H. Fletcher et al. / Open Journal of Obstetrics and Gynecology 1 (2011) 64-69
68
that misoprostol indu ction may be a useful alternative to
emergency caesarean section in these very ill patients.
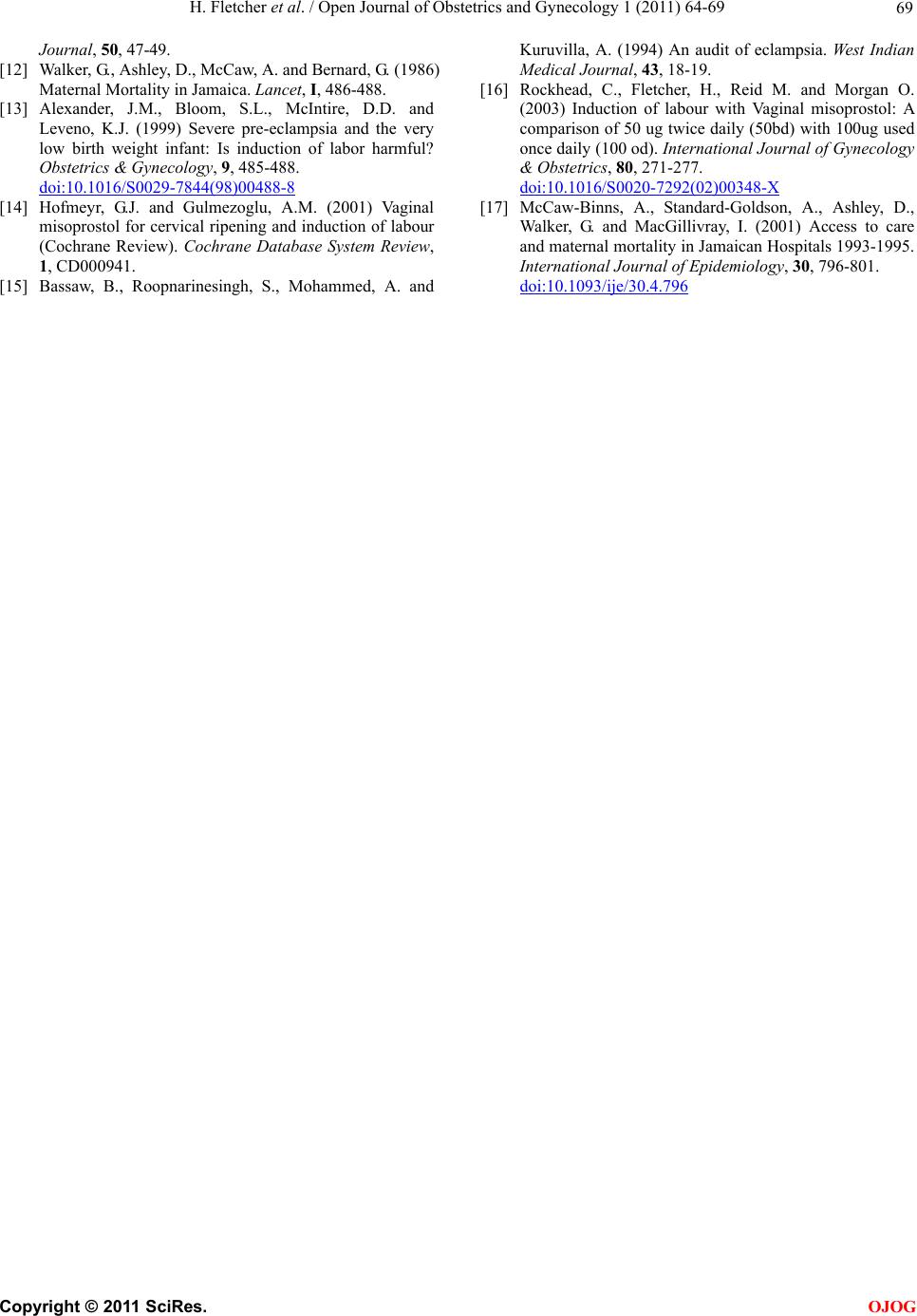
The frequency of failure to progress and failed induc-
tion was the same in both groups, so the introduction of
misoprostol did not have a significant impact as ex-
pected and thus show a beneficial effect over the era
with oxytocin induction only. There were also signifi-
cantly more cases of fetal distress in the latter group. An
earlier study had found an association between the inci-
dence of fetal distress and Misoprostol when used in
doses greater than 25ug [7] and this has been a constant
finding of most large studies [10].
