H. B. WANG ET AL.
Copyright © 2011 SciRes. SS
165
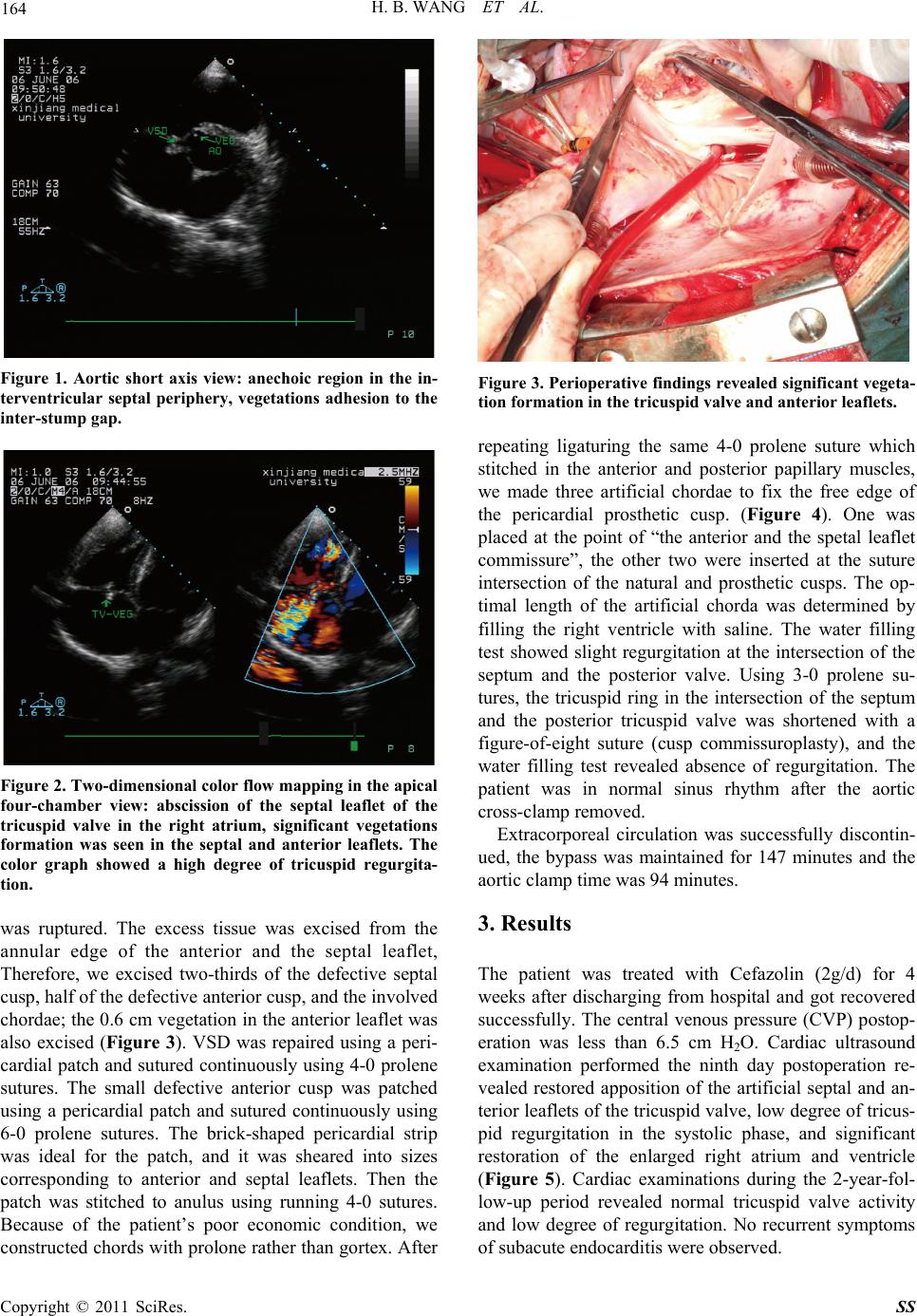
Figure 4. Operative procedures: (A) two large and one
small vegetations were presented at the anterior and septal
leaflets of the tricuspid valve, (B) two-thirds of the septal
cusp and half of the anterior cusp were excised, (C) peri-
cardial patch was used to replace the defected leaflets, arti-
fical chordae tendineae and Cusp commissuroplasty were
used to reconstruct the tricuspid valve.
