A. ZEGHB IB ET AL.
Copyright © 2013 SciRes. ENG
a ‘virtual Star Chamber’ pooling all available expertise
of the clinical staff in that Unit; 2) use this wealth of
knowledge to derive current treatment for an individual
patient via data bases which can ideally be interrogated;
3) use data-mining tools to categorize the current patient
condition; 4) integrate current treatment protocols into
real-time care; 5) exploit a predictive function to model
and thus pred ict the clinical c ourse of the patien t into the
future resulting from this care; 6) Test, “off -line”, the
consequences of the current treatment actions; 7) Finally,
interrogate the generated data from the patient to check
conformity with the predicted outcome
In the Intensive Care environment, clinical decisions
are made to maintain patients’ physiological parameters
within acceptable (safe) ranges whilst treating or improv-
ing the underlying illne ss. Clinicians rely on their kno w-
ledge and experience to plan appropriate therapy rules.
These are applied to the developing clinical condition
and the outcomes revisited and alterations considered for
implementatio n.
Selecting the most appropriate treatment package from
differing options raises the possibility of potentially di-
verging and conflicting clinical decisions, or therapy
rules, and that selecting one path will engender a devel-
oping and necessarily diverging clinical course for that
patient. T his dilemma requires that t he choices should b e
clearly identified and that any model-based method must
be able to predict future consequences for each choice.
However, clinical decisions entail a degree of uncertainty
and do not have a clearly mapped outcome for the con-
sequences. If a clinician has a patient with a diagnosis
“D”, the therapeutic choices can be T1, T2, or T3. Ther-
apy “T1” may induce a complication and cause the pa-
tient to deteriorate. Therapeutic decision “T2” may im-
prove the state of t he patient, or may not chan ge it. “T3”
may treat t he diagno sis D, but entail colla teral da mage in
other organs. Thus the clinician faces considerable un-
certainty. A map detailing clear future outcomes in all
possibilities for patients’ anticipated clinical recovery
paths will be useful undoubtedly.
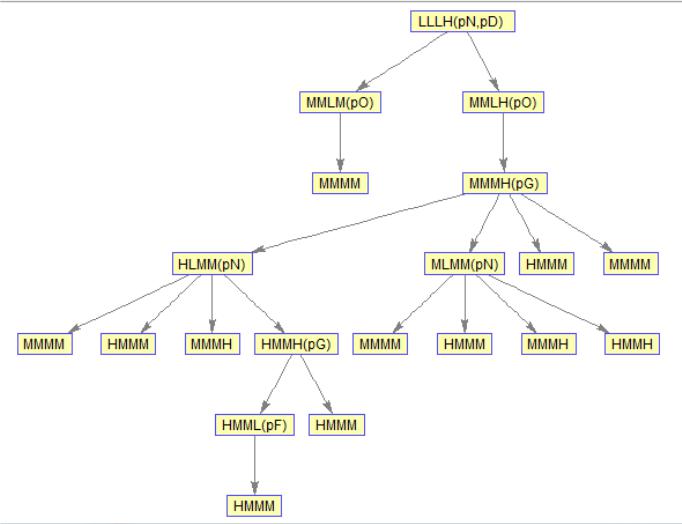
The decision-support map would provide clinicians
predicted pathways for multiple possible patient- states,
until the patient enters a final state of stability with nor-
malized values for all monitored physiological parame-
ters. This stable state would in effect represent, in terms
of dynamic systems, the so called equilibrium state.
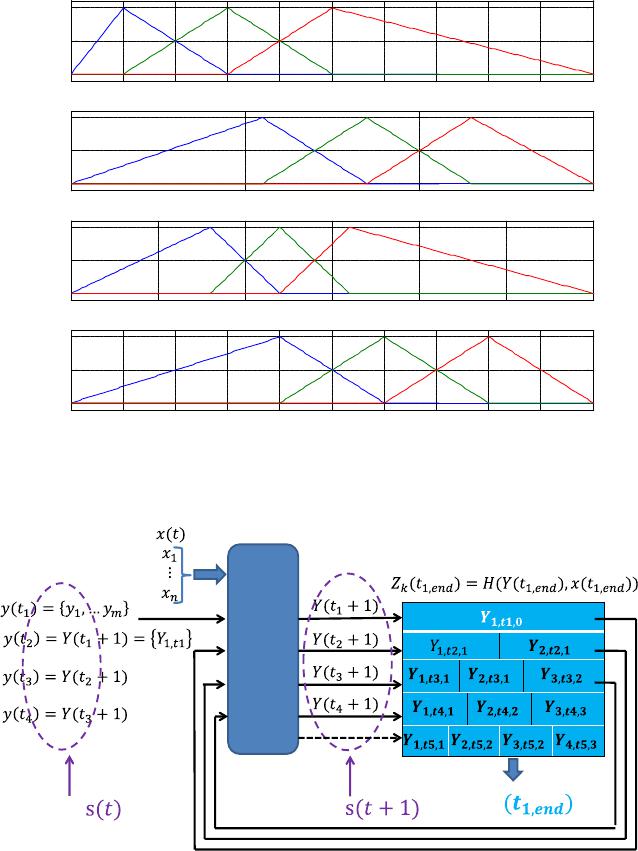
In the framework proposed in this paper, each gener-
ated node of the path displays two types of information.
