Health
Vol. 4 No. 8 (2012) , Article ID: 21988 , 4 pages DOI:10.4236/health.2012.48074
Assessing the relative perspective of the regulation of kinesiologists among other health professionals
![]()
1Lakehead University, Thunder Bay, Canada
2University of Leeds, Leeds, UK; *Corresponding Author: wmontelp@lakeheadu.ca, w.j.montelpare@leeds.ac.uk
Received 26 March 2012; revised 19 April 2012; accepted 29 April 2012
Keywords: kinesiology; allied health professions; clinical care
ABSTRACT
Formerly a self-governed profession, in the Province of Ontario, Canada, kinesiology was designated a regulated profession under the Regulated Health Professions Act (1991). The purpose of this study was to evaluate the perceptions of current health delivery agents to the regulation of kinesiology. An 18-item survey was used to collect data, and a SWOT (strengths, weaknesses, opportunities and threats) framework was used for analysis. The data indicated that kinesiology provides a unique expertise adding to client and patient care and is a needed partner within the multidisciplinary health environment. Similarly, despite the need for the profession to clearly define, delineate, and promote its scope of practice to professionals and to the public, there are increased opportunities that exist within the health care sector, particularly in chronic disease prevention. The addition of kinesiology as a regulated health profession was not considered to be a threat by existing key stakeholders.
1. INTRODUCTION
Kinesiology as a profession is in a state of transition in the Province of Ontario, Canada. In April 2006 the Health Professions Regulatory Advisory Council (HPRAC) submitted a recommendation to the Minister of Health and Long Term Care to regulate kinesiology under the Regulated Health Professions Act (1991) (RHPA). The RHPA provides the framework for regulating the scope of practice for health professions. Longer standing health professions under the direction of the RHPA include physicians and surgeons, chiropractors, massage therapists, occupational therapists, physiotherapists, nurses, and dietitians. In June of 2007, Bill 171 achieved royal assent within the Ontario Legislative Assembly, designating kinesiology as a regulated health profession. As a result of the passing of this legislation, students completing undergraduate kinesiology programs throughout Canada are now eligible to pursue provincial certifications, which will enable them to become part of the allied health professions’ regulated services [1].
The scope of practice for kinesiology as defined in Bill 171 and described by the Ontario Kinesiology Association (OKA) is as follows: certified kinesiologists are trained to assess, prescribe and evaluate human movement and exercise.
Bill 171 defines the scope of practice for kinesiology practitioners as, “The practice of kinesiology is the assessment of human movement and performance and its rehabilitation and management to maintain, rehabilitate or enhance movement and performance.” [1] Kinesiologists work in a variety of settings that include: hospitals, long term care facilities, rehabilitation clinics, worksites, research centres, health and fitness facilities, private practices, insurance companies, assessment companies, and wellness centres [2].
As a result of the passing of this legislation, the kinesiologist will be recognized as a highly trained and formally educated individual with a distinct knowledge base. Likewise, the practicing kinesiologist will be considered capable of working within a health care system that is increasingly focused on healthy lifestyle and exercise [3, 4]. Considering that the field of kinesiology is defined as the study of the science of human movement, the legislation enables qualified individuals—those completing the post-program process of certification (following the successful completion of a recognized undergraduate degree in Kinesiology or approved Human Kinetics program), to deliver services associated with the designated scope of practice for kinesiology [5]. Most important, accepting kinesiologists as a regulated profession will ensure that potential clients are protected by a well understood standard of practice and a level of service that will increase the quality of care and reduce the risk of harm to the public [2,3,6].
As a result of the United States Surgeon General’s Report on the health benefits of physical activity in 1996 behaviours toward exercise and physical activity in relation to health, wellness, and functional abilities have become increasingly accepted [7]. Even though kinesiology as a practice could safely provide education, assessment, and management of human movement and performance to the population [3,5], the practice of kinesiology is not widely understood or utilized by the general public or potential consumer groups (e.g. workplace, government, or rehabilitation clinics) [8]. However, as kinesiology moves from a self governed profession to a government regulated health profession in the Province of Ontario, acceptance and utilization of the practice of kinesiology by key stakeholder communities will be essential to the viability of the profession. As such, the purpose of this research was to evaluate the perceptions of current health service delivery agents about the impact of introducing kinesiology as a regulated health profession on their own disciplinary practice. The intent of collecting this data was to provide evidence to inform future program development and continuing education for the regulated profession of kinesiology.
