C.-M. Yip et al.
Rathke cleft cysts have been found incidentally in 11% - 33% of post-mortem examinations, and were asso-
ciated with 1.7% - 2.1% of the pituitary adenoma cases [1]-[3] [8]. The relationship between Rathke cleft cyst
and pituitary adenoma is still co ntroversial [1] [3]. Associations between these two lesions have been reporte d to
be only occasional and coincidental [3]. Although Rathke cleft cyst and pituitary adenoma have a common em-
bryological ancestry, a pituitary adenoma and a concomitant Rathke cleft cyst rarely occurs. The diagnosis of
Rathke cleft cyst with a co existing pituitary adeno ma is difficult before surg ery because Rathke clef t cysts show
variable size, position and signal intensity on MRI. Nevertheless, the presence of a non-enhancing cyst with a
pituitary adenoma suggests the possibility of an accompanying Rathke cleft cyst [2] [9]. Treatment of this un-
usual coexisting lesion involves surgical resection to decrease mass effect and medical management to normal-
ize hormonal imbalances [2].
4. Conclusion
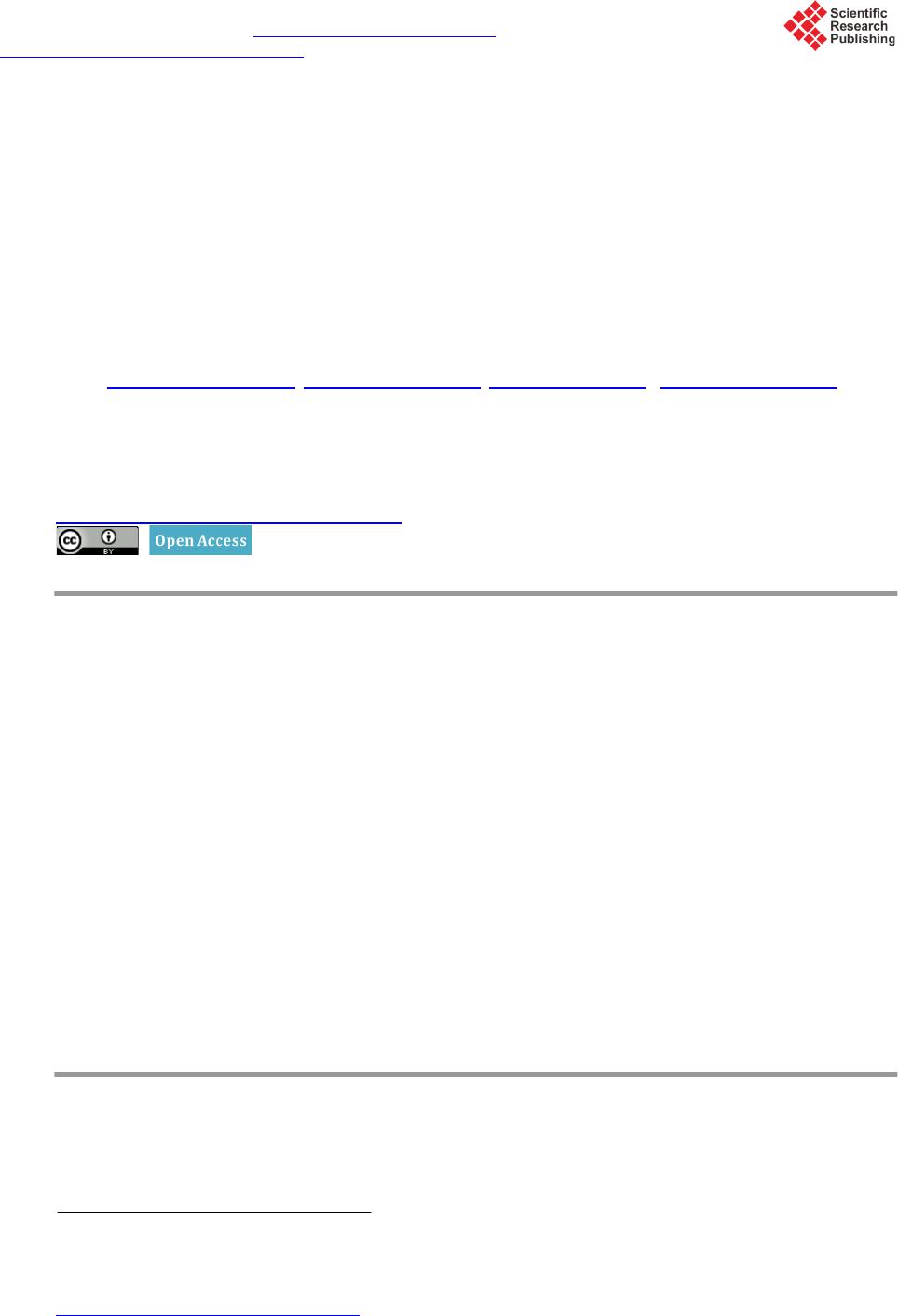
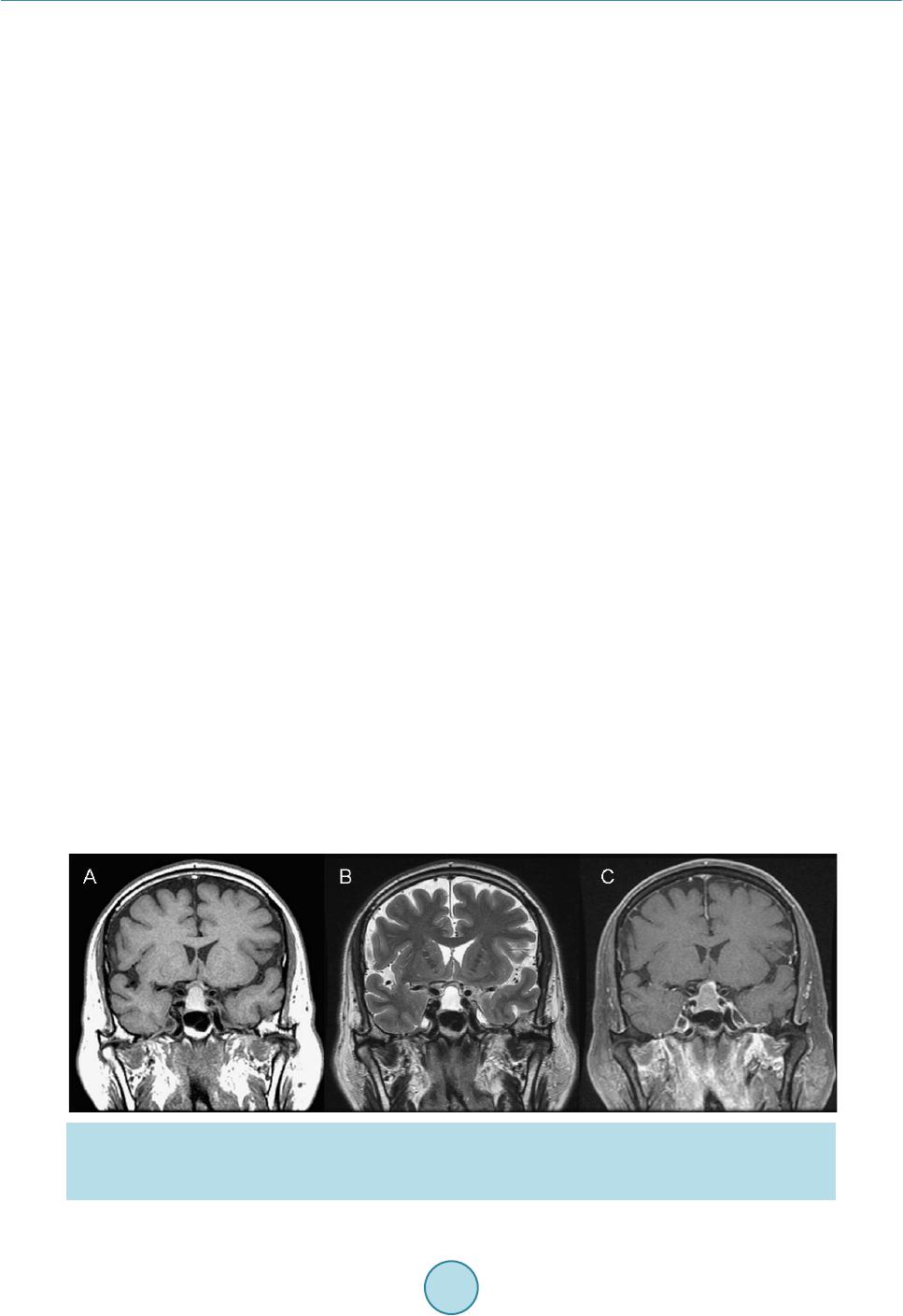
Our patient was diagnosed to have a sellar cystic lesion with suprasellar extension in 2007. This lesion pro-
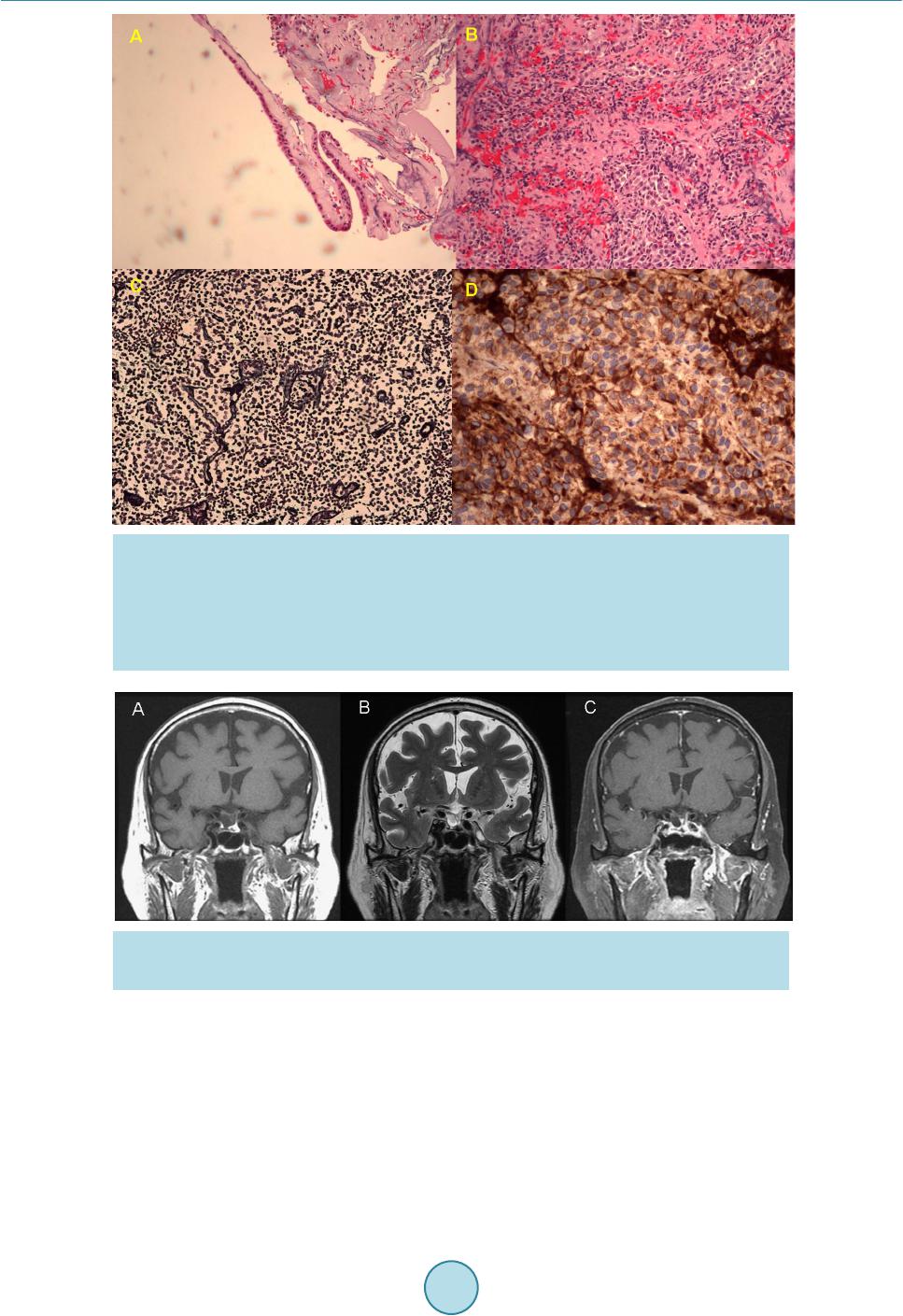
gressed and let him to have significant visual and endocrine dysfunction in 2013. He was successfully treated by
endoscopic endonasal transsphenoidal approach with the removal of the sellar lesion and temporary hormone
