A. Milionis et al. / Health 3 (2011) 338-342
Copyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/
341341
represents a significant factor which leads to the forma-
tion of atherosclerotic lesions and favors both the desta-
bilization of the atheromatic plaque and the formation of
thrombi [25]. It is assumed that various factors could
differentiate selectively the sensitivity of the vascular
endothelium or affect in various ways the organism’s
reaction to the “toxic” influence of LDL.
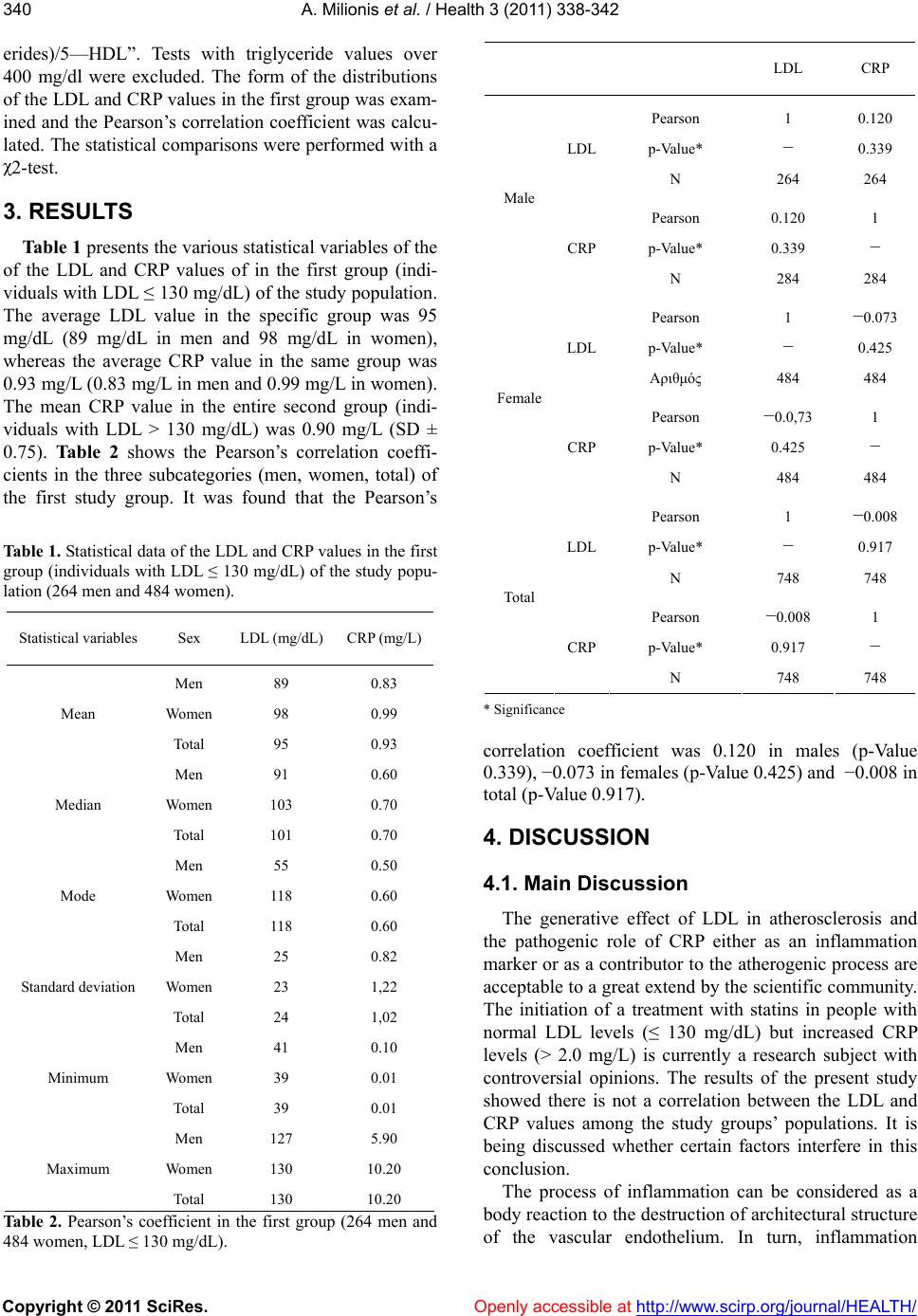
According to the Pearson’s correlation coefficient
(0.120 in males, −0.073 in females and −0.008 in total),
the LDL variations were not being followed by respec-
tive variations in the CRP values among the normal LDL
group in the present study. That is to say that an LDL
increase was not accompanied by a statistically respec-
tive CRP increase. Moreover, the comparison of the
mean values of CRP in the two study groups (individuals
with LDL ≤ 130 mg/dL and individuals with LDL > 130
mg/dL) showed that there is no statistically significant
difference (P > 0.05).
4.2. Conclusions
Nowadays, there is a clinical trend which supports the
study and use of certain biochemical markers, such as
oxidized phospholipids on apolipoprotein B-100 parti-
cles (OxPL/apoB), for the prediction of the development
of the atheromatic disease [26]. The findings of the pre-
sent study could also implicate a clinical significance.
