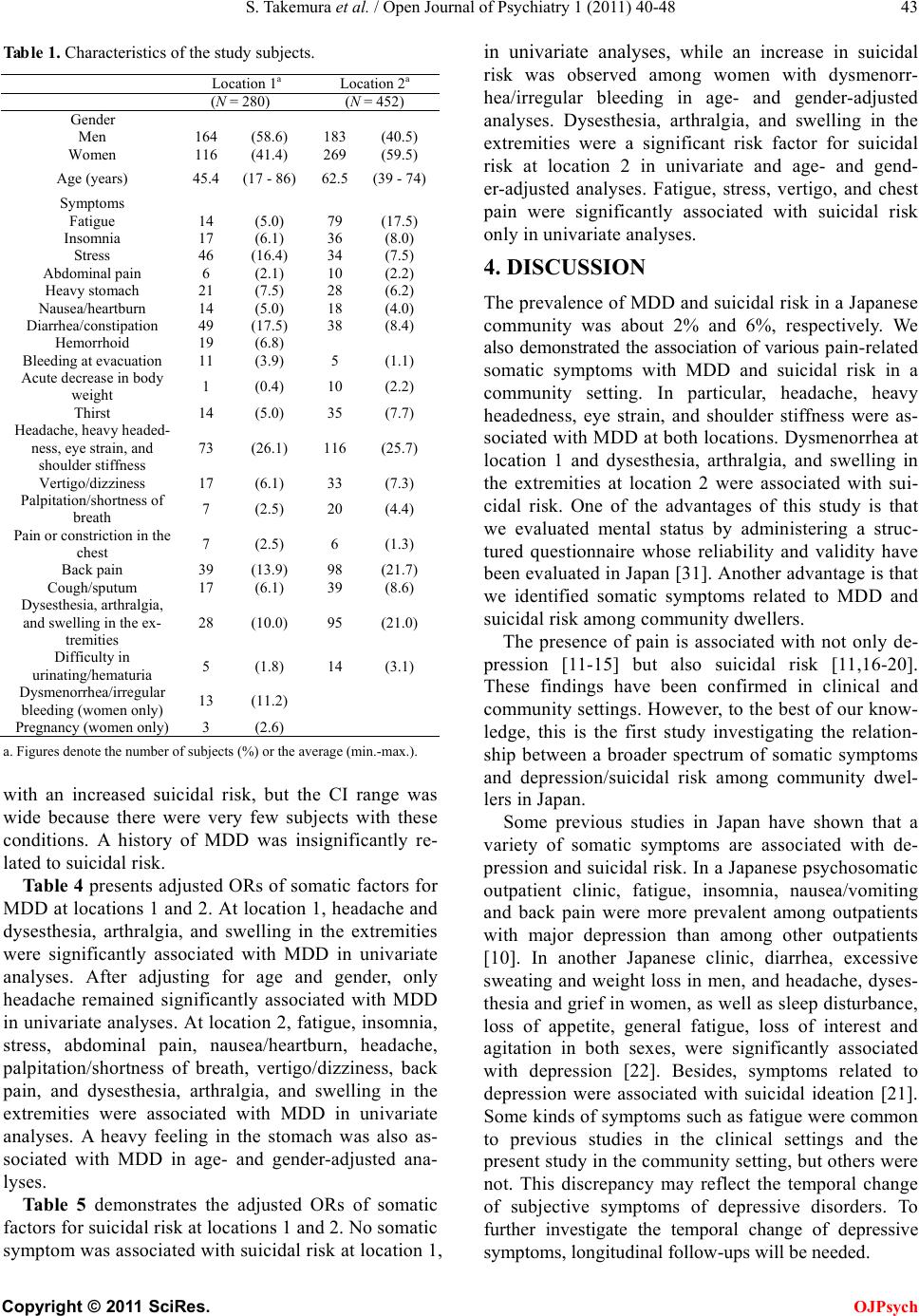 S. Ta ke mura et al. / Open Journal of Psychiatry 1 (2011) 40-48 Copyright © 2011 SciRes. OJPsych Table 1. Characteristics of the study subjects. a. Figures denote the number of subjects (%) or the average (min.-max.). with an increased suicidal risk, but the CI range was wide because there were very few subjects with these conditions. A history of MDD was insignificantly re- lated to suicidal risk. Tabl e 4 presents adjusted ORs of somatic factors for MDD at locations 1 and 2. At location 1, head ache and dysesthesia, arthralgia, and swelling in the extremities were significantly associated with MDD in univariate analyses. After adjusting for age and gender, only headache remained significantly associated with MDD in univar iate anal yses. At loc ation 2, f atigue, in somnia, stress, abdominal pain, nausea/heartburn, headache, palpitation/shortness of breath, vertigo/dizziness, back pain, and dysesthesia, arthralgia, and swelling in the extremities were associated with MDD in univariate analyses. A heavy feeling in the stomach was also as- sociated with MDD in age- and gender-adjusted ana- lyses. Table 5 demonstrates the adjusted ORs of somatic factors for suicidal risk at locations 1 and 2. No somatic symptom was associated with suicid al risk at location 1, in univariate analyses, while an increase in suicidal risk was observed among women with dysmenorr- hea/irregular bleeding in age- and gender-adjusted analyses. Dysesthesia, arthralgia, and swelling in the extremities were a significant risk factor for suicidal risk at location 2 in univariate and age- and gend- er-adjusted analyses. Fatigue, stress, vertigo, and chest pain were significantly associated with suicidal risk only in univariate analyses. 4. DISCUSSION The prevalence of MDD and suicidal risk in a Japanese community was about 2% and 6%, respectively. We also demonstrated the association of various pain-related somatic symptoms with MDD and suicidal risk in a community setting. In particular, headache, heavy headedness, eye strain, and shoulder stiffness were as- sociated with MDD at both lo cations. Dysmenorrhea at location 1 and dysesthesia, arthralgia, and swelling in the extremities at location 2 were associated with sui- cidal risk. One of the advantages of this study is that we evaluated mental status by administering a struc- tured questionnaire whose reliability and validity have been eva luated in Jap an [31]. A nother adv antage is that we identified somatic symptoms related to MDD and suicidal risk among community dwellers. The presence of pain is associated with not only de- pression [11-15] but also suicidal risk [11 ,16-20]. These findings have been confirmed in clinical and community settings. However, to the best of our know- ledge, this is the first study investigating the relation- ship between a broader spectrum of somatic symptoms and depression/suicidal risk among community dwel- lers in J ap an . Some previous studies in Japan have shown that a variety of somatic symptoms are associated with de- pression and