The first describes the current values of physiological
parameters as concept variables, and the second de-
scribes the drug that causes these concept variables to
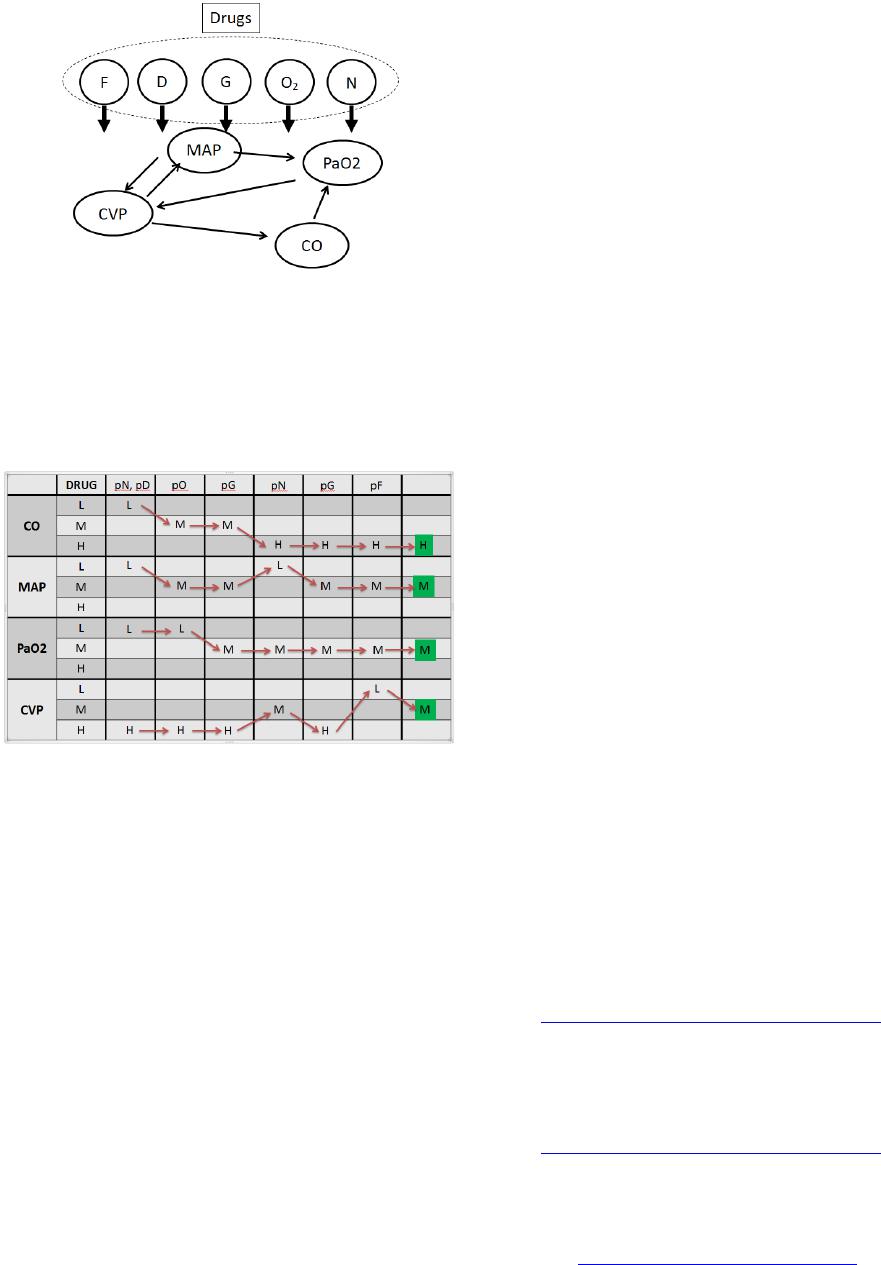
evolve according a certain trend. The physiological pa-
rameters are calculated by reflecting the connective inte-
ractions of the variables within each node and between
the nodes, which thus functions as part of a dynamical
biological system. Thus, the interaction between clinical
concepts should keep a stable equilibrium within time or
continuous until reach the equilibrium cycle, depending
on the initial patient state and the expert knowledge da-
ta-base.
The displayed options of possible treatment pathways
support a clinical proactive decision making. This model
has two principle components: the first component is the
State Transition Predictor (STP), and the second is the
Patient Paths Network (PPN). The first component is an
expert knowledge data-base of the basic clinical rules for
different possible patient states based on a number of
clinical concepts to be observed. The number of clinical
concepts is determined by a possibility that a clinical
outcome would in effect take place. The remainder of
this paper will be organized as follows: Section 2 will
detail the “recursive” concept as well as the associated
algorithms of the physiological patient map. Section 3
will explain how the cause-effect relationship within pa-
tient physiological parameters can be represented via a
fuzzy cognitive map. Finally, conclusions relating to the
proposed study together with future research directions
will be given in Se ction 4.
2. Physiological Patient Map
In order to populate the physiological patient map, we
reconceptualise clinical conditions from general terms
such a s “critical”, “stable” “mild”, etc.; via fuz z y l i ng ui s-
tic terms describing the values of the physiological pa-
rameters. Each parameter is described in one of three
fuzzy linguistic terms: Low (L), Medium (M), and High
(H). For m clinical concepts (i.e. physiological parame-
ters), the nodes (i.e. states) of p atient paths are expressed
as follows:
Let us consider a vector of m variables:
(1)
( )
{ }
, 1,Fuzzy Linguistic Terms
,,,:state index
kim
y
LMHk
=
∈
We argue here that there are two components (Mod-
ules) of our Physiological patient map: state transition
predictor (STP) and patient path network (PPN), see
“Figure 1”. The next sections will expand on these two
modules:
2.1. State Transition Predictor (STP)
The STP has two inputs, the first input is represented by
clinical concepts,
, and the second input is repre-
sented by drugs, i.e.
( )
{ }
,1 ,
,,:drug vector dimension
kk kn
xt xx n=
(2)