replacement. His bitemporal hemianopia was resolved after surgery and his hormonal imbalance was recovered
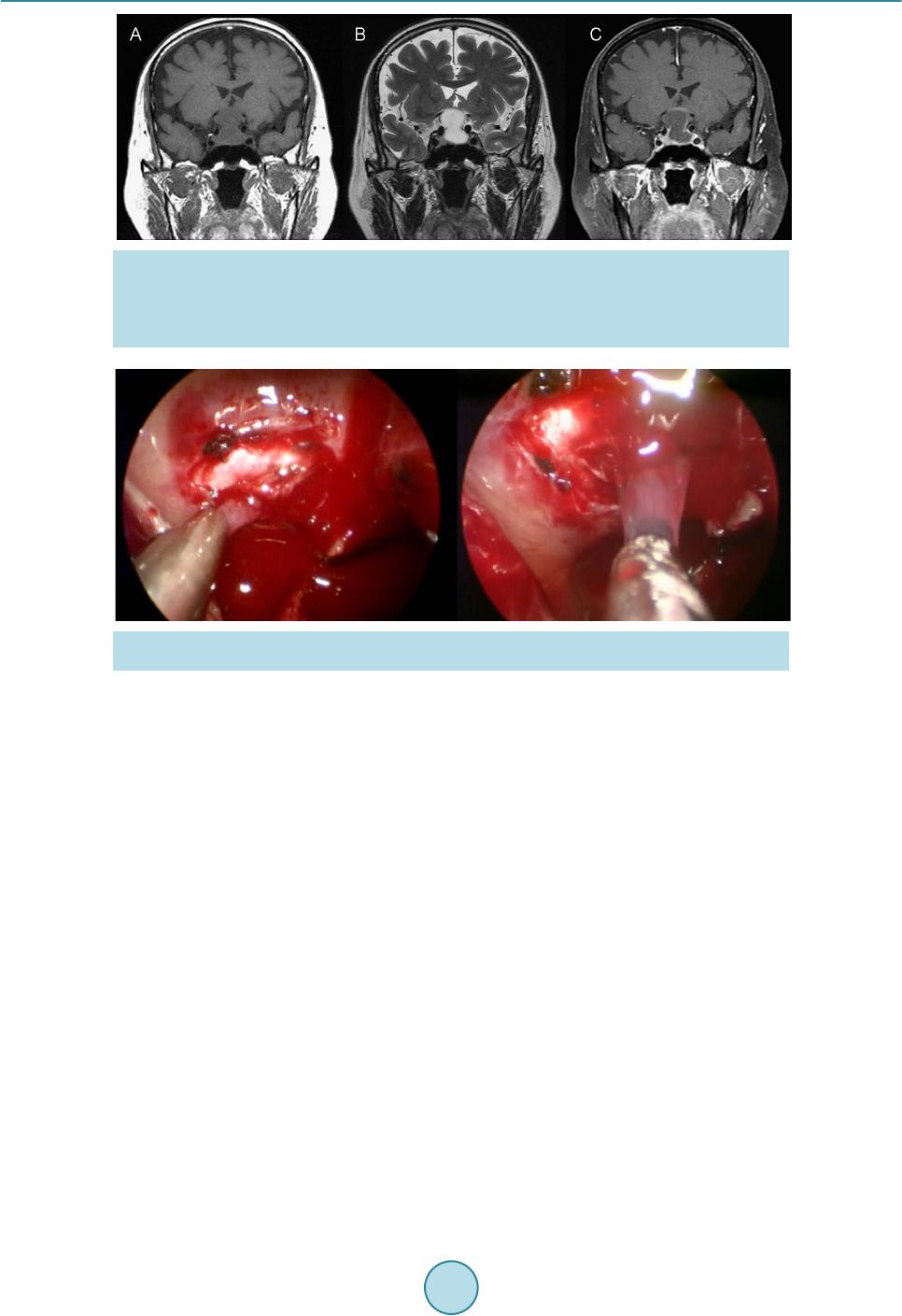
during the follow-up. The histological examination of the sellar cystic lesi on proved to be Rathke cleft cyst with
a coexistent gonadotropin producing adenoma which probably is the first reported combination.
References
[1] Riva, G., Meli, G.A., Chiaramonte, R., et al. (2007) Imaging of Rathke’s Cleft Cysts: Criteria for a Differential Diag-
nosis. The Neuroradiology Journal, 20, 617-621. http://dx.doi.org/10.1177/197140090702000602
[2] Babu, R., Back, A.G., Komisarow, J.M., et al. (2013) Symptomatic Rathke’s Cleft Cyst with a Co-Existing Pituitary