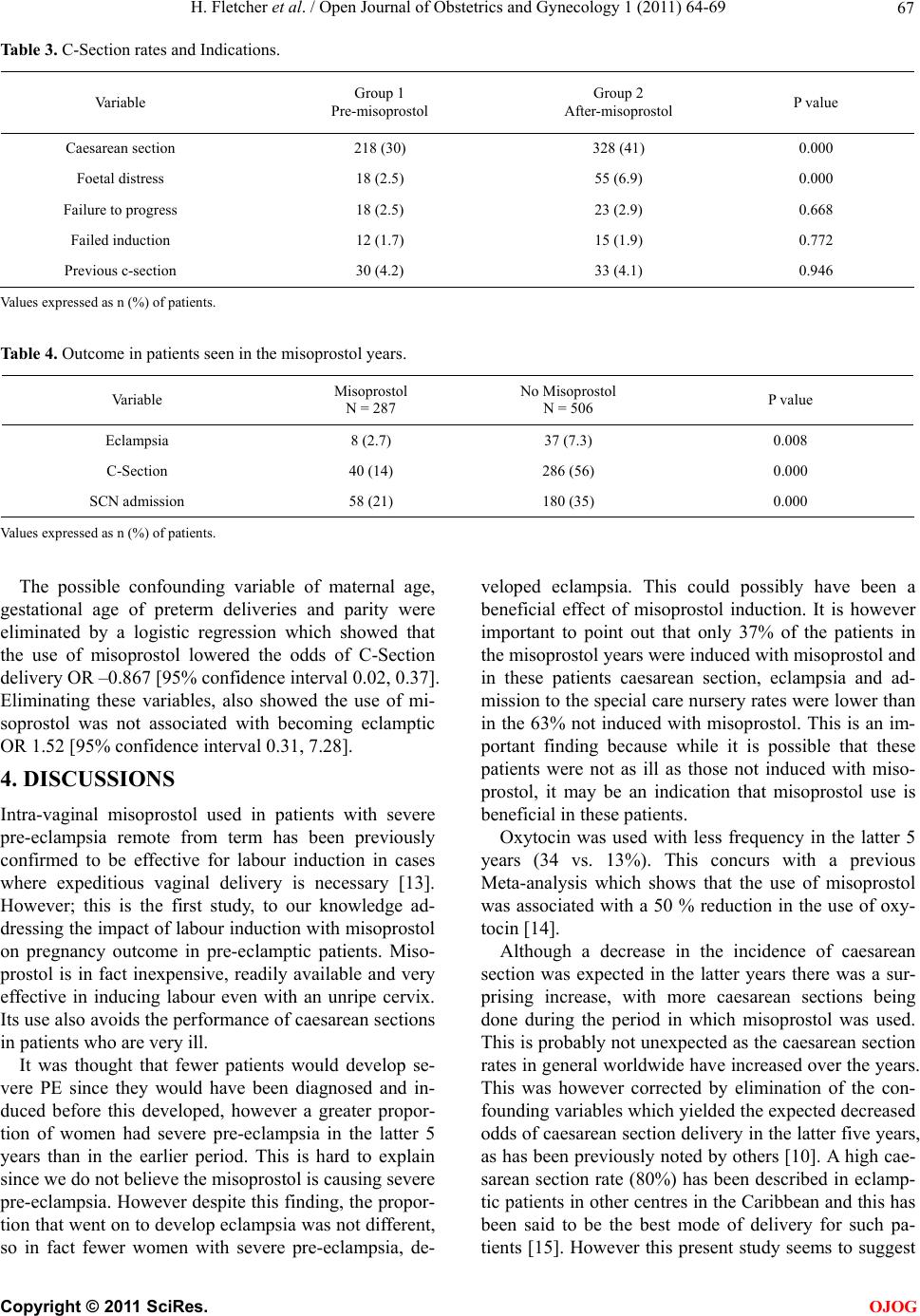
The fact that the gestational age at delivery and mean
neonatal birth weight were bo th lower after th e introd uc-
tion of misoprostol is also an important finding. What
this implies is that we now have the ability to intervene
earlier with induction of labour when severe pre-
eclampsia occurs. This could also be a reason for the
greater number of special care nursery admissions.
