A. E. LASHEEN ET AL.
Copyright © 2011 SciRes. SS
181
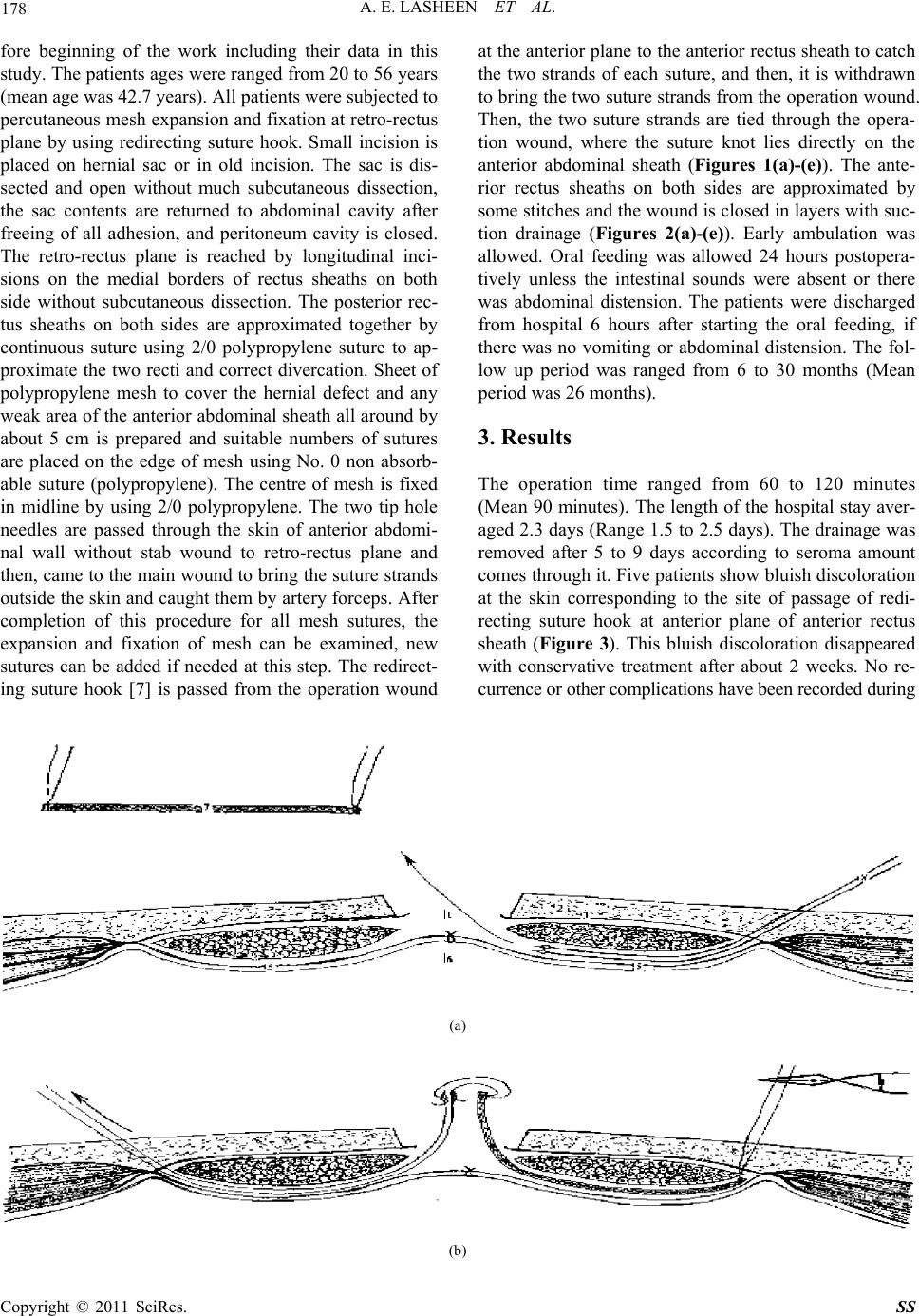
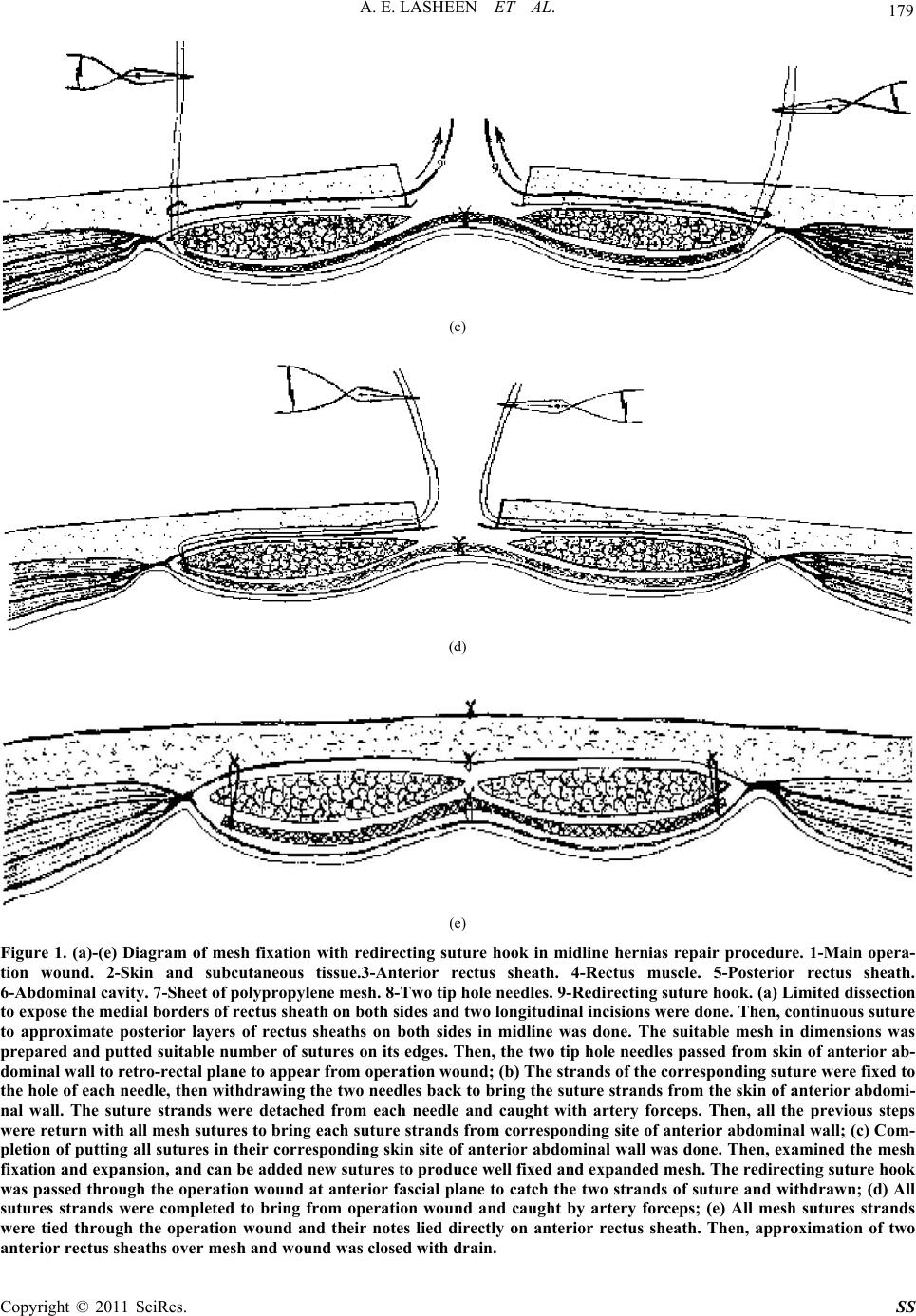
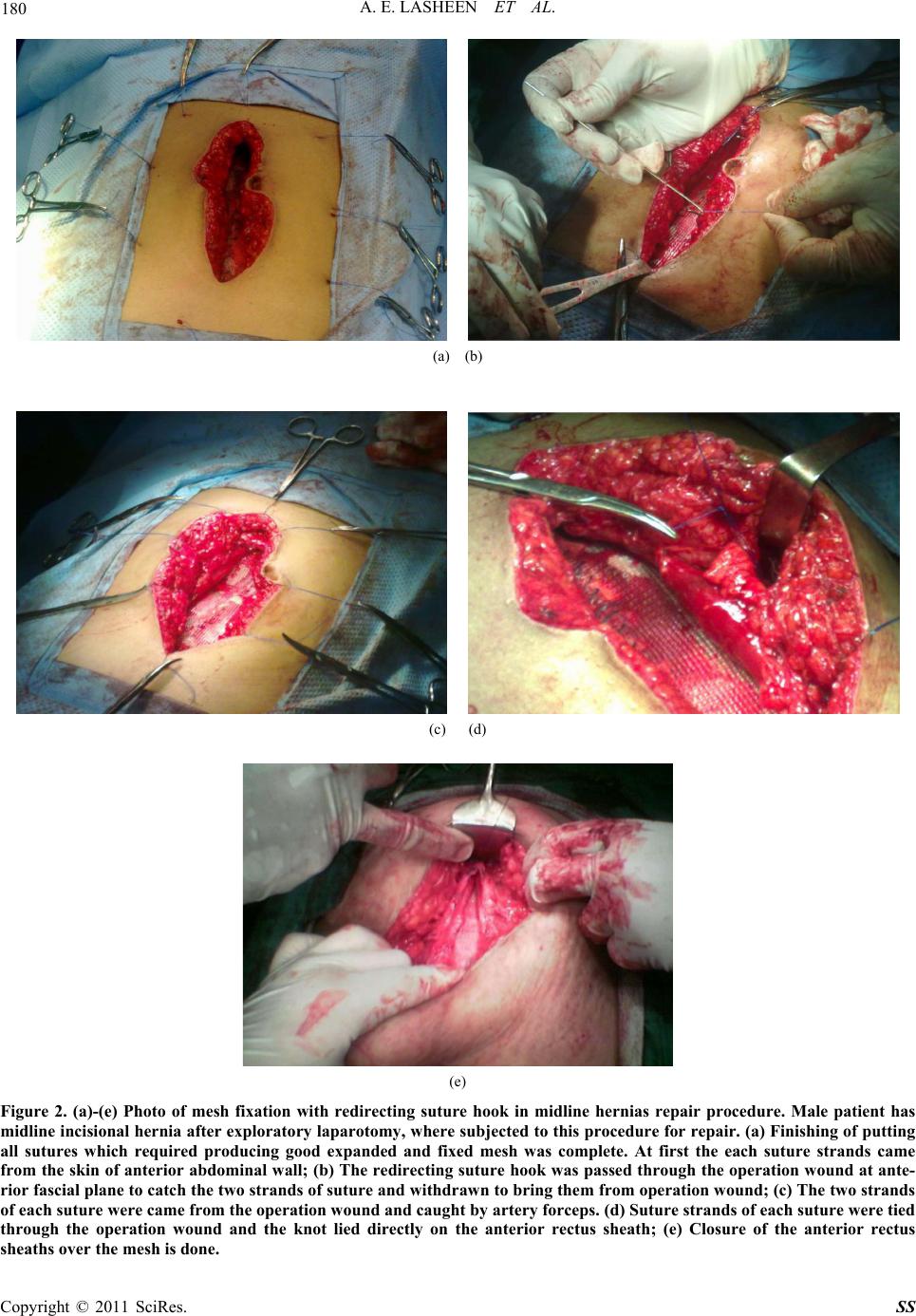
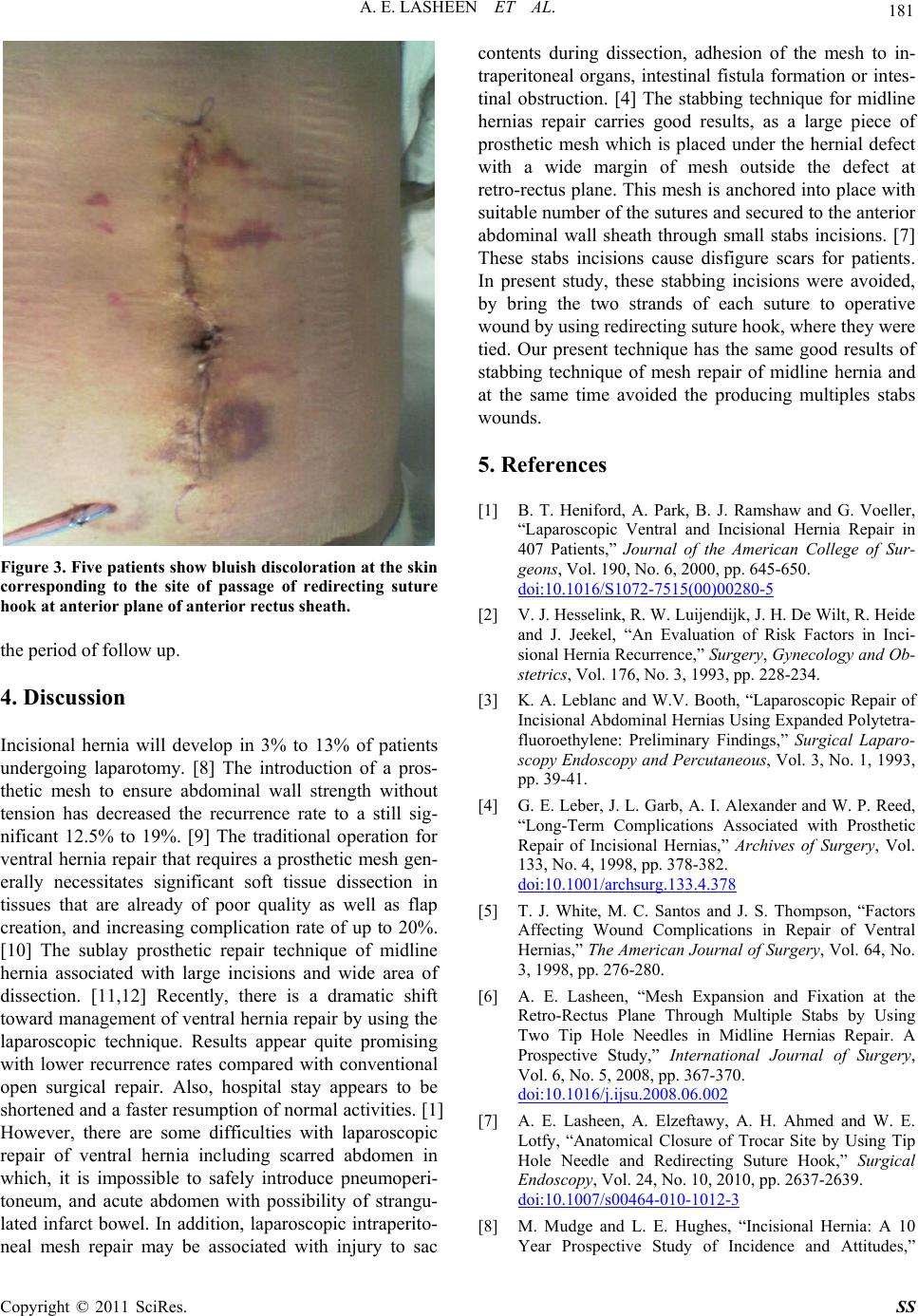
Figure 3. Five patients show bluish discoloration at the skin
corresponding to the site of passage of redirecting suture
hook at anterior plane of anterior rectus sheath.
the period of follow up.
4. Discussion
Incisional hernia will develop in 3% to 13% of patients
undergoing laparotomy. [8] The introduction of a pros-
thetic mesh to ensure abdominal wall strength without
tension has decreased the recurrence rate to a still sig-
nificant 12.5% to 19%. [9] The traditional operation for
ventral hernia repair that requires a prosthetic mesh gen-
erally necessitates significant soft tissue dissection in
tissues that are already of poor quality as well as flap
creation, and increasing complication rate of up to 20%.