2. METHODS
The primary method for data collection in this study was a computer based self-administered survey consisting of 18 questions. The study was conducted using a two stage approach in which the first stage was used to develop the questionnaire items, and the second stage used a non-probabilistic convenience sample of sixtytwo health care providers to gain insight about the impact of introducing kinesiology as a regulated health profession.
2.1. Development of the Survey Items Using a Focus Group Approach
The researchers developed an electronic survey tool that was comprised of two parts: 1) a series of demographic items that could identify the characteristics of the respondents; and 2) a series of open-ended questions based on a SWOT1 model of assessment. Using the SWOT approach, the researchers assessed the impact of adding kinesiology as a regulated profession to the existing cadre of allied health professions. As a first step in creating the appropriate language for open-ended questions, the researchers identified specific individuals that were currently practicing in fields that represent the key stakeholder communities associated with kinesiology. After receiving approval from the University Research Ethics Board, a focus group consisting of a chiropractor, physiotherapist, massage therapist, rehabilitation consultant, certified kinesiologists, a medical exercise specialist, and a personal trainer were invited to participate as the expert panel. An informal process of engagement was next organized and the purpose of the research was explained in detail. The focus group reviewed the questions for language, readability, and clarity of purpose.
The general consensus was that although the purpose of the survey was clear, the wording and language were at times cumbersome. The focus group flagged weaknesses in the survey language such as the use of double-barreled questions, and also recommended that the researchers use a web-delivered survey rather than a text-based document. The survey was edited and a computer generated web-format was created to deliver the questionnaire to the designated group of respondents.
2.2. Distribution of the Survey and the Research Sample
The research sample was comprised of specific practitioners within the allied health professions that have been identified as colleagues, competitors, and employers of kinesiology graduates. In this way, the researchers were able to obtain a comprehensive overview of the market in which kinesiologist will practice.
The sampling frame consisted of 10 associations, each representing members of the allied health professions, and included physical fitness professionals & personal trainers, physiotherapists, chiropractors, occupational therapists, as well as massage therapists. In addition, respondents included Province of Ontario public health employees, dietitians, nurses, and rehabilitation consultants. Participants were recruited through email addresses posted to the various profession based web-sites.
A total of sixty-two invitations to participate were distributed to members of the identified allied health professions. Specifically, invitations were sent to the managing directors of 10 associations drawn from the allied health professions, and an additional 52 e-mail invitations were sent to current practitioners from the various stakeholder groups mentioned above. Respondents were invited to circulate the survey website to members of their respective associations if they wished.
2.3. Survey Format and Data Collection
The eighteen-item survey was written in standard hypertext mark-up language with data capture functions that were written in PHP. The survey was distributed as an electronic self-administered questionnaire. The uniform resource locator (URL) for the survey’s home page was embedded in the introductory letter so that participants could link directly to the site. The home page provided a link to background information about the survey including a letter of informed consent, as well as a link to the electronic survey. The survey was tested to ensure that data were being captured accurately and completely using the selected Internet protocol.
All participants were informed that their participation was completely voluntary and anonymous, and that they were free to withdraw from the study at anytime. No individual was identified in any report of the results and a summary of the results could be made available to the respondent upon request at the completion of the study.
3. RESULTS
3.1. Part 1: Demographic Characteristics
Fifty-six of the initially distributed sixty-two surveys were returned for a response rate of ninety percent. The sample consisted of slightly more female than male respondents (66% female; 44% male), with most of the respondents in the 30 - 40 year age decile. Twenty-five percent of the respondents were below the age of 30, while the remaining respondents were above age 40. Seventy five percent of the sample had completed at least a four-year undergraduate degree, of which more than one-third of the group (35%) had successfully completed a graduate or professional level degree.
The current professional position of the respondent at the time of participating in the survey is summarized in Table 1, below.
