H. Takagi et al. / Open Journal of Obstetrics and Gynecology 1 (2011) 21-24 23
ymptomatic participants undergo a medical examination
at public expense. The cultural tradition and high con-
cern on check-up of our subjects restrict the likelihood
of multiple sexual partners. This may explain why very
low incidence of dysplastic changes and cervical cancer
were found in our study group of women.
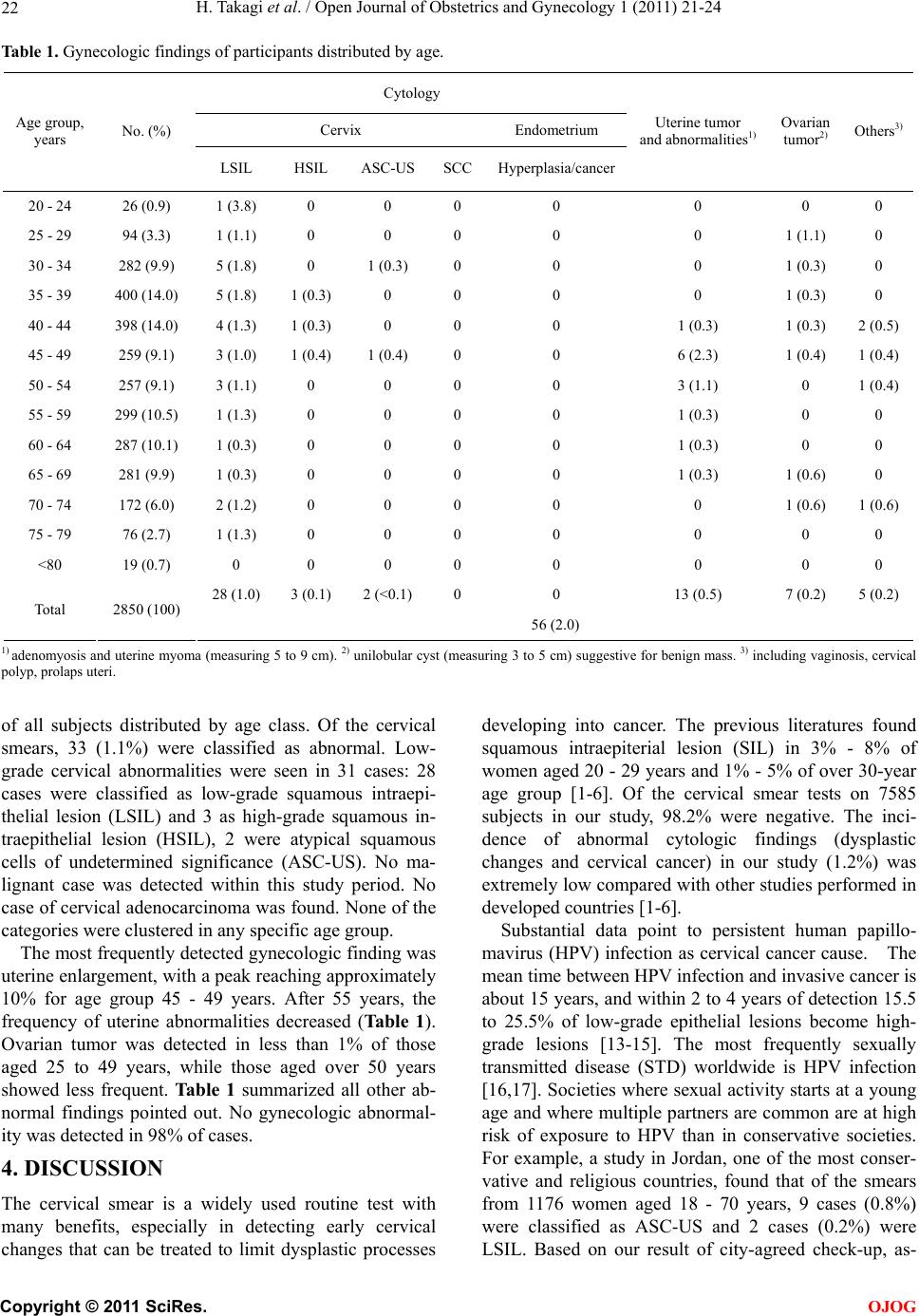
Of pelvic mass, uterine myomas and/or adenomyosis
are estimated to be present in 20% - 25% or reproduc-
tive-age women, indicating that they are one of the most
common human neoplasma [18-20]. A myoma does not
necessarily produce symptoms, and even very large ones
may go undetected by the patient, particularly if she is
obese. Symptoms from myomas depend on their location,
size and state of presentation; symptoms are present in
35% - 50% of patients with myomas. Ovarian tumors,
cystic or solid, are also frequently asymptomatic and
undetected by themselves. The diagnosis of these tumors
is not usually difficult using ultrasonography at physical
check-up. We observed lower frequency of uterine en-
largement and ovarian tumors in our subjects.
The present study based on symptom-free population
suggested annual gynecologic screening and proper fol-
low-up programs even against asymptomatic women
may remarkably reduce the probability of (pre) maliga-
nant disease. Since the study sample was shown to be
representative populatio n of high-attitu de toward screen-
ing but non-high income, most of our observations may
have important implications in terms of public health.
REFERENCES
[1] Anttila, A., Ronco, G., Clifford, G., Bray, F., Hakama, M.,
Arbyn, M. and Weiderpass, E. (2004) Cervical cancer
screening programmes and policies in 18 European
countries. British Journal of Cancer, 91, 935-941.