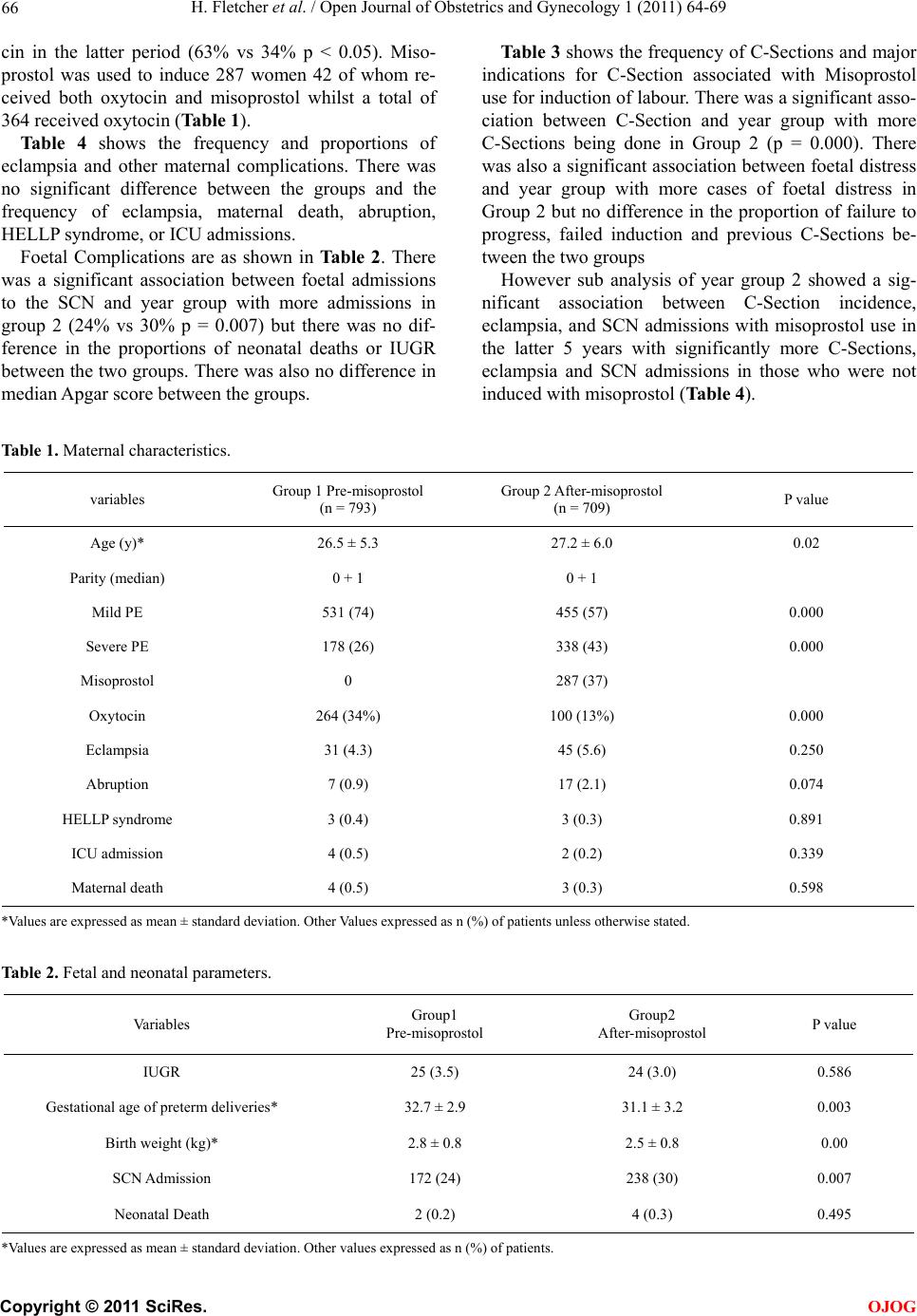
The overall frequency of eclampsia and other mater-
nal complicatio ns in the two groups were similar and no
improvement was seen in perinatal outcome. The fact
that more special care nursery admissions occurred in
the latter 5 years even though the mean Apgar scores
were similar may be an indication of differences in care
in the two eras. However misoprostol indu ction has been
shown to be associated with foetal distress (hyperstimu-
lation syndrome) and increased passage of meconium
especially at the high doses used at UWI [7,16] .