They do not reject the initiation of a treatment with stat-
ins in individuals with a normal lipidemic profile but
increased CRP values (>2 mg/L), no matter what discus-
sion is being conducted on this field. However, the spe-
cific treatment should not be based exclusively on the
correlation of the LDL and CRP values, as certain re-
searchers believe, but it should include other criteria too.
Definitely, the coexisting increased levels of LDL and
CRP constitute a dangerous compound, even if the CRP
measurement has not been established as an important
marker for the prevention of cardiovascular incidents
and it is not included in the ordinary tests, unlike the
LDL evaluation. Further studies on this field are cer-
tainly necessary for the formation of well established
guidelines and the broad application of CRP screening
and the initiation of statin therapy or even treatment with
ezetimibe [27] in individuals with normal lipidemic pro-
file.
REFERENCES
[1] Everett, B.M., Glynn, R.J., MacFadyen, J.G. and Ridker,
P.M. (2010) Rosuvastatin in the prevention of stroke
among men and women with elevated levels of
C-reactive protein: justification for the use of statins in
prevention: an intervention trial evaluating rosuvastatin
(JUPITER). Circulation, 121, 143-150.
doi:10.1161/CIRCULATIONAHA.109.874834
[2] Fan, J. and Watanabe, T. (2003) Inflammatory reactions
in the pathogenesis of atherosclerosis. Journal of
Atherosclerosis and Thrombosis, 10, 63-71.
[3] Stoll, G. and Bendszus, M. (2006) Inflammation and
atherosclerosis—novel insights into plaque formation
and destabilization. Stroke, 37, 1923-1932.
doi:10.1161/01.STR.0000226901.34927.10
[4] Mora, S. and Ridker, P.M. (2006) Justification for the use
of statins in primary prevention: an intervention trial
evaluating rosuvastatin (JUPITER)—can C-reactive pro-
tein be used to target statin therapy in primary prevention?
The American Journal of Cardiology, 97, 33A-41A.
doi:10.1016/j.amjcard.2005.11.014
[5] Hirschfield, G.M. and Pepys, M.B. (2003) C-reactive
protein and cardiovascular disease: new insights from an
old molecule. QJM: Monthly Journal of the Association
of the Physicians, 96, 793-807.
[6] Venugopal, S.K., Devaraj, S. and Jialal, I. (2005) Effect
of C-reactive protein on vascular cells: evidence for a
proinflammatory, proatherogenic role. Current Opinion
in Nephrology and Hypertension, 14, 33-37.
doi:10.1097/00041552-200501000-00006
[7] Black, S., Kushner, I. and Samols, D. (2004) C-reactive
protein. The Journal of Biological Chemistry, 279,
48487-48490.
doi:10.1074/jbc.R400025200
[8] Pearson, T.A., Mensah, G.A., Alexander, R.W., Anderson,
J.L., Cannon, R.O. 3rd, Criqui, M., Fadl, Y.Y., Fortmann,
S.P., Hong, Y., Myers, G.L., Rifai, N., Smith, S.C. Jr,
Taubert, K., Tracy, R.P. and Vinicor, F. (2003) Markers of
inflammation and cardiovascular disease: Application to
clinical and public health practice: A statement for
healthcare professionals from the Centers for Disease
Control and Prevention and the American Heart Associa-
tion. Circulation, 107, 499-511.
doi:10.1161/01.CIR.0000052939.59093.45
[9] Devaraj, S., Singh, U. and Jialal, I. (2009) The evolving
role of C-reactive protein in atherothrombosis. Clinical
Chemistry, 55, 229-238.
doi:10.1373/clinchem.2008.108886
[10] Jialal, I., Devaraj, S. and Venugopal, S.K. (2004)
C-reactive protein: Risk marker or mediator in
atherothrombosis? Hypertension, 44, 6-11.
doi:10.1161/01.HYP.0000130484.20501.df
[11] Ridker, P.M. (2003) Clinical application of C-reactive
protein for cardiovascular disease detection and preven-
tion. Circulation, 107, 363-369.
doi:10.1161/01.CIR.0000053730.47739.3C
[12] Grundy, S.M., Cleeman, J.L., Merz, C.N., Brewer, H.B.
Jr, Clark, L.T., Hunninghake, D.B., Pasternak, R.C.,
Smith, S.C. Jr and Stone, N.J. (2004) Implications of re-
cent clinical trials for the National Cholesterol Education
Program Adult Treatment Panel III Guidelines. Circula-
tion, 110, 227-239.
doi:10.1161/01.CIR.0000133317.49796.0E
[13] Genest, J., McPherson, R., Frohlich, J., Anderson, T.,
Campbell, N., Carpentier, A., Couture, P., Dufour, R.,
Fodor, G., Francis, G.A., Grover, S., Gupta, M., Hegele,
R.A., Lau, D.C., Leiter, L., Lewis, G.F., Lonn, E.,
Mancini, G.B., Ng, D., Pearson, G.J., Sniderman, A.,
Stone, J.A. and Ur, E. (2009) 2009 Canadian Cardiovas-
cular Society/Canadian guidelines for the diagnosis and