suicidal risk. In a J apanese psychosomatic outpatient clinic, fatigue, insomnia, nausea/vomiting and back pain were more prevalent among outpatients with major depression than among other outpatients [10]. In another Japanese clinic, diarrhea, excessive sweating and weight loss in men, and headache, dyses- thesi a and gri ef in wome n, as we ll as sleep distu rbance, loss of appetite, general fatigue, loss of interest and agitation in both sexes, were significantly associated with depression [22]. Besides, symptoms related to depression were associated with suicidal ideation [21]. Some kinds of symptoms such as fatigue were common to previous studies in the clinical settings and the present study in the community setting, but others were not. This discrepancy may reflect the temporal change of subjective symptoms of depressive disorders. To further investigate the temporal change of depressive symptoms, longitudinal follow-ups wi l l be needed. Wome n 116 (41.4) 269 (59.5) Age (years) 45.4 (17 - 86) 62.5 (39 - 74) Insomnia 17 (6.1) 36 (8.0) Diarrhea/constipation 49 (17.5) 38 (8.4) Acute decrease in body weight 1 (0.4) 10 (2.2 ) Thirst 14 (5.0) 35 (7.7) ness, eye strain, and 73 (26.1) 116 (25.7) Palpitation/shortness of breath 7 (2.5) 20 (4.4 ) Pain or constriction in the chest 7 (2.5) 6 (1.3) Cough/sputum 17 (6.1) 39 (8.6) and swelling in the ex- 28 (10.0) 95 (21.0) urinating/hematuria 5 (1.8) 14 (3.1 ) Dysmenorrhea/irregular bleeding (women only) 13 (11.2) 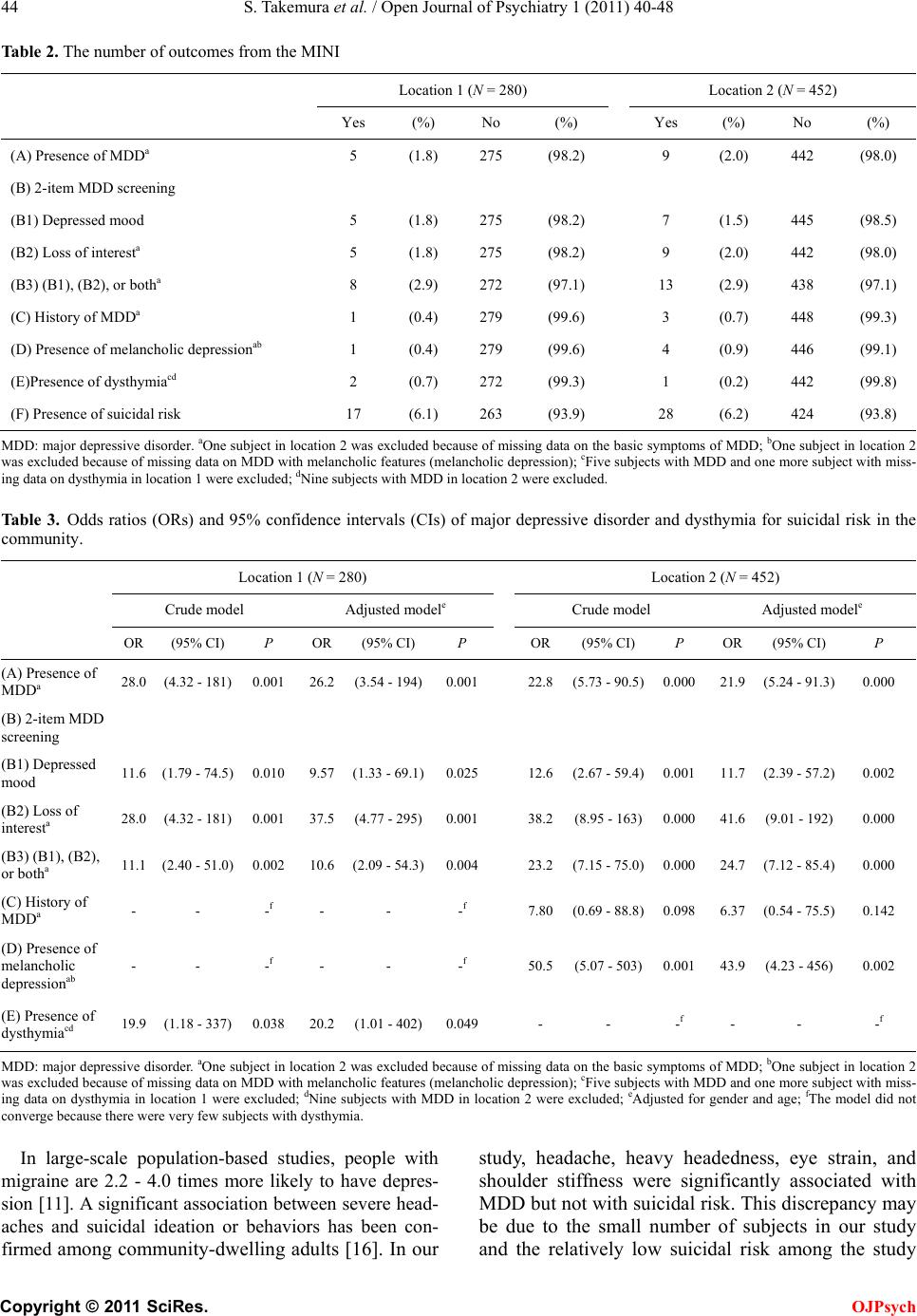 S. Ta ke mura et al. / Open Journal of Psychiatry 1 (2011) 40-48 Copyright © 2011 SciRes. OJPsych Table 2. The number of outcomes from the MINI Location 1 (N = 280) Location 2 (N = 452) Yes (%) No (%) Yes (%) No (%) (A) Presence of MDDa 5 (1.8) 275 (98.2) 9 (2.0) 442 (98.0) (B) 2-item MDD screening (B1) Depre s s ed mood 5 (1.8) 275 (98.2) 7 (1.5) 445 (98.5) (B2) Loss of interesta 5 (1.8) 275 (98.2) 9 (2.0) 442 (98.0) (B3) (B1), (B2), or botha 8 (2.9) 272 (97.1) 13 (2.9) 438 (97.1) (C) History of MDDa 1 (0.4) 279 (99.6) 3 (0.7) 448 (99.3) (D) Presence of melancholic depressionab 1 (0.4) 279 (99.6) 4 (0.9) 446 (99.1) (E)Presence of dysthymiacd 2 (0.7) 272 (99.3) 1 (0.2) 442 (99.8) (F) Presence of suicidal risk 17 (6.1) 263 (93.9) 28 (6.2) 424 (93.8) MDD: major depressiv e disorder . aOne subject in locatio n 2 was exclu ded because o f missing data on the basic symptoms of MDD; bOne su bject in lo cation 2 was excluded because of missing data on MDD with melancho li c featu r es ( melan cho li c dep res sio n); cFive subjects with MDD and one more subject with miss- ing data on dysthymia i n l ocation 1 were excluded; dNine subjects with MDD in location 2 were excluded. Table 3. Odds ratios (ORs) and 95% confidence intervals (CIs) of major depressive disorder and dysthymia for suicidal risk in the community. Location 1 (N = 280) Location 2 (N = 452) Crude model Adjusted modele Crude model Adjusted modele OR (95% CI) P OR (95% CI) P OR (95% CI) P OR (95% CI) P (A) Presence of MDDa 28.0 (4.32 - 181) 0.001 26.2 (3.54 - 194) 0.001 22.8 (5.73 - 90.5) 0.000 