A further analysis of these data indicates that slightly more than half of the respondents (52%) were currently regarded as regulated professionals and from this group, some 10% were also Ontario Kinesiology Association
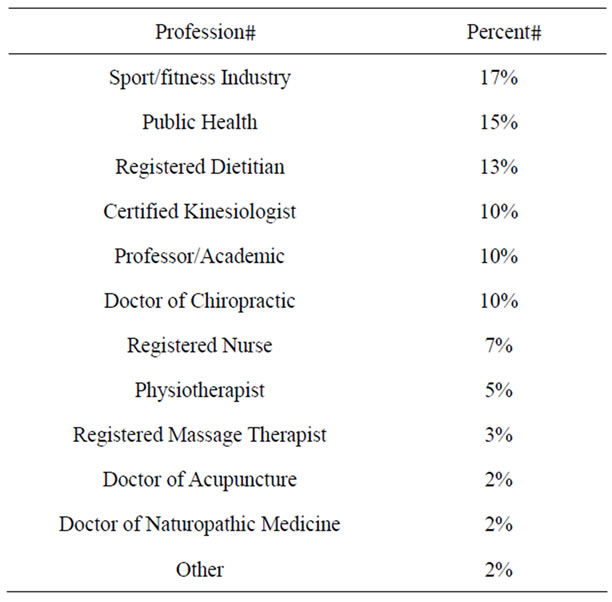
Table 1. Professional makeup of respondents by percentage.
certified kinesiologists. The remaining respondents included kinesiology related professors/acade-mics, fitness/ sport industry workers, public health workers, health promoters, and managers. Fifty-five percent of respondents had been in their current position less than 10 years, while more than 28% had been in the current position between 11 and 20 years.
The type of workplace setting represented by the respondents included professionals in public health (17%), private practice (13%), and the fitness/sport industry (10%). The workplace funding structure is outlined in Table 2 below.
Thirty percent of the respondents lived in areas with a population between 10,001 - 50,000 while 34% of respondents lived in areas with a population base between 50,001 - 100,000. Twenty one percent lived in areas with a population greater than 100,000 and the remaining respondents were designated as unattributed.
3.2. Part 2: Perceptions about the Impact of Adding Kinesiology to the Cadre of Regulated Allied Health Professions
Responses to the open ended questions assessing the impact of adding kinesiology as a regulated profession to the current group of allied health professions were evaluated independent of the questions about respondent demographics. Specific themes were identified for each question in the second part of the survey using theme identification techniques suggested by Ryan and Bernard [9]. Responses to each question were reread a minimum of six times by the lead researcher. This repeated scanning approach allowed for initial understanding of patterns in word repetition, phrase, and theme. Repeated words and phrases were then identified and underlined. Repeated words and phrases were used to develop key themes. Each key theme for each question was then given an identifying colour code. The colour codes were collated using a cut and paste method. A summary table was designed for each of the questions. The summary tables included all key themes identified for each question with all supporting data that had been collected from the respondents’ answers.
The themes identified by the lead researcher were verified by the focus group representing key stakeholders.
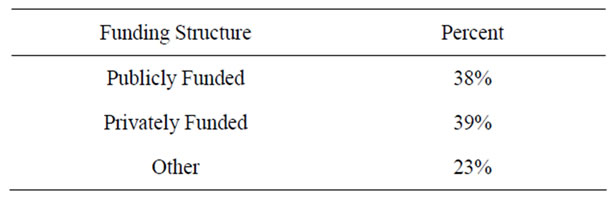
Table 2. Funding structure of respondents workplace by percentage.
Through a process of response review, the focus group was charged with the task of identifying key themes for each question. The key phrases and themes identified by the focus group for the specific questions matched the key phrases and themes identified by the lead researcher, thereby corroborating the initial distillation process.
The majority of the respondents (sixty-six percent) were aware that the practice of kinesiology had recently been regulated. Eighty percent of the respondents either strongly agreed or agreed with the change to regulation. Only five percent of respondents disagreed with regulation, and no respondents indicated that they strongly disagreed with the move to regulate kinesiology.
3.3. Strengths
Survey respondents stated that including kinesiology as a regulated health profession would increase multidisciplinary collaboration, provide the health system with a unique expertise that could potentially increase continuity of care for the client, and fill the gap between wellness and disease to increase total care for clients and patients.