Pregnancy induced hypertension is the leading cause
of maternal mortality in Jamaica and timely delivery is
the only way to stop the progress of the cond ition. It was
therefore hoped that the introduction of misoprostol to
the obstetric armamentarium would have shown a dra-
matic difference in this outcome in these patients. This
however has not been the case as shown in this study
and also as has been demonstrated by the fact that de-
spite the introduction of misoprostol hypertensive disor-
ders still remain the leading cause of maternal mortality
[12,17] with no decrease in maternal mortality rates.
The main drawback to studies of this type is the im-
pact of differences in management which could have
occurred in the two different time periods which have
not been taken in to account. These may explain some of
the differences seen.
Using the data from one period alone has shown some
differences indicating that the introduction of misopros-
tol may have been beneficial in these patients although
the overall impact appears disappointing.
Thus, it can be concluded that the introduction of mi-
soprostol is beneficial to pregnancy out come in patients
with pre-eclampsia but has not shown significant im-
provements between the two eras, as there are other fac-
tors which may possibly be involved which need to be
identified and corrected. We therefore believe that the
introduction of misoprostol to decrease maternal com-
plication rates in these patients must be associated with
careful patient selection and close monitoring in labour.
REFERENCES
[1] Walker, G., McCaw-Binns, A., Ashley, D. and Bernard,
W. (1990) Identifying Maternal deaths in developing
countries: Experience in Jamaica. International Journal
of Epidemiology, 19, 599-605.
doi:10.1093/ije/19.3.599
[2] Keeling, J., McCaw-Binns, A., Ashley, D. and Golding, J.
(1991) Maternal mortality in Jamaica; Health care provi-
sions and causes of death. International Journal of Gy-
necology & Obstetrics, 35, 19-27.
doi:10.1016/0020-7292(91)90058-D
[3] Xiong, X., Mayes, D., Demianczuk, N., Olson, D.M.,
Davidge, S.T., Newburn-Cook, C., and Saunders, L.D.
(1999) Impact of pregnancy-induced hypertension on fe-
tal growth. American Journal of Obstetrics & Gyneco-
logy, 180, 207-213. doi:10.1016/S0002-9378(99)70176-6
[4] Cunningham, F.G. and Lindheimer, M.D. (1992) Hyper-
tension in pregnancy. The New England Journal of Medi-
cine, 326, 927-932.
doi:10.1056/NEJM199204023261405
[5] Campos, G.A., Guzman, S., Rodriguez, J.G., Voto, L.S.
and Margulies, M. (1994) Misoprostol--a PGE1 analog
for induction of labor at term: comparative and random-
ized study with oxytocin. Revista chilena de obstetricia y
ginecologia, 59, 190-195 (in Spanish).
[6] Chuck, F.J. and Huffaker, B.J. (1995) Labor induction
with intravaginal misoprostol versus intracervical pros-
taglandins E2 gel. randomised comparison. American
Journal of Obstetrics & Gynecology, 173, 1137-1142.
[7] Wing, D.A., Ortiz-Omphroy, G. and Paul, R.H. (1997) A
comparison of intermittent vaginal administration of mi-
soprostol with continuous dinoprostone for cervical rip-
ening and labor induction. American Journal of Obstet-
rics & Gynecology, 177, 612-618.
doi:10.1016/S0002-9378(97)70154-6
[8] Fletcher, H., Mitchell, S., Simeon, D., Brown, D. (1993)
Intravaginal misoprostol as a cervical ripening agent.
British Journal of Obstetrics & Gynecology, 100, 641-
644. d oi:10.1111/j.1471-0528.1993.tb14230.x
[9] Fletcher, H., Mitchell, S., Simeon, D. and Brown, D.
(1994) Intra-vaginal misoprostol versus dinoprostone as
cervical ripening and labor-inducing agents. Obstetrics &
Gynecology, 83, 244-247.
[10] Del Valle, G.O., Sanchez-Ramos, L., Jordan, C.W.,
Gaudier, F.L. and Delke, I. (1996) Use of misoprostol
(prostaglandin E1 methyl analogue) to expedite delivery
in severe pre-eclampsia remote from term. Journal of
maternal-fetal medicine, 5, 39-40.
doi:10.1002/(SICI)1520-6661(199601/02)5:1<39::AID-
MFM9>3.0.CO;2-U
[11] Fletcher, H. and Hutchinson, S. (2001) A retrospective
review of pregnancy outcome after misoprostol (pros-
taglandin E1) induction of labour. West Indian Medical
C
opyright © 2011 SciRes. OJOG