21.9 (5.24 - 91.3) 0.000 (B) 2-item MDD screening (B1) Depressed mood 11.6 (1.79 - 74.5) 0.010 9.57 (1.33 - 69.1) 0.025 12.6 (2.67 - 59.4) 0.001 11.7 (2.39 - 57.2) 0.002 (B2) Loss of interesta 28.0 (4.32 - 181) 0.001 37.5 (4.77 - 295) 0.001 38.2 (8.95 - 163) 0.000 41.6 (9.01 - 192) 0.000 (B3) (B1), (B2), or botha 11.1 (2.40 - 51.0) 0.002 10.6 (2.09 - 54.3) 0.004 23.2 (7.15 - 75.0) 0.000 24.7 (7.12 - 85.4) 0.000 (C) History of MDDa - - -f - - -f 7.80 (0.69 - 88.8) 0.098 6.37 (0.54 - 75.5) 0.142 (D) Presence of melancholic depressionab - - -f - - -f 50.5 (5.07 - 503) 0.001 43.9 (4.23 - 456) 0.002 (E) Presence of dysthymi a cd 19.9 (1.18 - 337) 0.038 20.2 (1.01 - 402) 0.049 - - -f - - -f MDD: major depressiv e disorder. aOne subject in l ocation 2 was excluded because of missing d ata on the basic symptoms of MDD; bOne sub ject in locat ion 2 was exclu ded b ecaus e of mis si ng dat a on MDD wi th melan ch o lic f eatu res (m elan cho li c dep res sio n); cFive subjects with MDD and one more subject with miss- ing data on dysthymia in location 1 were excluded; dNine su bjects with MDD in location 2 were ex cluded; eAdjusted for gender and age; fThe model did not converge because there were very few subjects with dysthymia. In large-scale population-based studies, people with migraine are 2.2 - 4.0 times more likely to have depres- sion [11 ]. A significant association between severe head- aches and suicidal ideation or behaviors has been con- firmed among community-dwelling adults [16]. In our study, headache, heavy headedness, eye strain, and shoulder stiffness were significantly associated with MDD but not with suicidal risk. This discrepancy may be due to the small number of subjects in our study and the relatively low suicidal risk among the study 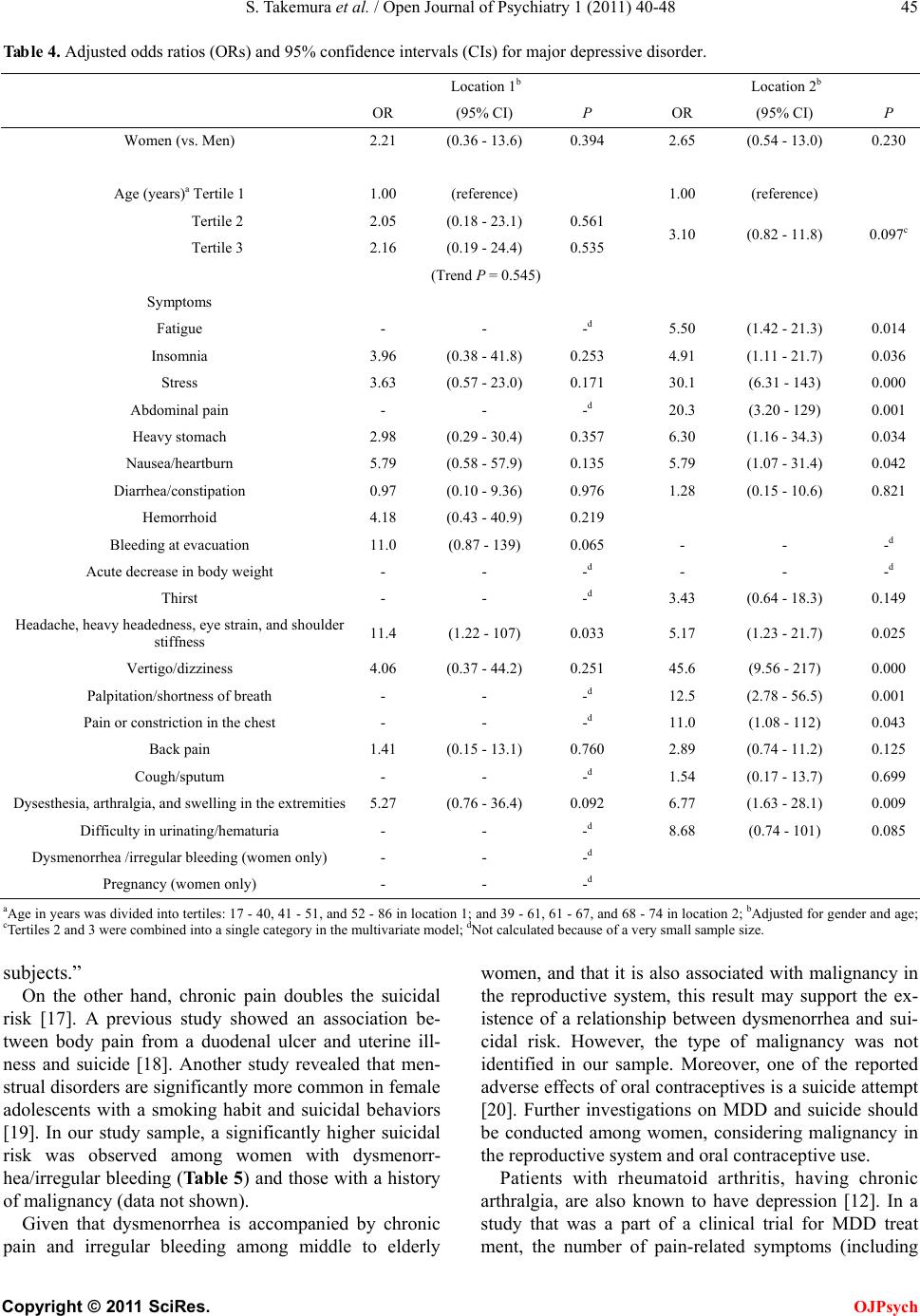 S. Ta ke mura et al. / Open Journal of Psychiatry 1 (2011) 40-48 Copyright © 2011 SciRes. OJPsych Table 4. Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for major depressive disorder. Location 1b Location 2b OR (95% CI) P OR (95% CI) P Women (vs. Men) 2.21 (0.36 - 13.6) 0.394 2.65 (0.54 - 13.0) 0.230 Age (years)a Tertile 1 1.00 (reference) 1.00 (reference) Tertile 2 2.05 (0.18 - 23.1) 0.561 3.10 (0.82 - 11.8) 0.097c Tertile 3 2.16 (0.19 - 24.4) 0.535 (Trend P = 0.545) Symptoms Fatigue - - -d 5.50 (1.42 - 21.3) 0.014 Insomnia 3.96 (0.38 - 41.8) 0.253 4.91 (1.11 - 21.7) 0.036 Stress 3.63 (0.57 - 23.0) 0.171 30.1 (6.31 - 143) 0.000 Abdominal pain - - -d 20.3 (3.20 - 129) 0.001 Heavy stomach 2.98 (0.29 - 30.4) 0.357 6.30 (1.16 - 34.3) 0.034 Nausea/heartburn 5.79 (0.58 - 57.9) 0.135 5.79 (1.07 - 31.4) 0.042 Diarrhea/constipation 0.97 (0.10 - 9.36) 0.976 1.28 (0.15 - 10.6) 0.821 Hemorrhoid 4.18 (0.43 - 40.9) 0.219 Bleeding at evacuation 11.0 (0.87 - 139) 0.065 - - -d Acute decrease in body weight - - -d - - -d Thirst - - -d 3.43 (0.64 - 18.3) 0.149 Headache, heavy headedness, eye strain, and shoulder stiffness 11.4 (1.22 - 107) 0.033 5.17 (1.23 - 21.7) 0.025 Vertigo/dizziness 4.06 (0.37 - 44.2) 0.251 45.6 (9.56 - 217) 0.000 Palpitation/shortness of breath - - -d 12.5 (2.78 - 56.5) 0.001 Pain or constriction in the chest - - -d 11.0 (1.08 - 112) 0.043 Back pain 1.41 (0.15 - 13.1) 0.760 2.89 (0.74 - 11.2) 0.125 Cough/sputum - - -d 1.54 (0.17 - 13.7) 0.699 Dysesthesia, arthralgia, and swelling in the extremities 5.27 (0.76 - 36.4) 0.092 6.77 (1.63 - 28.1) 0.009 Difficulty in urinating/hematuria - - -d 8.68 (0.74 - 101) 0.085 Dysmenorrhea /irregular bleeding (women only) - - -d Pregnancy (women only) - - -d aAge in years was divided into tertiles: 17 - 40, 41 - 51, and 52 - 86 in location 1; and 39 - 61, 61 - 67, and 68 - 74 in location 2; bAdjusted for gender and age; cTertiles 2 and 3 were combined into a single category in the multivariate model; dNot calculated because of a very small sample size. subjects.” On the other hand, chronic pain doubles the suicidal risk [17]. A previous study showed an association be- tween body pain from a duodenal ulcer and uterine ill- ness and suicide [18]. Another study revealed that men- strual disorders are significantly more common in female adolescents with a smoking habit and suicidal behaviors [19]. In our study sampl e, a significantly higher suicidal risk was observed among women with dysmenorr- hea/irregular bleedin g (Table 5) and those with a h istory of mali gna nc y (data n ot sh own). Given that dysmenorrhea is accompanied by chronic pain and irregular bleeding among middle to elderly women, and that it is also associated with malignancy in the reproductive system, this result may support the ex- istence of a relationship between dysmenorrhea and sui- cidal risk. However, the type of malignancy was not identified in our sample. Moreover, one of the reported adverse effects of oral contraceptives is a suicide attempt [20]. Further investigations on MDD and suicide should be conducted among women, considering malignancy in the reproductive system and oral contraceptive use. Patients with rheumatoid arthritis, having chronic arthralgia, are also known to have depression [12]. In a study that was a part of a clinical trial for MDD treat ment, the number of pain-related symptoms (including 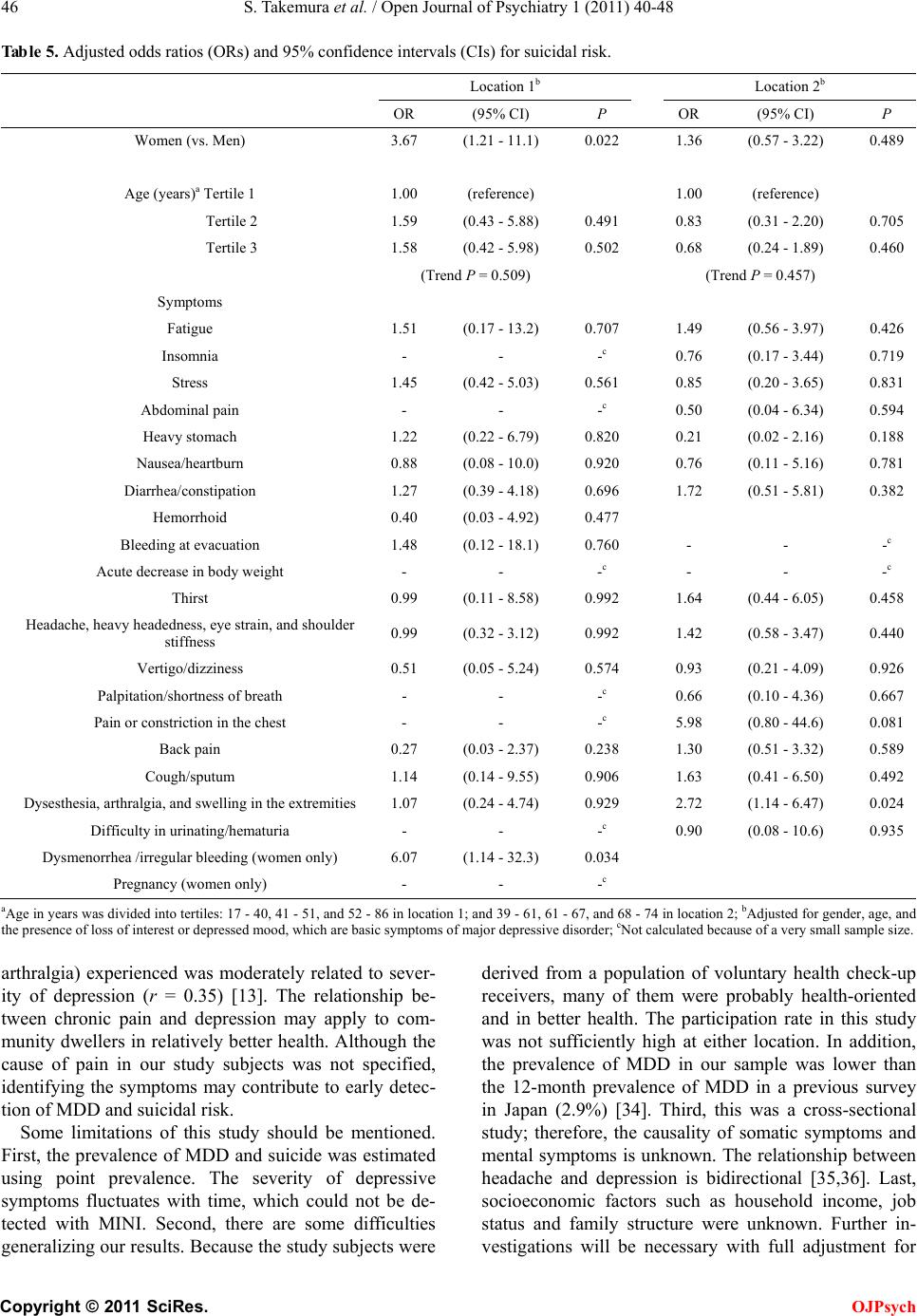 S. Ta ke mura et al. / Open Journal of Psychiatry 1 (2011) 40-48 Copyright © 2011 SciRes. OJPsych Table 5. Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for suicidal risk. Location 1b Location 2b OR (95% CI) P OR (95% CI) P Women (vs. Men) 3.67 (1.21 - 11.1) 0.022 1.36 (0.57 - 3.22) 0.489 Age (years)a Tertile 1 1.00 (reference) 1.00 (reference) Tertile 2 1.59 (0.43 - 5.88) 0.491 0.83 (0.31 - 2.20) 0.705 Tertile 3 1.58 (0.42 - 5.98) 0.502 0.68 (0.24 - 1.89) 0.460 (Trend P = 0.509) (Trend P = 0.457) Symptoms Fatigue 1.51 (0.17 - 13.2) 0.707 1.49 (0.56 - 3.97) 0.426 Insomnia - - -c 0.76 (0.17 - 3.44) 0.719 Stress 1.45 (0.42 - 5.03) 0.561 0.85 (0.20 - 3.65) 0.831 Abdominal pain - - -c 0.50 (0.04 - 6.34) 0.594 Heavy stomach 1.22 (0.22 - 6.79) 0.820 0.21 (0.02 - 2.16) 0.188 Nausea/heartburn 0.88 (0.08 - 10.0) 0.920 0.76 (0.11 - 5.16) 0.781 Diarrhea/constipation 1.27 (0.39 - 4.18) 0.696 1.72 (0.51 - 5.81) 0.382 Hemorrhoid 