World Journal of Cardiovascular Diseases
Vol.03 No.03(2013), Article ID:33343,3 pages
10.4236/wjcd.2013.33045
Retinal hemorrhage as a unique ophthalmic manifestation of cerebral hyper perfusion syndrome
Eitan Heldenberg, Arie Bass
Department of Vascular Surgery, Assaf Harofeh Medical Center, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
Email: eitan@heldenberg.name
Copyright © 2013 Eitan Heldenberg, Arie Bass. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 10 April 2013; revised 12 May 2013; accepted 25 May 2013
ABSTRACT
Cerebral hyperperfusion syndrome (CHPS) is a rare disease with complications of carotid artery revascu- larization. Acute retinal hemorrhage is a very rare entity that has been previously described as a mani- festation of CHPS followed by the carotid artery sten- ting (CAS), but to the best of our knowledge, not yet described as a complication of carotid surgery. An Ascending Aorta to bilateral Carotid bypass was per- formed in a 35 years old woman with active Takayasu arteritis and 95% symptomatic stenosis of both common carotid arteries. Severe retinal hemorrhage appeared on the second post operative day combined with high blood pressure, brain edema on CT scan and grand mal seizures. It seems that fundoscopic examination followed by the carotid revascularization of tightness can be helpful in identifying those pa- tients who develop symptoms suggesting of CHPS.
Keywords:
Cerebral Hyper Perfusion Syndrome; Takayasu Arteritis; Retinal Hemorrhage
1. INTRODUCTION
Cerebral hyperperfusion syndrome (CHPS) was first de- scribed by Sundt in 1981. It is a potentially lethal com- plication directly related to carotid revascularization [1]. CHPS presents with a wide spectrum of manifestations ranging from mild headaches, to lethal intracerebral hemorrhage (ICH) [1,2]. The incidence of CHPS, as re- viewed in various clinical series, has been 0.3% - 2.7% [2].
We herein described retinal hemorrhage as a manifesta- tion of CHPS in a young patient with Takaysu’s arteritis who underwent Ascending Aorta to bilateral distal Com- mon Carotid Arteries bypass and developed brain edemas as a manifestation of CHPS.
2. Case Presentation
A 35 years old previously healthy female, was admitted to the department of neurology with right hemiparesis and motor aphasia. Carotid duplex demonstrated diffuse thickening of both Common Carotid Arteries (CCA) without any pathology of the bifurcation or the Internal Carotid Arteries (ICA). Aortic arch and cervical vessel computerized tomographic angiography demonstrated 95% stenosis of both CCA, complete occlusion of the left Subclavian Artery (SCA) and 90% stenosis of the right SCA.
Based on the clinical presentation, imaging findings and elevated ESR [4-6], the patient was diagnosed as suffering from Takayasu Arteritis, and steroid therapy (Prednisone 20 mg daily) was initiated. As all cervical arteries were either occluded or tightly stenosed, we pre- formed an Ascending Aorta to bilateral CCA bifurcation bypass using a 14 ×
3. Discussion
CHPS is a well known entity among vascular surgeons

Figure 1. MRI examination visualizing the Aorto-Bi-Carotid (ABC) bypass. The graft is emerging off the ascending aorta and its limbs were anastomosed end-to-end to the distal com- mon carotid arteries.
who treat carotid artery disease, either by endarterectomy or stenting, with an average incidence of 0.3% - 2.7% [1].
It seems that the risk of developing CHPS is increased among patients with severe, diffuse cerebrovascular dis- ease, such that the worse the occlusive disease and the more cerebral vessels involved, the higher the probability of developing CHPS.
The pathogenesis, although obscure, is attributed to the failure of autoregulation of cerebral blood flow in chronically hypoperfused brain hemispheres followed by the revascularization. Maximal dilatation of cerebral ar- terioles secondary to marginal arterial perfusion may cause loss of cerebral vascular auto regulation. This, in conjunction with uncontrolled hypertension, may result in brain edema or intracerebral hemorrhage (ICH) once normal blood flow has been restored [1,3]. The intra- cerebral edema may further worsen the hypertension resulting in further hyperperfusion.
Although the literature is replete with descriptions of CHPS, there is a lack of literature regarding its ophthal- mic manifestation CHPS [4]. Only one recent publication regarding retinal hemorrhage followed by the carotid art- ery stenting (CAS) as a manifestation of CHPS has been published [5].
