Surgical Science, 2011, 2, 175-176
doi:10.4236/ss.2011.24038 Published Online June 2011 (http://www.SciRP.org/journal/ss)
Copyright © 2011 SciRes. SS
Ventricular Septal Defect and Left Ventricular Aneurysm
after Acute Myocardial Infarction
Kasra Azarnoush, Mario Manca, Andrea Innorta, Lionel Camilleri
CHU Clermont-Ferrand, Service de Chirurgie Cardiaque, Clermont-Ferrand, France
E-mail: kazarnoush@chu-clermontferrand.fr
Received January 14, 2011; revised April 27, 2011; accepted April 29, 2011
Abstract
The combination of an acute ventricular septal defect (VSD) and left ventricular aneurysm (LVA) is a rare,
life-threatening complication which usually occurs within the first week following acute myocardial infarct-
tion (AMI). We describe the case of an apical VSD and LVA in a 77-year-old diabetic and dyslipidemic
male patient after anterior AMI. The patient was an active smoker and had a history of chronic obstructive
pulmonary disease, arterial hypertension and atrial fibrillation. The patient underwent ventriculotomy for
VSD repair using a large equine pericardial patch followed by intraventricular patch remodelling of the LVA.
He was discharged 2 months after surgery and underwent a successful hip replacement 10 months later.
Keywords: Endoventricular Patch Remodelling, Myocardial Infarction, Ventricular Aneurysm, Ventricular
Septal Defect
1. Introduction
Acute ventricular septal defects (VSDs) usually occur
within the first week of acute myocardial infarction
(AMI) [1]. These defects have an incidence of 1% - 3%
[2] and are associated with high mortality if not diag-
nosed early and adequately managed [3].
Left ventricular aneurysms (LVAs) are more common,
with a reported incidence of 3.5% - 5% [4]. However, the
true incidence of LVAs is unknown because there is no
well-established definition of LVA and because of
time-dependant left ventricular remodelling with late
LVA occurrence [5]. LVAs have been associated with
myocardial free wall rupture, congestive heart failure,
left ventricular thrombus formation and ventricular tach-
yarrhythmias [3]. Acute VSD combined with LVA is
uncommon and usually occurs within the first week of
AMI.
2. Case Report
A 77-year-old diabetic and dyslipidemic male patient
suffered an anterior AMI. The patient was an active
smoker with a history of chronic obstructive pulmonary
disease, arterial hypertension and atrial fibrillation.
On day 1 he was referred to our hospital with symp-
toms of acute heart failure and renal dysfunction
(creatinine clearance 30 ml/min; estimated with the
Cockroft & Gault equation). Doppler-echocardiography
revealed an apical VSD, without valve disease, plus an
antero-apical LVA; the patient had an ejection fraction of
50% and pulmonary arterial systolic pressure of 70 mmHg.
Coronarography revealed occlusion of the anterior in-
terventricular artery and right coronary artery stenosis.
Preoperative Euroscore (standard Euroscore = 20, lo-
gistic Euroscore = 86.46%) graded the patient as high
risk.
The patient underwent surgery using typical bicaval
cannulation for the cardiopulmonary bypass circuit,
maintaining a blood temperature of 37˚C with warm
blood cardioplegia.
The antero-apical LVA was visible when the pericar-
dium was opened. Revascularization was performed with
a saphenous graft to the right coronary artery and a
skeletonized and pedicled left internal thoracic artery
graft to the interventricular artery.