[10] The sublay prosthetic repair technique of midline
hernia associated with large incisions and wide area of
dissection. [11,12] Recently, there is a dramatic shift
toward management of ventral hernia repair by using the
laparoscopic technique. Results appear quite promising
with lower recurrence rates compared with conventional
open surgical repair. Also, hospital stay appears to be
shortened and a faster resumption of normal activities. [1]
However, there are some difficulties with laparoscopic
repair of ventral hernia including scarred abdomen in
which, it is impossible to safely introduce pneumoperi-
toneum, and acute abdomen with possibility of strangu-
lated infarct bowel. In addition, laparoscopic intraperito-
neal mesh repair may be associated with injury to sac
contents during dissection, adhesion of the mesh to in-
traperitoneal organs, intestinal fistula formation or intes-
tinal obstruction. [4] The stabbing technique for midline
hernias repair carries good results, as a large piece of
prosthetic mesh which is placed under the hernial defect
with a wide margin of mesh outside the defect at
retro-rectus plane. This mesh is anchored into place with
suitable number of the sutures and secured to the anterior
abdominal wall sheath through small stabs incisions. [7]
These stabs incisions cause disfigure scars for patients.
In present study, these stabbing incisions were avoided,
by bring the two strands of each suture to operative
wound by using redirecting suture hook, where they were
tied. Our present technique has the same good results of
stabbing technique of mesh repair of midline hernia and
at the same time avoided the producing multiples stabs
wounds.
5. References
[1] B. T. Heniford, A. Park, B. J. Ramshaw and G. Voeller,
“Laparoscopic Ventral and Incisional Hernia Repair in
407 Patients,” Journal of the American College of Sur-
geons, Vol. 190, No. 6, 2000, pp. 645-650.
doi:10.1016/S1072-7515(00)00280-5
[2] V. J. Hesselink, R. W. Luijendijk, J. H. De Wilt, R. Heide
and J. Jeekel, “An Evaluation of Risk Factors in Inci-
sional Hernia Recurrence,” Surgery, Gynecology and Ob-
stetrics, Vol. 176, No. 3, 1993, pp. 228-234.
[3] K. A. Leblanc and W.V. Booth, “Laparoscopic Repair of
Incisional Abdominal Hernias Using Expanded Polytetra-
fluoroethylene: Preliminary Findings,” Surgical Laparo-
scopy Endoscopy and Percutaneous, Vol. 3, No. 1, 1993,
pp. 39-41.
[4] G. E. Leber, J. L. Garb, A. I. Alexander and W. P. Reed,
“Long-Term Complications Associated with Prosthetic
Repair of Incisional Hernias,” Archives of Surgery, Vol.
133, No. 4, 1998, pp. 378-382.
doi:10.1001/archsurg.133.4.378
[5] T. J. White, M. C. Santos and J. S. Thompson, “Factors
Affecting Wound Complications in Repair of Ventral
Hernias,” The American Journal of Surgery, Vol. 64, No.
3, 1998, pp. 276-280.
[6] A. E. Lasheen, “Mesh Expansion and Fixation at the
Retro-Rectus Plane Through Multiple Stabs by Using
Two Tip Hole Needles in Midline Hernias Repair. A
Prospective Study,” International Journal of Surgery,
Vol. 6, No. 5, 2008, pp. 367-370.
doi:10.1016/j.ijsu.2008.06.002
[7] A. E. Lasheen, A. Elzeftawy, A. H. Ahmed and W. E.
Lotfy, “Anatomical Closure of Trocar Site by Using Tip
Hole Needle and Redirecting Suture Hook,” Surgical
Endoscopy, Vol. 24, No. 10, 2010, pp. 2637-2639.
doi:10.1007/s00464-010-1012-3
[8] M. Mudge and L. E. Hughes, “Incisional Hernia: A 10
Year Prospective Study of Incidence and Attitudes,”