Open Journal of Obstetrics and Gynecology, 2011, 1, 13-16
doi:10.4236/ojog.2011.12003 Published Online June 2011 (http://www.SciRP.org/journal/ojog/
OJOG
).
Published Online June 2011 in SciRes. http://www.scirp.org/journal/OJOG
Isolated proteinuria as an initial sign of severe preeclampsia
Takahir o Ya mada, Takashi Ya mada, Mamoru Morikawa, Masamitsu Takeda, Ryutaro Nishida,
Rina Akaishi, Hisanori Minakami
Department of Obstetrics, Hokkaido University Graduate School of Medicine, Sapporo, Japan.
Email: taka0197@med.hokudai.ac.jp
Received 21 April 2011; revised 20 May 2011; accepted 27 May 2011.
ABSTRACT
Two pregnant women who initially developed pro-
teinuria alone followed by serious preeclampsia are
presented to emphasize that there is no adequate
technical term to express the period of proteinuria
alone based on the current criteria of pregnancy-
induced hypertension. Case 1 exhibited a urinary
protein concentration of 46 mg/dL in the absence of
hypertension, and abdominal pain due to placental
abruption with hypertension at gestational week
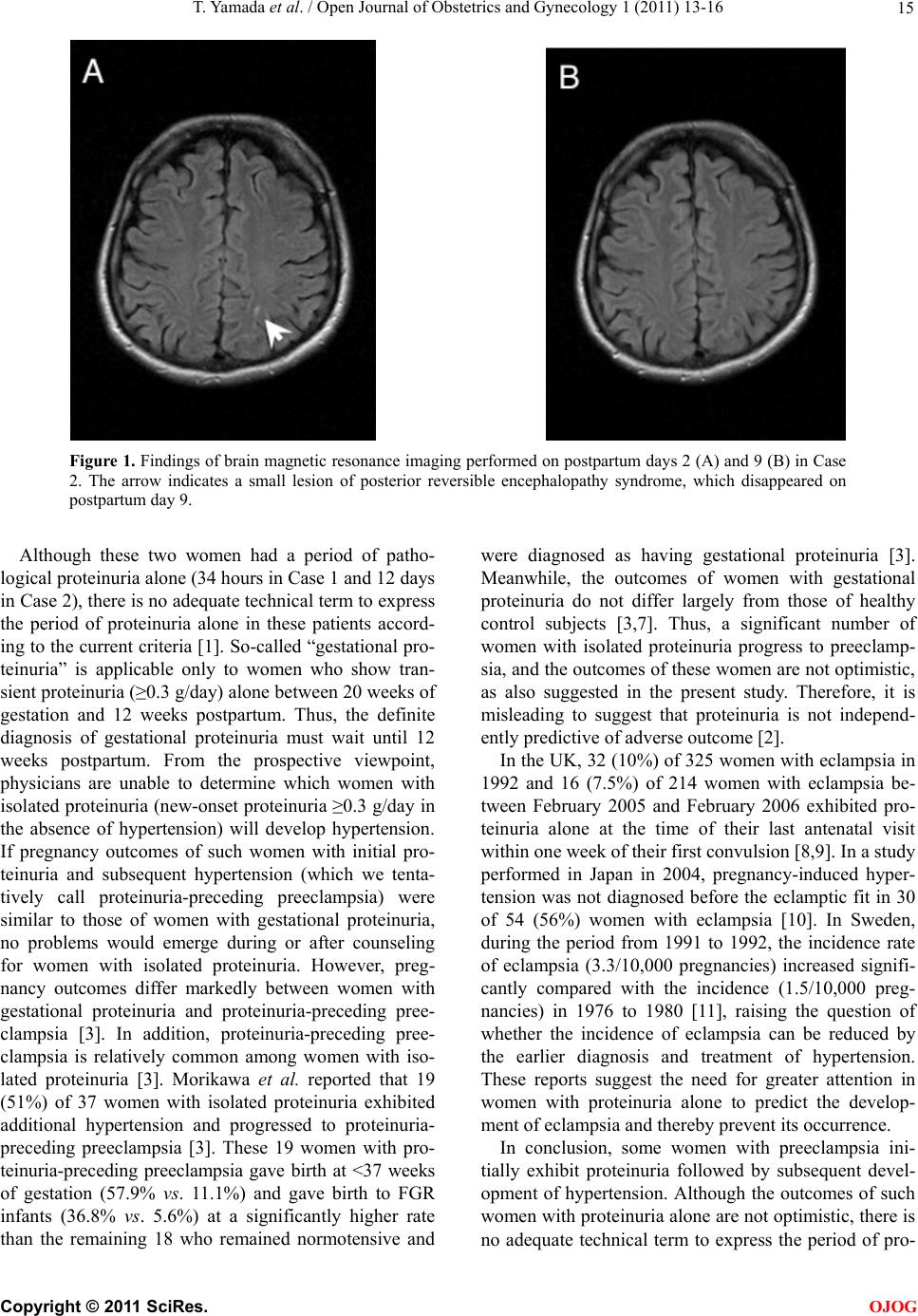
(GW) 29–3/7 and 29–4/7, respectively. Case 2 exhibited a
urinary protein/creatinine ratio of 2.67, developed
hypertension, required cesarean section, and devel-
oped posterior reversible encephalopathy syndrome
at GW 28–1/7, 29–6/7, and 32–0/7, and on postpartum
day 2, respectively. As women with proteinuria alone
are not diagnosed as having preeclampsia and as a
diagnosis of gestational proteinuria can be made only
at 12 weeks postpartum, a prospective technical term
applicable to the condition of proteinuria alone is
needed to increase physicians’ attention to this co ndi-
tion.
Keywords: Posterior Reversible Encephalopathy
Syndrome; Proteinuria; Placental Abruption;
Pregnancy-Induced Hypertension
1. INTRODUCTION
Based on the current criteria adopted in many countries,
women with proteinuria alone are not diagnosed as hav-
ing preeclampsia until they also exhibit hypertension [1];
in Japan, those who do not develop hypertension are
diagnosed as having had gestational proteinuria. Thus,
gestational proteinuria is a retrospective diagnosis. These
criteria may have been based on the belief that clinical
presentation of preeclampsia involves initial hyperten-