In addition, respondents indicated that regulating the practice of kinesiology provided explicit standardization of practice, and thereby increased public safety. With a clearly understood standard of practice, the respondents noted that there would be uniform credentialing, control, and monitoring of the level of practice, and a reduction in fraudulent behaviours which, in turn, was viewed as a necessary precursor to increase professional credibility among kinesiologists. The major strengths identified by respondents are presented in Table 3, below.
3.4. Weakness
The primary weakness of the practice of kinesiology is the confusion about the role of kinesiology in general terms. Survey respondents saw the need for the profession to have a clearly defined and understood level of knowledge and scope of practice. This is especially important
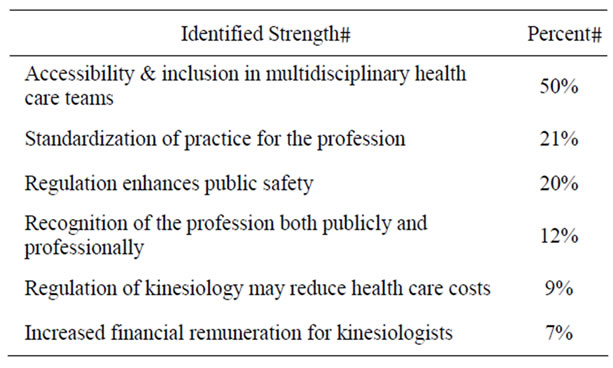
Table 3. Strengths of a regulated kinesiology profession by percent of responses.
as kinesiology transitions into a mainstream regulated health profession. Respondents stated that there is a need to not only define their (kinesiologists) specific role as a profession, but also identify and clarify how kinesiology overlaps and/or differs from the scope offered by other health care professionals. The apparent lack of understanding by the public of the role of kinesiologists is an area that the College of Kinesiology will need to address in the future. Respondents indicated that there is a lack of public knowledge as well as professional awareness about the educational background, level of knowledge, and practical skills kinesiologists have acquired through their academic training. This lack of understanding of kinesiology as a profession may lead to reduced utilization by other regulated health professionals thereby reducing future opportunities for collaboration between kinesiologists and other health service delivery professionals. The major weaknesses identified by respondents are presented in Table 4, below.
3.5. Opportunities
Fifty percent of the respondents indicated that regulation of kinesiologists would enhance health care delivery within their organization, while 28% stated explicitly that including kinesiologists as a regulated health profession would not enhance their health care delivery.
Overall, the respondents indicated that regulation will increase career viability for kinesiologists by providing more opportunity to practice in areas such as, chronic disease prevention, health promo-tion programming, general health programs, rehabilitation settings, and independent business.
Increased opportunities within the larger health care delivery system also increase the integration into multidisciplinary health teams providing a team approach to solving client and/or patient issues and providing an opportunity to extend networks among health professionals. Respondents viewed this inclusion into the cadre of health professionals as an opportunity to enhance the overall quality of Ontario’s community health centres and family health teams.
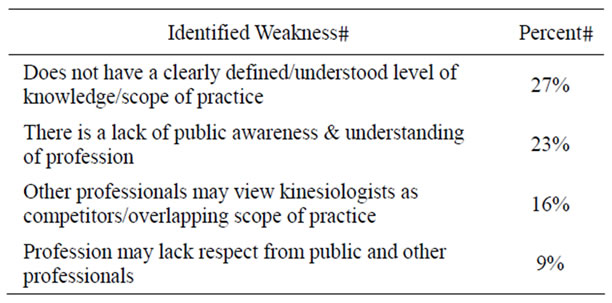
Table 4. Weaknesses of a regulated kinesiology profession by percent of responses.
According to the response data, as regulated professionals, kinesiologists have an opportunity to educate and mentor within health care agencies, institutions and the fitness industry, particularly on subjects pertaining to health promotion, chronic disease prevention and management. A less noted opportunity identified by the respondents was the opportunity to charge for services directly through various insurance systems, and as such increase visibility and service delivery. Major opportunities identified for kinesiologists are presented in Table 5, below.