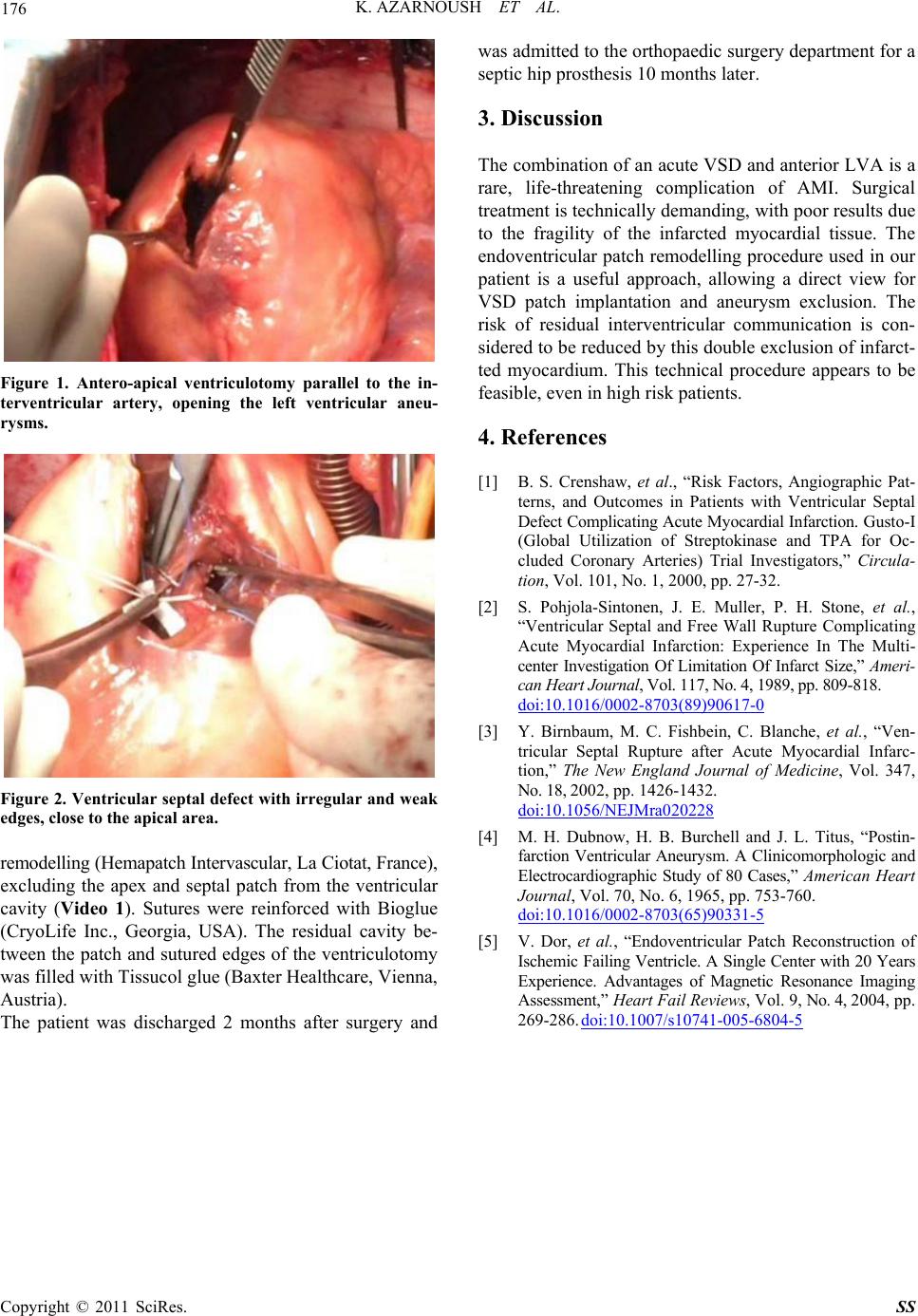
A 6 cm long left ventriculotomy was performed paral-
lel to the interventricular artery (Figure 1) for VSD re-
pair. The VSD had a diameter of 1.5 cm with irregular
and weak edges (Figure 2). The VSD was covered with
a large equine pericardial patch fastened with U stitches
and the fragile apical portion of the septum was rein-
forced with Bioglue (CryoLife Inc., Georgia, USA).
The LVA was then repaired by intraventricular patch