B. Liu et al. / Open Journal of Preventive Medicine 1 (2011) 8-12
ogically confirmed breast cancer between January 2000
and February 2001, were identified through three hospi-
tals, including Tongji Hospital, Xiehe Hospital and Wu-
han Central Hospital in Wuhan city of China. These
hospitals were requested to provide complete informa-
tion for all known cases of female breast cancer. All pa-
tients who entered the study in May 2003 have been
received follow-up visit till June, 2008. All of documents
included 163 completed data cases and 41 censored
cases, which had 25 visit loss cases, 1 death of other
diseases case and 15 survival cases.
2.2. Data Collection
On the basis of all sources of information, we recon-
structed a detailed medical history for each patient. In
compiling all sources of information, we also ascertained
breast cancer stage, histology, estrogen receptor (ER)
status, methods of treatment, age at diagnosis, gestagenic
history, and married status [12] through their abstraction
of pathology reports and medical records relating to
breast cancer diagnosis. For women who had two or
more primary cancers diagnosed within the follow-up
time, we took the earliest diagnosis, or if both tumors
were diagnosed on the same date, the tumor characteris-
tics are those associated with the larger tumor.
Although we were able to confirm most exposure his-
tories of patients through interview of medical records,
we were unable to confirm other information. Thus, the
exposure information, such as educational level, occupa-
tion, emotional function, social function and economical
status correlated with health, were obtained by trained
interviewers that asked patients, their husband or first-
degree relatives. All data were collected with a stan-
dardized questionnaire using a telephone interview.
Variables included demographics, emotional function,
social function and economical status. If patients die,
interviewers must obtain their age at death. Due to the