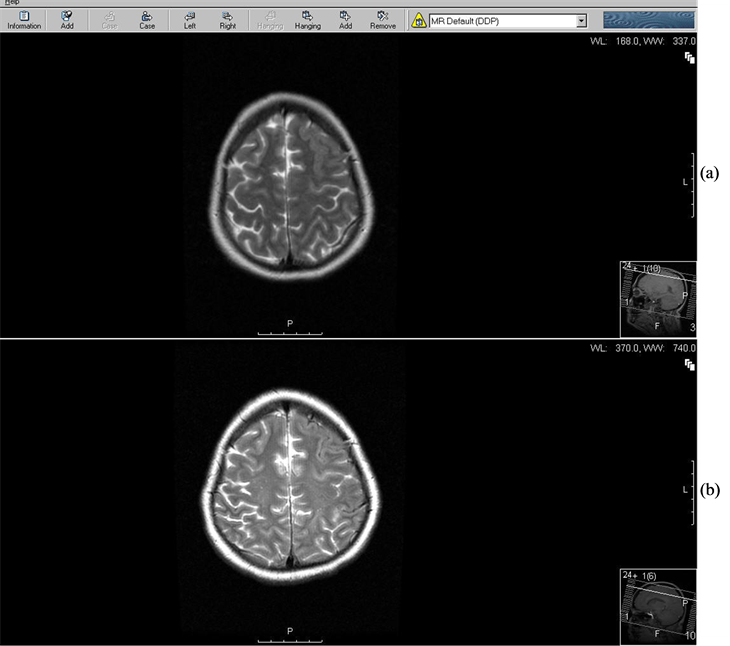
Figure 2.Brain MRI four days after cerebral revascularization is demonstrating vasogenic edema (VE) in the left frontal lobe (a). Five weeks later the edema has disappeared (b).
 (a) (b)
(a) (b)
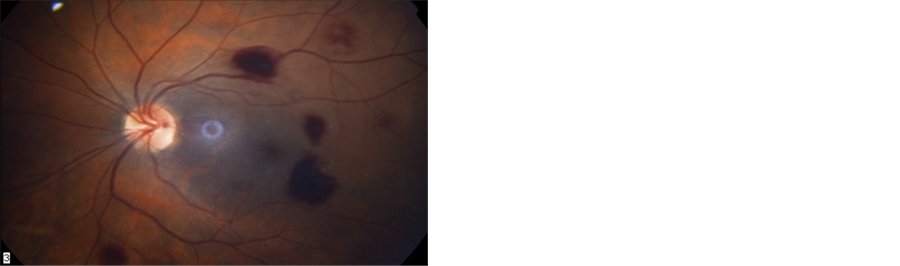
Figure 3. Fundoscopic examination four days after revascularization. Multiple retinal hemorrhages are demonstrated in both eyes (a). Three weeks later most hemorrhages have been absorbed (b).
The symptoms of impaired visual acuity in our patient could have been attributed to vasogenic brain edema, which was demonstrated by MRI. Previous case reports described an association between reversible cortical blind- ness and vasogenic cerebral edema among patients with severe postpartum preeclampsia [6].
Our patient presented with fundoscopic evidence of binocular retinal hemorrhages, coinciding with brain vasogenic edema. This linkage may reflect a rather un- recognized entity of bleeding within neuronal tissue, related to capillary leak, in the setting of uncontrolled hy- pertension. Furthermore, routine use of Aspirin and Clo- pidogrel, and utilization of anticoagulants during surgery may further increase the risk of bleeding.
This unusual case illustrates that fundoscopic exami- nation may be useful in diagnosing CHPS after carotid revascularization.
REFERENCES
[1] Sundt, T.M., Sharbourgh, F.W., Piepgras, D.G., Kearns, T.P., Messick, J.M., O’Fallon, W.M. (1987) Correlation of cerebral blood flow and electroencephalographic changes during Endarterectomy: With results of surgery and hemodynamic of cerebral ischemia. Mayo Clinic Pro- ceedings, 56, 533-543.
[2] Ogasawara, K., Mikami, C., Inoue, T. and Ogawa, A. (2004) Delayed cerebral hyperperfusion syndrome caused by prolonged impairment of cerebrovascular auto regula- tion after carotid end arterectomy: Case report. Neuro- surgery, 54, 1258-1262. doi:10.1227/01.NEU.0000120064.55339.F9
[3] Krapanayiotides, T., Meuli, R., Devuyst, G., Piechowski, Jozwiak, B., Dewarrat, A., Ruchat, P., Segger, V.L. and Bogousslasky, J. (2005) Post carotid endarterectomy hy- perperfusion or reperfusion syndrome. Stroke, 6, 21-36.
[4] Nicholas, G.G., Hashemi, H., Gee, W. and Reed, F.J. (1993) The cerebral hyperperfusion syndrome: Diagnostic value of ocular pneumoplethysmography. Journal of Vascular Surgery, 17, 690-695. doi:10.1016/0741-5214(93)90112-Y
[5] Kim, D.Y., Kim, B.M., Park, H. and Chung, J. (2011) Retinal hemorrhage as an initial sign of cerebral hyper- perfusion Syndrome after carotid artery stenting. Acta Neurochirurgica, 154, 75-77. doi:10.1007/s00701-011-1194-z
[6] Do, D.V., Rismondo, V. and Nyguyen, Q.D. (2002) Rever- sible cortical blindness in preeclampsia. American Jour- nal of Ophthalmology, 134, 916-918. doi:10.1016/S0002-9394(02)01753-1