Tumor; Brief Review of the Literature. Asian Journal of Neurosurgery, 8, 183-187.
http://dx.doi.org/10.4103/1793-5482.125662
[3] Sumida, M., Arita, K., Migita, K., et al. (2001) Concomitant Pituitary Adenoma and Rathke’s Cleft Cyst. Neuroradi-
ology, 43, 755-759. http://dx.doi.org/10.1007/s002340100559
[4] Kasperbauer, J.L., Orvidas, L.J., Atkinson, J.L.D., et al. (2002) Rathke Cleft Cyst: Diagnostic and Therapeutic Con-
siderations. Laryngoscope, 112, 1836-1839. http://dx.doi.org/10.1097/00005537-200210000-00024
[5] You, C., Qiao, F., Jiang, S. and Xiao, A.Q. (2012) Growth Hormone Secreting Pituitary Adenoma Associated with
Rathke’s Cleft Cyst. Neurology India, 60, 310-311. http://dx.doi.org/10.4103/0028-3886.98521
[6] Wang, K., Ma, L. and You, C. (2012) Pituitary Adenoma and Concomitant Rathke’s Cleft Cyst: A Case Report and
Review of the Literature. Neurology India, 60, 309-310. http://dx.doi.org/10.4103/0028-3886.98520
[7] Zada, G. (2011) Rathke Cleft Cysts: A Review of Clinical and Surgical Management. Neurosurgical Focus, 31, 1-6.
http://dx.doi.org/10.3171/2011.5.FOCUS1183
[8] Gessler, F., Coon, V.C., Chin, S.S. and Couldwell, W.T. (2011) Coexisting Rathke Cleft Cyst and Pituitary Adenoma
Presenting with Pituitary Apoplexy: Report of Two Cases. Sku ll Base Reports, 1, 99-104.
http://dx.doi.org/10.1055/s-0031-1280737
[9] Noh, S.J., Ahn, J.Y., Lee, K.S. and Kim, S.H. (2007) Pituitary Adenoma and Concomitant Rathke’s Cleft Cyst. Acta
Neurochirurgica, 149, 1223-1228. http://dx.doi.org/10.1007/s00701-007-1295-x