nature of the data collected (medical records and tele-
phone interview), complete information was impossible
for some of the variable assessed. In some instances (e.g.
the history of other chronic disease, emotional function,
social function and economical status) over 35% of the
data were missing, therefore these variables were ex-
cluded from the analysis. In the end, complete informa-
tion was available for 204 cases from the initial study
population of 300 cases.
2.3. Statistical Methods
Twenty-one features of patients, clinical pathologic fac-
tors and lifestyle have been selected as the indexes of
analysis and been quantified, which came from clinical
records and may influence prognosis of patients with
breast cancer. Patients’ live time were calculated by
month, which means the time span from the operation
day to death or termination of follow-up visit, and we
put corresponding data of every patient into computer on
the basis of clinical records and results of follow-up visit,
and data was dealt by SAS9.0 for WINDOWS software
and the survival rate was calculated by life table method.
All indexes of survival rate difference were analyzed by
multiple factor Cox proportional hazard model (using
gradually backward progressive method, two-tailed α =
0.05).
3. RESULTS
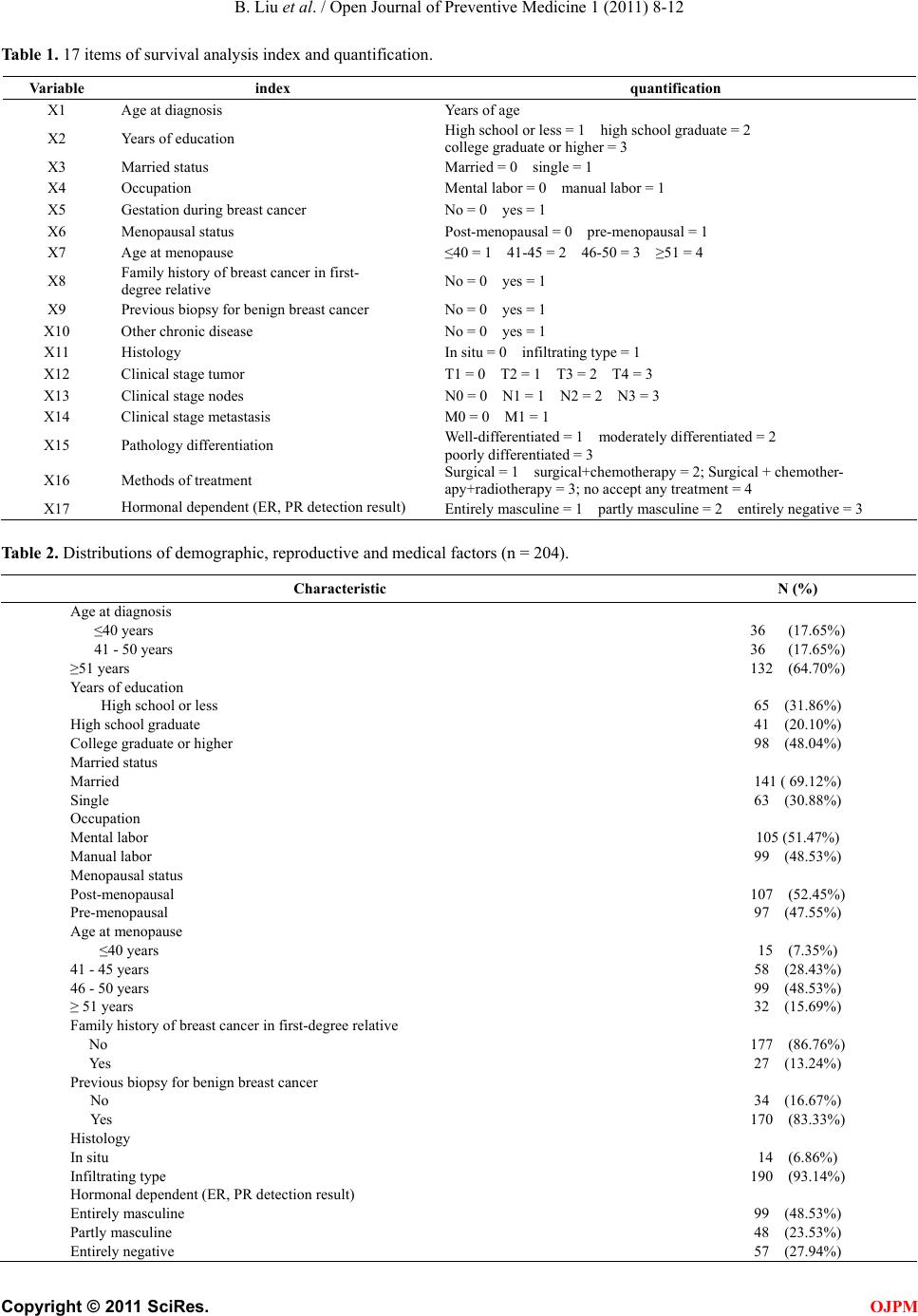
The 17 categorical variables were summarized in Table
1. For the model selection there were records with miss-
ing variables. Previous analysis on these datasets sug-
gested that missing variables might be informative.
Therefore, any missing values in the 17 categories were
coded as a separate attribute.
The distributions of various demographic, reproduc-
tive and medical characteristics of the cohort were pro-
vided in Table 2. Among the 204 women included in this
analysis, 48.04% had at least a college degree, 13.24%
had a first-degree family history of breast cancer and
83.33% had biopsy for benign breast cancer. The major-
ity was later-stage cancers, and 190 (93.14%) had infil-
trating type.