0.40 (0.03 - 4.92) 0.477 Bleeding at evacuation 1.48 (0.12 - 18.1) 0.760 - - -c Acute decrease in body weight - - -c - - -c Thirst 0.99 (0.11 - 8.58) 0.992 1.64 (0.44 - 6.05) 0.458 Headache, heavy headedness, eye strain, and shoulder stiffness 0.99 (0.32 - 3.12) 0.992 1.42 (0.58 - 3.47) 0.440 Vertigo/dizziness 0.51 (0.05 - 5.24) 0.574 0.93 (0.21 - 4.09) 0.926 Palpitation/shortness of breath - - -c 0.66 (0.10 - 4.36) 0.667 Pain or constriction in the chest - - -c 5.98 (0.80 - 44.6) 0.081 Back pain 0.27 (0.03 - 2.37) 0.238 1.30 (0.51 - 3.32) 0.589 Cough/sputum 1.14 (0.14 - 9.55) 0.906 1.63 (0.41 - 6.50) 0.492 Dysesthesia, arthralgia, and swelling in the extremities 1.07 (0.24 - 4.74) 0.929 2.72 (1.14 - 6.47) 0.024 Difficulty in urinating/hematuria - - -c 0.90 (0.08 - 10.6) 0.935 Dysmenorrhea /irregular bleeding (women only) 6.07 (1.14 - 32.3) 0.034 Pregnancy (women only) - - -c aAge in years was divided into tertiles: 17 - 40, 41 - 51, and 52 - 86 in location 1; and 39 - 61, 61 - 67, and 68 - 74 in location 2; bAdjusted for gender, age, and the presence of loss of int erest or depr essed mood, which are basic symptoms of major depressive disorder; cNot calculated because of a very small sample size. arthralgia) experienced was moderately related to sever- ity of depression (r = 0.35) [13]. The relationship be- tween chronic pain and depression may apply to com- munity dwellers in relatively better health. Although the cause of pain in our study subjects was not specified, identifying the symptoms may contribute to early detec- tion of MDD and suicidal risk. Some limitations of this study should be mentioned. First, the prevalence of MDD and suicide was estimated using point prevalence. The severity of depressive symptoms fluctuates with time, which could not be de- tected with MINI. Second, there are some difficulties generalizing our results. Because the study subjects were derived from a population of voluntary health check-up receivers, many of them were probably health-oriented and in better health. The participation rate in this study was not sufficiently high at either location. In addition, the prevalence of MDD in our sample was lower than the 12-month prevalence of MDD in a previous survey in Japan (2.9%) [34]. Third, this was a cross-sectional study; therefore, the causality of somatic symptoms and mental symptoms is unknown. The relationship between headache and depression is bidirectional [35,36]. Last, socioeconomic factors such as household income, job status and family structure were unknown. Further in- vestigations will be necessary with full adjustment for  S. Ta ke mura et al. / Open Journal of Psychiatry 1 (2011) 40-48 Copyright © 2011 SciRes. OJPsych those factors and with longitudinal follow-ups. In conclusion, a strong link between various somatic symptoms, including pain-related symptoms, and MDD and/or suicidal risk was observed among community dwellers. Early detection of depressive symptoms in the community or in primary care may have an impact on the prevalence of MDD and suicide rates in Ja pan. Given that a large