[2] Bray, F., Loos, A., McCarron, P., Weiderpass, E., Arbyn,
M., Møller, H., Hakama, M. and Parkin, D. (2005)
Trends in cervical squamous cell carcinoma incidence in
13 European countries: Changing risk and the effects of
screening. Cancer Epidemiology, Biomarkers & Preven-
tion, 14, 677-686. doi:10.1158/1055-9965.EPI-04-0569
[3] Greenlee, R., Hill-Harmon, M., Murray, T. and Thun, M.
(2001) Cancer statistics, 2001. CA: A Cancer Journal for
Clinicians, 51, 15-36. doi:10.3322/canjclin.51.1.15
[4] Hakama, M., Coleman, M., Alexe, D. and Auvinen, A.
(2008) Cancer screening: Evidence and practice in Eu-
rope 2008. European Journal of Cancer, 44, 1404-1413.
doi:10.1016/j.ejca.2008.02.013
[5] Johannesson, G., Geirsson, G., Day, N. and Tulinius, H.
(1982) Screening for cancer of the uterine cervix in Ice-
land 1965-1978. Acta Obstetricia et Gynecologica Scan-
dinavica, 61, 199-203.
doi:10.3109/00016348209156556
[6] Mount, S. and Papillo, J. (1999) A study of 10,296 pedi-
atric and adolescent Papanicolaou smear diagnoses in
northern New England. Pediatrics, 103, 539-545.
doi:10.1542/peds.103.3.539
[7] Nieminen, P., Kallio, M., Anttila, A. and Hakama, M.
(1999) Organised vs. spontaneous Pap-smear screening
for cervical cancer: A case-control study. International
Journal of Cancer, 83, 55-58.
doi:10.1002/(SICI)1097-0215(19990924)83:1<55::AID-I
JC11>3.0.CO;2-U
[8] Dietrich, A., Tobin, J., Cassells, A., Robinson, C., Greene,
M., Sox, C., Beach, M., DuHamel, K. and Younge, R.
(2006) Telephone care management to improve cancer
screening among low-income women: A randomized,
controlled trial. Annals of Internal Medicine, 144, 563-
571.
[9] Lawson, H., Henson, R., Bobo, J. and Kaeser, M. (2000)
Implementing recommendations for the early detection
of breast and cervical cancer among low-income women.
MMWR—Recommendations and Reports, 49, 37-55.
[10] Ng, E., Wilkins, R., Fung, M. and Berthelot, J. (2004)
Cervical cancer mortality by neighbourhood income in
urban Canada from 1971 to 1996. Canadian Medical
Association Journal, 170, 1545-1549.
doi:10.1503/cmaj.1031528
[11] Schoenberg, N., Hopenhayn, C., Christ ian, A., Kn igh t, E.
and Rubio, A. (2005) An in-depth and updated perspec-
tive on determinants of cervical cancer screening among
central Appal achian w omen. Women Health, 42, 89-105.
doi:10.1300/J013v42n02_06
[12] Yabroff, K., Lawrence, W., King, J., Mangan, P., Wash-
ington, K., Yi, B., Kerner, J. and Mandelblatt, J. (2005)
Geographic disparities in cervical cancer mortality: What
are the roles of risk factor prevalence, screening, and use
of recommended treatment? The Journal of Rural Health,
21, 149-157. doi:10.1111/j.1748-0361.2005.tb00075.x
[13] Muñoz, N., Bosch, F., de Sanjosé, S., Herrero, R., Cas-
tellsagué, X., Shah, K., Snijders, P. and Meijer, C. (2003)
Epidemiologic classification of human papillomavirus
types associated with cervical cancer. The New England
Journal of Medicine, 348, 518-527.
doi:10.1056/NEJMoa021641
[14] Rocha-Zavaleta, L., Yescas, G., Cruz. R. and Cruz-Talo-
nia, F. (2004) Human papillomavirus infection and cer-
vical ectopy. International Journal of Gynecology & Ob-
stetrics, 85, 259-266. doi:10.1016/j.ijgo.2003.10.002
[15] Tachezy, R., Saláková, M., Hamsíková, E., Kanka, J.,
Havránková, A. and Vonka, V. (2003) Prospective study
on cervical neoplasia: Presence of HPV DNA in cyto-
logical smears precedes the development of cervical neo-
plastic lesions. Sexually Transmitted Infections, 79, 191-
196. doi:10.1136/sti.79.3.191
[16] Baseman, J. and Koutsky, L. (2005) The epidemiology of
human papillomavirus infections. Journal of Clinical Vi-
rology, 32, S16-24. doi:10.1016/j.jcv.2004.12.008
[17] Clavel, C., Masure, M., Bory, J., Putaud, I., Mangeonjean,
C., Lorenzato, M., Nazeyrollas, P., Gabriel, R. and Que-
reux, C., Birembaut, P. (2001) Human papillomavirus
testing in primary screening for the detection of high-
grade cervical lesions: A study of 7932 women. British
Journal of Cancer, 84, 1616-1623.
doi:10.1054/bjoc.2001.1845
[18] Levy, B. (2008) Modern management of uterine fibroids.
Acta Obstetricia et Gynecologica Scandinavica, 87, 812-
823. doi:10.1080/00016340802146912
[19] Parker, W. (2007) Uterine myomas: Management. Fertil-
C
opyright © 2011 SciRes. OJOG