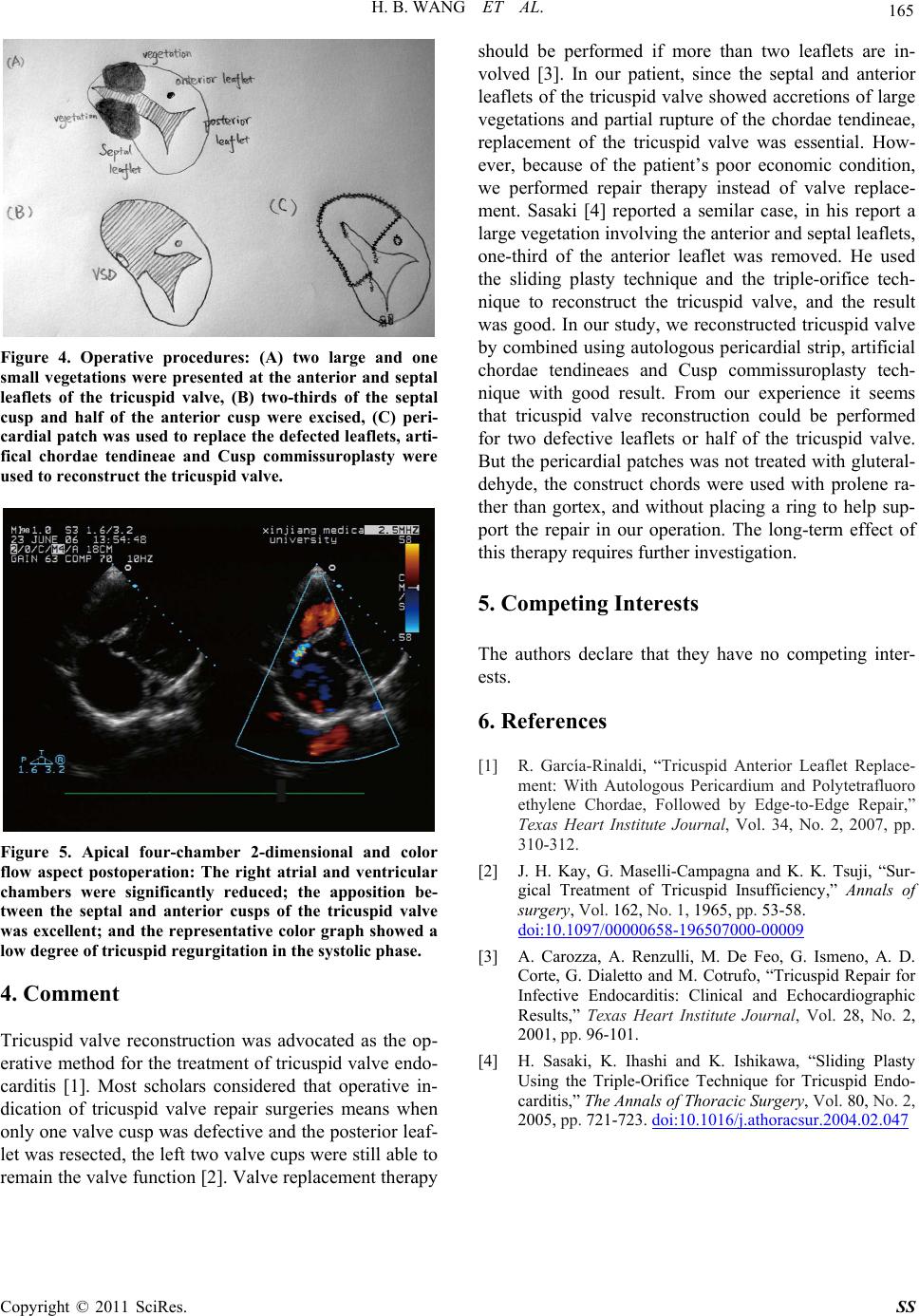
Figure 5. Apical four-chamber 2-dimensional and color
flow aspect postoperation: The right atrial and ventricular
chambers were significantly reduced; the apposition be-
tween the septal and anterior cusps of the tricuspid valve
was excellent; and the representative color graph showed a
low degree of tricuspid re g ur gi tation in the systolic phase.
4. Comment
Tricuspid valve reconstruction was advocated as the op-
erative method for the treatment of tricuspid valve endo-
carditis [1]. Most scholars considered that operative in-
dication of tricuspid valve repair surgeries means when
only one valve cusp was defective and the posterior leaf-
let was resected, the left two valve cups were still able to
remain the valve function [2]. Valve replacement therapy
should be performed if more than two leaflets are in-
volved [3]. In our patient, since the septal and anterior
leaflets of the tricuspid valve showed accretions of large
vegetations and partial rupture of the chordae tendineae,
replacement of the tricuspid valve was essential. How-
ever, because of the patient’s poor economic condition,
we performed repair therapy instead of valve replace-
ment. Sasaki [4] reported a semilar case, in his report a
large vegetation involv ing the an terior and septal leaflets,
one-third of the anterior leaflet was removed. He used
the sliding plasty technique and the triple-orifice tech-
nique to reconstruct the tricuspid valve, and the result
was good. In our study, we reconstruc ted tricuspid valve
by combined using autologous pericardial strip, artificial
chordae tendineaes and Cusp commissuroplasty tech-
nique with good result. From our experience it seems
that tricuspid valve reconstruction could be performed
for two defective leaflets or half of the tricuspid valve.
But the pericardial patch es was not treated with gluteral-
dehyde, the construct chords were used with prolene ra-
ther than gortex, and without placing a ring to help sup-
port the repair in our operation. The long-term effect of
this therapy requires further investigation.
5. Competing Interests
The authors declare that they have no competing inter-
ests.
6. References
[1] R. García-Rinaldi, “Tricuspid Anterior Leaflet Replace-
ment: With Autologous Pericardium and Polytetrafluoro
ethylene Chordae, Followed by Edge-to-Edge Repair,”
Texas Heart Institute Journal, Vol. 34, No. 2, 2007, pp.
310-312.
[2] J. H. Kay, G. Maselli-Campagna and K. K. Tsuji, “Sur-
gical Treatment of Tricuspid Insufficiency,” Annals of
surgery, Vol. 162, No. 1, 1965, pp. 53-58.
doi:10.1097/00000658-196507000-00009
[3] A. Carozza, A. Renzulli, M. De Feo, G. Ismeno, A. D.
Corte, G. Dialetto and M. Cotrufo, “Tricuspid Repair for
Infective Endocarditis: Clinical and Echocardiographic
Results,” Texas Heart Institute Journal, Vol. 28, No. 2,
2001, pp. 96-101.
[4] H. Sasaki, K. Ihashi and K. Ishikawa, “Sliding Plasty
Using the Triple-Orifice Technique for Tricuspid Endo-
carditis,” The Annals of Thoracic Surgery, Vol. 80, No. 2,
2005, pp. 721-723. doi:10.1016/j.athoracsur.2004.02.047