proportion of patients with depression visit a physician rather than a psychiatrist, our findings may help physicians engaged in primary care to identify pa- tients with MDD or suicidal risk. REFERENCES [1] Sechter, D., Bonin, B., Bertschy, G., Vandel, S. and Bi- zouard, P. (1991) Prediction of suicide risk. In French, Encephale, 17, 361-364. [2] Hall, R.C., Platt, D.E. and Hall, R.C. (1999) Suicide risk assessment: A review of risk factors for suicide in 100 patients who made severe suicide attempts. Evaluation of suicide risk in a time of managed care. P sychosomatics, 40, 18-27. [3] Aihara, H. and Iki, M. (2003) An ecological study of the relations between the recent high suicide rates and eco- nomic and demographic factors in Japan. Journal of Ep- idemiology, 13, 56-61. [4] Nishi, N., Kurosawa, M., Nohara, M., Oguri, S., Chida, F., Otsuka, K., Sakai, A. and Okayama, A. (2005) Know- ledge of and attitude toward suicide and depression among Japanese in municipalities with high suicide rates. Journal of Epidemiology, 15, 48-55. doi:10.2188/jea.15.48 [5] Fushimi, M., Sugawara, J. and Shimizu, T. (2005) Sui- cide patterns and characteristics in Akita, Japan. Psy- chiatry and Clinical Neurosciences, 59, 296-302. doi:10.1111/j.1440-1819.2005.01374.x [6] Awata, S., Seki, T., Koizumi, Y., Sato, S., Hozawa, A., Omori, K., Kuriyama, S., Arai, H., Nagatomi, R., Mat- suoka, H. and Tsuji, I. (2005) Factors associated with suicidal ideation in an elderly urban Japanese population: A community-based, cross-sectional study. Psychiatry and Clinical Neurosciences, 59, 327-336. doi:10.1111/j.1440-1819.2005.01378.x [7] Fujioka, S., Abe, S. and Hiraiwa, K. (2004) Lifetime social, psychological and physical background of sui- cides-Research on the number of suicides during a year in Fukushima Prefecture. In Japanese, Seishin Shinkei- gaku Zasshi, 106, 17-31. [8] Okuma, H. (2008) Modern Clinical Psychiatry. In Japa- nese, 11th Edition, Kanahara Press, Tokyo, 448. [9] Bertolote, J.M., Fleischmann, A., De Leo, D. and Wa- sserman, D. (2004) Psychiatric diagnoses and suicide: Re-visiting the evidence. Crisis, 25, 147-155. doi:10.1027/0227-5910.25.4.147 [10] Nakao, M., Yamanaka, G. and Kuboki, T. (2001) Major depression and somatic symptoms in a mind/body medi- cine cli ni c. Psychopathology, 34, 230-235. doi:10.1159/000049315 [11] Pompili, M., Di Cosimo, D., Innamorati, M., Lester, D., Tatarelli, R. and Martelletti, P. (2009) Psychiatric comor- bidity in patients with chronic daily headache and mi- graine: A selective overview including personality traits and suicide risk. The Journal of Headache and Pain, 10, 283-290. doi:10.1007/s10194-009-0134-2 [12] Miwa, Y., Yajima, N., Shiozawa, F., Yoda, Y., Hanaoka, R., Hanyuda, M., Hosaka, M., Kasama, T., Negishi, M., Ide, H. and Adachi, M. (2002) Relationship between psychological factors and arthralgia in patients with rheumatoid arthritis. Modern Rheumatology, 12, 32-36. doi:10.1007/s101650200005 [13] Vaccarino, A.L., Sills, T.L., Evans, K.R. and Kalali, A.H. (2009) Multiple pain complaints in patients with major