sion and subsequent proteinuria. However, whether
some pregnant women who initially exhibit proteinuria
subsequently develop hypertension had not been exten-
sively studied. The clinical outcomes of such women
with gestational proteinuria, defined as those exhibiting
transient proteinuria of ≥0.3 g/day appearing at or after
20 weeks of gestation and disappearing by 12 weeks
postpartum, had been believed to be favorable, and pro-
teinuria had been thought not to be an independent pre-
dictor of an adverse outcome [2].
However, a recent report indicated that approximately
50% of women who develop proteinuria ≥0.3 g/day at
and after 20 weeks of gestation in the absence of hyper-
tension progress to preeclampsia [3]. If this is the case, it
is misleading to suggest that the outcome of pregnancy
in patients with isolated proteinuria is favorable.
Here, we present two patients who showed proteinuria
initially and subsequently developed hypertension, and
finally experienced severe clinical conditions. We em-
phasize that physicians have no adequate technical term
to express the period of proteinuria alone in such pa-
tients according to the current criteria of pregnancy-in-
duced hypertension.
2. PATIENTS AND RESULTS
This study was approved by the institutional review
board of the Hokkaido University Hospital.
Case 1: A 43-year-old nulliparous woman showed
blood pressure (BP) of 124/75 mmHg and proteinuria (1
+ on dipstick) at a regular antenatal visit at gestational
week (GW) 28–3/7 in July 2008. She exhibited BP of
119/78 mmHg, urinary protein concentration of 46
mg/dL (Ta bl e 1 ), and weight gain of 1.7 kg in 1 week,
and was diagnosed as having fetal growth restriction
(FGR, estimated fetal body weight of 1082 g) the fol-
lowing week (GW 29–3/7). Blood chemistry revealed
anemia only. The patient requested treatment on an out-
patient basis despite our recommendation of hospitaliza-
tion. Thirty-four hours later, the patient presented with
abdominal pain, hypertension (BP of 176/98 mmHg),
and urinary protein concentration of 120 mg/dL. Placen-
tal abruption was suspected based on ultrasonography
findings and was confirmed by uneventful emergency
cesarean section. A female infant with Apgar scores of 3