3.6. Threats
Forty-eight percent of respondents did not feel that the regulation of kinesiology would pose a threat to their profession. Conversely, eighteen percent of the respondents indicated that by creating an additional regulated health profession (i.e. certified kinesiology) there would be too much similarity and overlap in scope of practice among health care deliverers. In particular, the potential for infringement of kinesiologists on the current health delivery stakeholders was considered a threat by this cohort of respondents. Individuals opposed to the regulation of kinesiologists suggested that there would be an unnecessary diverting of patients and clients away from existing caregivers and an increased competition in the marketplace.
3.7. Allied Health Professionals Advice to the Kinesiology Profession
The respondents were asked what advice they may have for the profession as it moves through the transition into a regulated profession. Respondents identified the need to emphasize education and awareness of the academic and practical expertise of the profession and its scope of practice, particularly to decision makers. Likewise, individuals advised that there is a distinct need to collaborate with other health professionals in a non-adversarial team oriented approach, being respectful and understanding of skills and knowledge of others within the multidisciplinary health care environment.
With regard to program development the respondents indicated that education was needed in the areas of health

Table 5. Opportunities identified as a result of regulation.
promotion, population health, and in disease prevention. Furthermore, respondents noted that kinesiologists as a regulated health profession needed to maintain professional development, stay current in terms of literature, and maintain standards and ethics.
4. CONCLUSION
The main intention of this study was to gather perceptions of stakeholders and caregivers to the introduction of kinesiology as a regulated health profession. The results indicated that kinesiology as a regulated health profession has the potential to increase career viability through the acceptance of kinesiologists as part of the cadre of allied health professionals. Further, the public will surely benefit from the unique expertise offered by the kinesiologist to the continuum of care. However, a major hurdle in this transition process is for kinesiologists to be able to clearly define who they are, promote what they can contribute, and demonstrate that they can establish excellence in delivering service within the clearly defined scope of practice.
![]()
![]()
REFERENCES
- The Legislative Assembly of Ontario (2007) An act to improve health systems by amending or repealing various enactments and enacting certain act. Bill, 171, 127-130. http://www.ontla.on.ca/bills/bills-files/38_parliment/session2/b171.pdf
- The Ontario Kinesiology Association’s Submission for Regulation under the Regulated Health Professions Act (2005) Ontario kinesiology association document. http://www.hprac.org/english/default.asp
- Malek, M.H., Nalbone, D.P., Berger, D.E. and Coburn, J.W. (2002) Importance of health science education for personal fitness trainers. The Journal of Strength and Conditioning Research, 16, 19-24. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=11834102&dopt
- Miller, M.G. and Berry, D. (2000) Health-related physical fitness knowledge of student allied health professions. Evaluation & the Health: Professions, 23, 305-317. http://ehp.sagepub.com/cgi/content/refs/23/3/305 doi:10.1177/01632780022034624
- Shephard, R.J. and Bonneau, J. (2003) Supervision of occupational fitness assessments. Canadian Journal of Applied Physiology, 28, 225-239. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=12825332&dopt doi:10.1139/h03-018
- Springer, B.L. and Clarkson, P.M. (2003) Two cases of exertional rhabdomyolysis precipitated by personal trainers. Medicine & Science in Sport & Exercise, 35, 1499- 1502. http://www.acsm-msse.org/pt/re/msse/abstract.00005768-200309000-00007.htm;jsessionid=LKGBp5hzmrrFRpDllcFhvF2x81lrZllhKNn1QPH4qPyPgQLBjbxS!1593807172!181195629!8091!-1
- National Centre for Chronic Disease Prevention and Health Promotion (1996) Physical activity and health: A report of the surgeon general executive summary. http://www.cdc.gov/nccdphp/sgr/summary.htm
- Knudson, D. (2005) Evidence-based practice in kinesiology: The theory to practice gap revisited 2005. Physical Educator, 62, 212-221. http://search3.scholarsportal.info.ezproxy.lakeheadu.ca/ids70/results.php?id=2&page_no=2&log=page&SID=976e8221fcb33d25cfa219b43e03b871&mark_id=search%3A2%3A4%2C10%2C20#pubtypes
- Ryan, G. and Bernard, H. (1994) Techniques to identify themes in qualitative data. http://www.analytictech.com/mb870/Readings/ryan-bernard_techniques_to_identify_themes_in.htm
NOTES
1SWOT: Strengths, Weaknesses, Opportunities, and Threats.