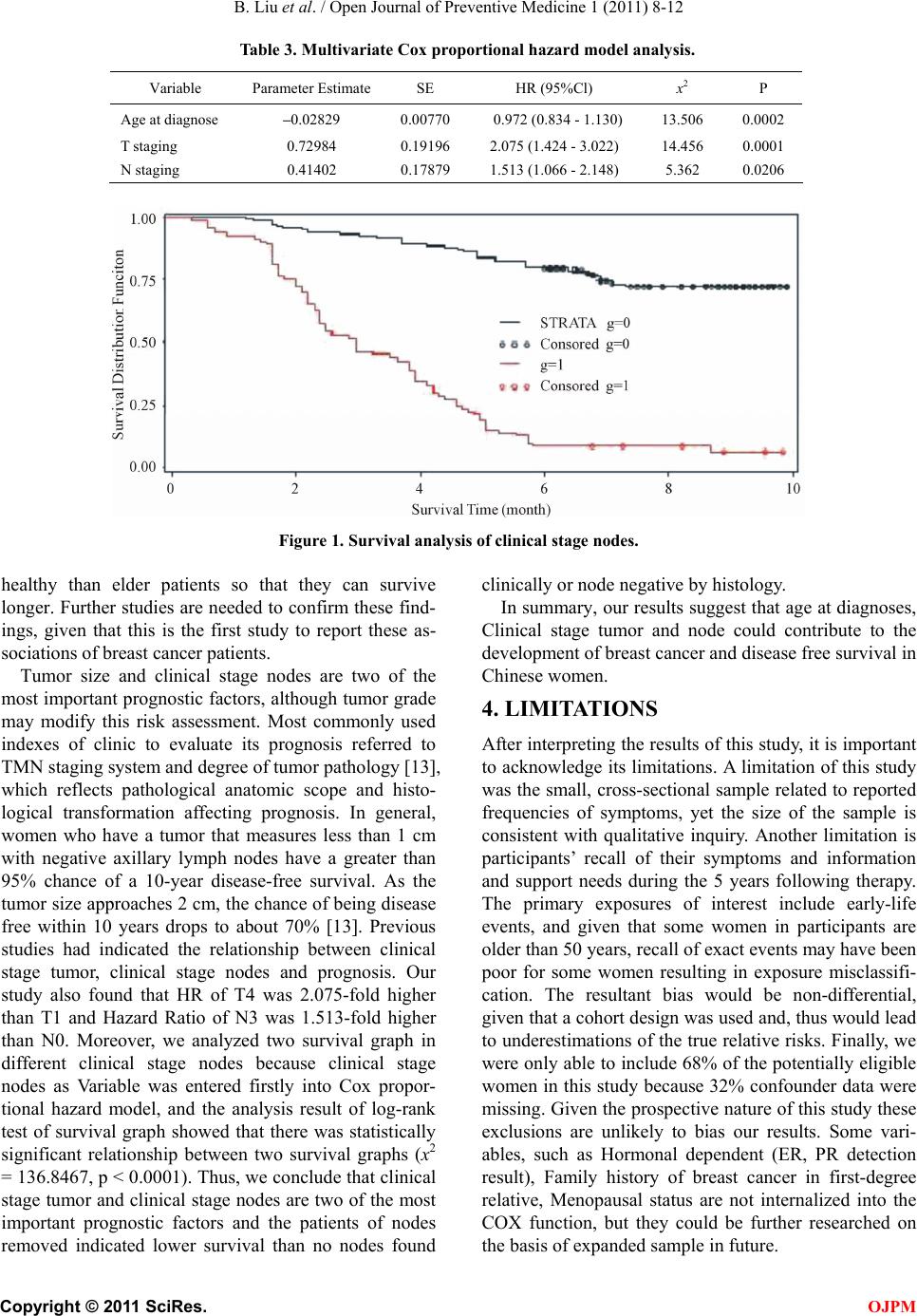
Multivariate Cox proportional hazard model analysis
was showed in Table 3. On the level of α = 0. 05, it was
indicated by analytic results that outstanding factors in-
cluding age at diagnosis, T staging, N staging, emotional
function, the level of the hospital, may influence survival
time statistically. Age at diagnosis was protective factors
(coefficient of regression was negative), the rest were all
risk factor (coefficient of regression was upright).
Survival analysis of clinical stage nodes was showed
in Figure 1. Two survival graphs of nodes found nega-
tive by histology and nodes found positive by histology
were analyzed by log-rank test, there was statistically
significant relationship between two survival graphs (x2
= 136.8467, p < 0.0001).
4. DISCUSSION
Age at diagnosis is one of the most definitive risk factors
on breast cancer. Sixty-five percent of all breast cancers
occur in women aged 55 and older. Our study found that
age at diagnosis was one of prognostic factors. The
younger patients at diagnosis showed lower death hazard
(Hazard Ratio: 0.972). But none of the prior studies
showed that age was one of the prognostic factors, and it
is difficult to hypothesize why age at diagnoses would
be more closely related to survival time. We presume
that the younger patients at diagnose may have fewer
hance of developing other chronic diseases and be more c
C
opyright © 2011 SciRes. OJPM