depressive disorde r. Psychosomatic Medicine, 71, 159-162. doi:10.1097/PSY.0b013e3181906572 [14] Benseñor, I.M., Tófoli, L.F. and Andrade, L. (2003) Headache complaints associated with psychiatric comor- bidity in a population-based sample. Brazilian Journal of Medical and Biological Research, 36, 1425-1432. doi:10.1590/S0100-879X2003001000021 [15] Demyttenaere, K., Bruffaerts, R., Lee, S., Posada-Villa, J., Kovess, V., Angermeyer, M.C., Levinson, D., de Girola- mo, G., Nakane, H., Mneimneh, Z., Lara, C., de Graaf, R., Scott, K.M., Gureje, O., Stein, D.J., Haro, J.M., Bromet, E.J., Kessler, R.C., Alonso, J. and Von Korff, M. (2007) Mental disorders among persons with chronic back or neck pain: Results from the World Mental Health Sur- vey s. Pain, 129, 332-342. doi:10.1016/j.pain.2007.01.022 [16] Woolley, S.B., Fredman, L., Goethe, J.W., Lincoln, A.K. and Heeren, T. (2008) Headache complaints and the risk of suicidal thoughts or behaviors. The Journal of Nervous and Mental Disease, 196, 822-828. doi:10.1097/NMD.0b013e31818b4e4f [17] Tang, N.K. and Crane, C. (2006) Suicidality in chronic pain: A review of the prevalence, risk factors and psy- chological links. Psychological Medicine, 36, 575-586. doi:10.1017/S0033291705006859 [18] Venkoba Rao, A. (1990) Physical illness, pain, and sui- cidal behavior. Crisis, 11, 48-56. [19] Lee, L.K., Chen, P.C., Lee, K.K. and Kaur, J. (2006) Menstruation among adolescent girls in Malaysia: A cross-sectional school survey. Singapore Medical Jour- nal, 47, 869-874. [20] McCain, J.R. (1967) Clinical criticism of the oral con- traceptive pills. Transactions of the New England Obste- trical and Gynecological Society, 21, 115-129. [21] Yoshimasu, K., Kondo, T., Tokunaga, S., Kanemitsu, Y., Sugahara, H., Akamine, M., Fujisawa, K., Miyashita, K. and Kubo, C. (2009) Mental and somatic symptoms re- lated to suicidal ideation in patients visiting a psychoso- matic clinic in Japan. International Journal of General Medicine, 2, 163-170. doi:10.2147/IJGM.S6631 [22] Sugahara, H., Akamine, M., Kondo, T., Fujisawa, K., Yoshimasu, K., Tokunaga, S. and Kubo, C. (2004) So- matic symptoms most often associated with depression in an urban hospital medical setting in Japan. Psychiatry Research, 128, 305-311. doi:10.1016/j.psychres.2004.06.015 [23] Marcus, S.M., Kerber, K.B., Rush, A.J., Wisniewski, S.R., Nierenberg, A., Balasubramani, G.K., Ritz, L., Kornstein, S., Young, E.A. and Trivedi, M.H. (2008) Sex differences in depression symptoms in treatment-seeking adults:  S. Ta ke mura et al. / Open Journal of Psychiatry 1 (2011) 40-48 Copyright © 2011 SciRes. OJPsych Confirmatory analyses from the sequenced treatment al- ternatives to relieve depression study. Comprehensive Psychiatry, 49, 238-246. doi:10.1016/j.comppsych.2007.06.012 [24] Dennis, M., Baillon, S., Brugha, T., Lindesay, J., Stewart, R. and Meltzer, H. (2009) The influence of limitation in activity of daily living and physical health on suicidal ideation: Results from a population survey of Great Brit- ain. Social Psychiatry and Psychiatric Epidemiology, 44, 608-613. doi:10.1007/s00127-008-0474-2 [25] Miki, O. (2002) The clinical feature of depression with psychosomatic medicine in primary care. In Japanese, Japanese Journal of Psychosomatic Medicine, 42, 585-591. [26] Feldman, M.D., Franks, P., Duberstein, P.R., Vannoy, S., Epstein, R. and Kravitz, RL. (2007) Let’s not talk about it: Suicide inquiry in primary care. Annals of Family Medicine, 5, 412-418. doi:10.1370/afm.719 [27] Griffiths, K.M., Nakane, Y., Christensen, H., Yoshioka, K., Jorm, A.F. and Nakane, H. (2006) Stigma in response to mental disorders: A comparison of Australia and Japan. BMC Psychiatry, 6, 21. doi:10.1186/1471-244X-6-21 [28] Kawakami, N., Takeshima, T., Ono, Y., Uda, H., Nakane, Y., Nakamura, Y., Tachimori, H., Iwata, N., Nakane, H., Watanabe, M., Naganuma, Y., Furukawa, T.A., Hata, Y., Kobayashi, M., Miyake, Y. and Kikkawa, T. (2008) Twelv e-month prevalence, severity, and treatment of common mental disorders in communities in Japan: The World Mental Health Japan 2002-2004 Survey. In: Kess- ler, R.C. and Üstün, T.B., Eds., The WHO World Mental Health Surveys, Cambridge University Press, New York, 474-485. [29] Sheehan, D.V., Lecrubier, Y., Sheehan, K.H., Amorim, P., Janavs, J., Weiller, E., Hergueta, T., Baker, R. and Dun- bar, G.C. (1998) The Mini-international neuropsychiatric interview: The development and validation of a struc- tured diagnostic psychiatric interview for DSM-IV and ICD-10. The Journal of Clinical Psychiatry, 59, 22-33. [30] Sheehan, D.V., Lecrubier, Y., Otsubo, T., Miyaoka, H. and Kamijima, K. (2003) Mini-international neuropsy- chiatric interview Japanese version 5.0.0. In Ja panese, Seiwa Shoten Publishers, Tokyo. [31] Otsubo, T., Tanaka, K., Koda, R., Shinoda, J., Sano, N., Tanaka, S., Aoyama, H., Mimura, M. and Kamijima, K. (2005) Reliability and validity of Japanese version of the Mini-international neuropsychiatric interview. Psychiatry and Clinical Neurosciences, 59, 517-526. doi:10.1111/j.1440-1819.2005.01408.x [32] Ministry of Health, Labor and Welfare, Japan. (2007) Standard program for health screening and education (fi- nal version). http://www.mhlw.go.jp/bunya/shakaihosho/iryouseido01/ info03a.html [33] Hamilton, M. (1967) Development of a social scale for primary depressive illness. The British Journal of Social and Clinical Psychology, 6, 278-296. [34] Kawakami, N., Takeshima, T., Ono, Y., Uda, H., Hata, Y., Nakane, Y., Nakane, H., Iwata, N., Furukawa, T.A. and Kikkawa, T. (2005) Twelve-month prevalence, severity, and treatment of common mental disorders in communi- ties in Japan: preliminary finding from the World Mental Health Japan Survey 2002-2003. Psychiatry and Clinical Neurosciences, 59, 441-452. doi:10.1111/j.1440-1819.2005.01397.x [35] Breslau, N., Lipton, R.B., Stewart, W.F., Schultz, L.R. and Welch, K.M. (2003) Comorbidity of migraine and depression: Investigating potential etiology and progno- sis. Neurology, 60, 1308-1312. [36] Bigal, M.E. and Lipton, R.B. (2006) Modifiable risk factors for m igrai ne prog ression . Head ache, 46, 1334-1343. doi:10.1111/j.1526-4610.2006.00577.x
|