N. Zou et al. / Health 3 (2011) 271-275
Copyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/
274
males than in males, 2) the prevalence of persistent fa-
tigue increased with age, 3) persistent fatigue was ac-
companied by psychological disorders such as depres-
sion and anxiety, and 4) the appearance of persistent
fatigue was associated with lifestyle. Among lifestyle,
unhealthy dietary life and irregular sleep habits have
been demonstrated as causative factors of persistent fa-
tigue.
In comparison with western countries, the epidemiol-
ogical study of fatigue in healthy adolescents in Asian
countries is quite scanty. Okamoto et al. investigated the
characteristics of fatigue in association with lifestyle in
247 healthy Japanese adolescents and found that the
complaints most frequently observed were drowsiness
and dullness, followed by difficulty of concentration
[17]. Moreover, undesirable eating habits or poor life-
style, such as staying up late at night, were associated
with the degree of fatigue. Recently, it is reported that
fatigue is largely affected by physical fitness level but
very little by exercise habits in healthy Japanese adoles-
cents aged 15 - 20 years [18]. We have recently reported
the fatigue status in 1225 Japanese adolescents aged
between 11 and 16 yrs by the questionnaire used in the
present study, but the method of data collection was
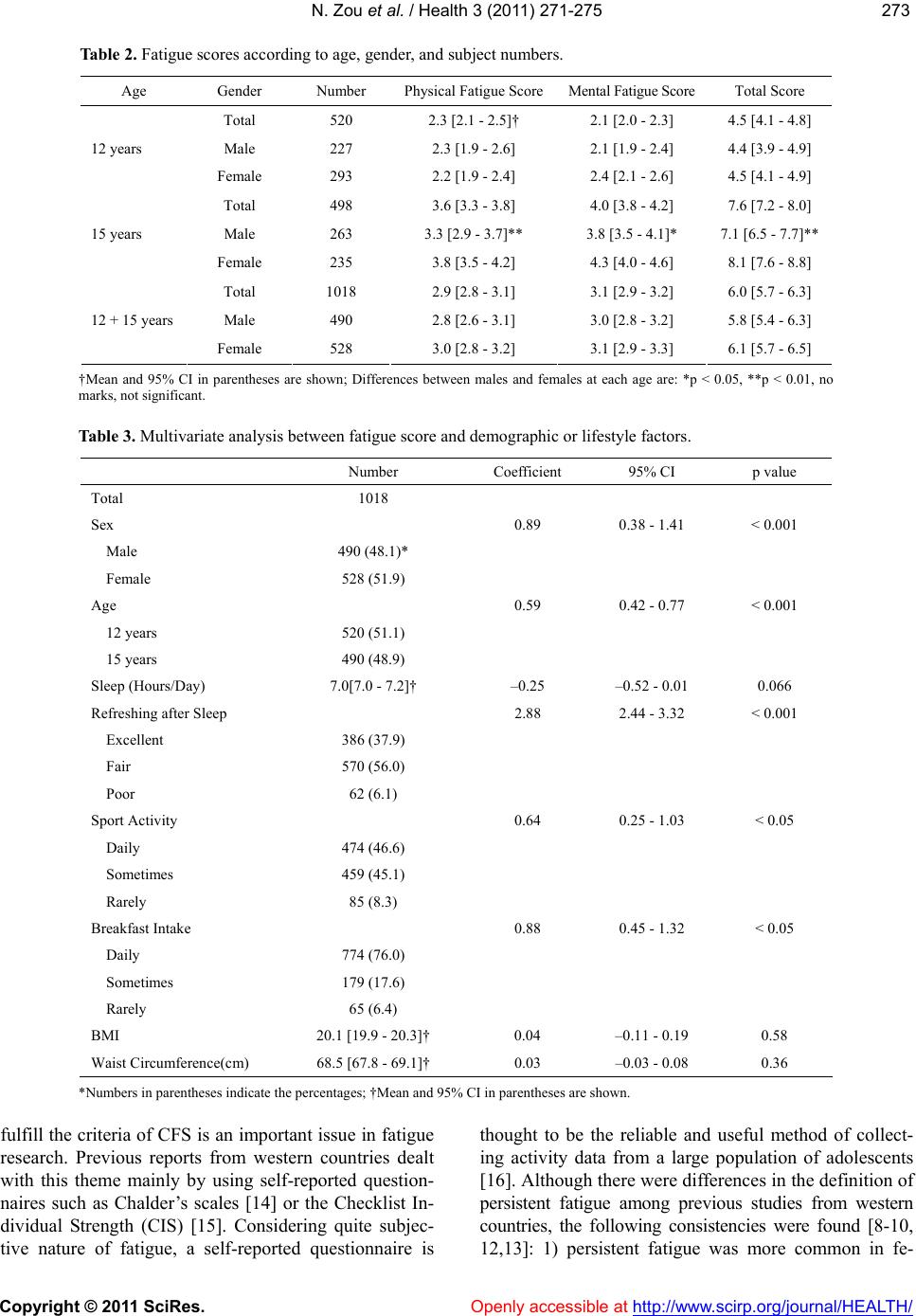
“self-reported” [19]. In this study, the fatigue scores in-
creased significantly with age, but there was no gender
difference at any age. Moreover, subjects with higher
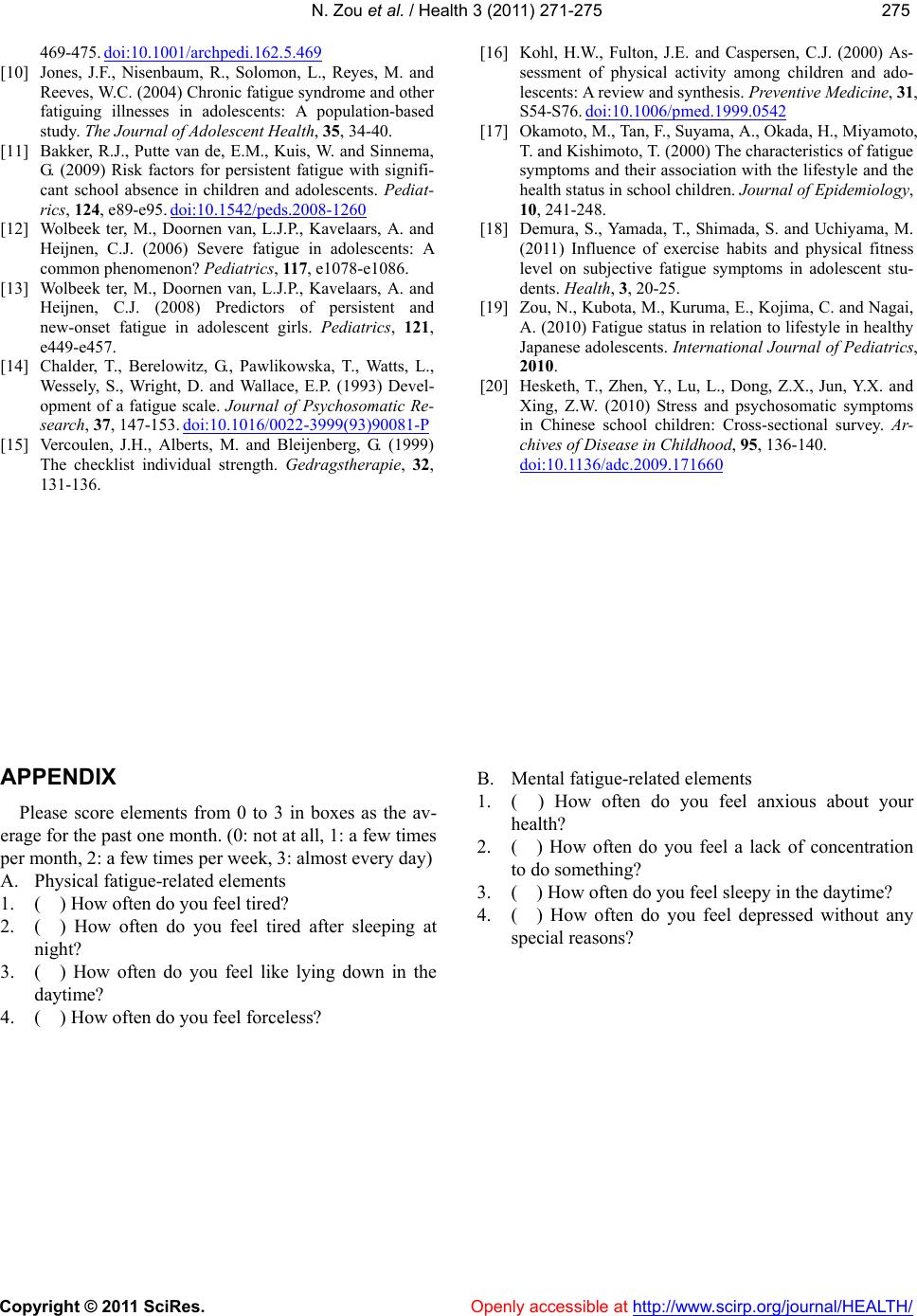
fatigue scores tended to skip breakfast more frequently,
and to have less balanced eating habits or lesser sleep
duration, as in the present study. “To feel sleepy in the
daytime” was the commonest complaint followed by “to
feel often tired”. On the other hand, “lack of concentra-
tion” was the 5th most common complaint. We are un-
certain about the reason for this disparity in findings
between Chinese and Japanese adolescents. One possible
explanation is that there exist basic differences of daily
lifestyle in adolescents between Jixi and Nara cities,
although both cities are classified as middle class urban
cities in their respective countries.
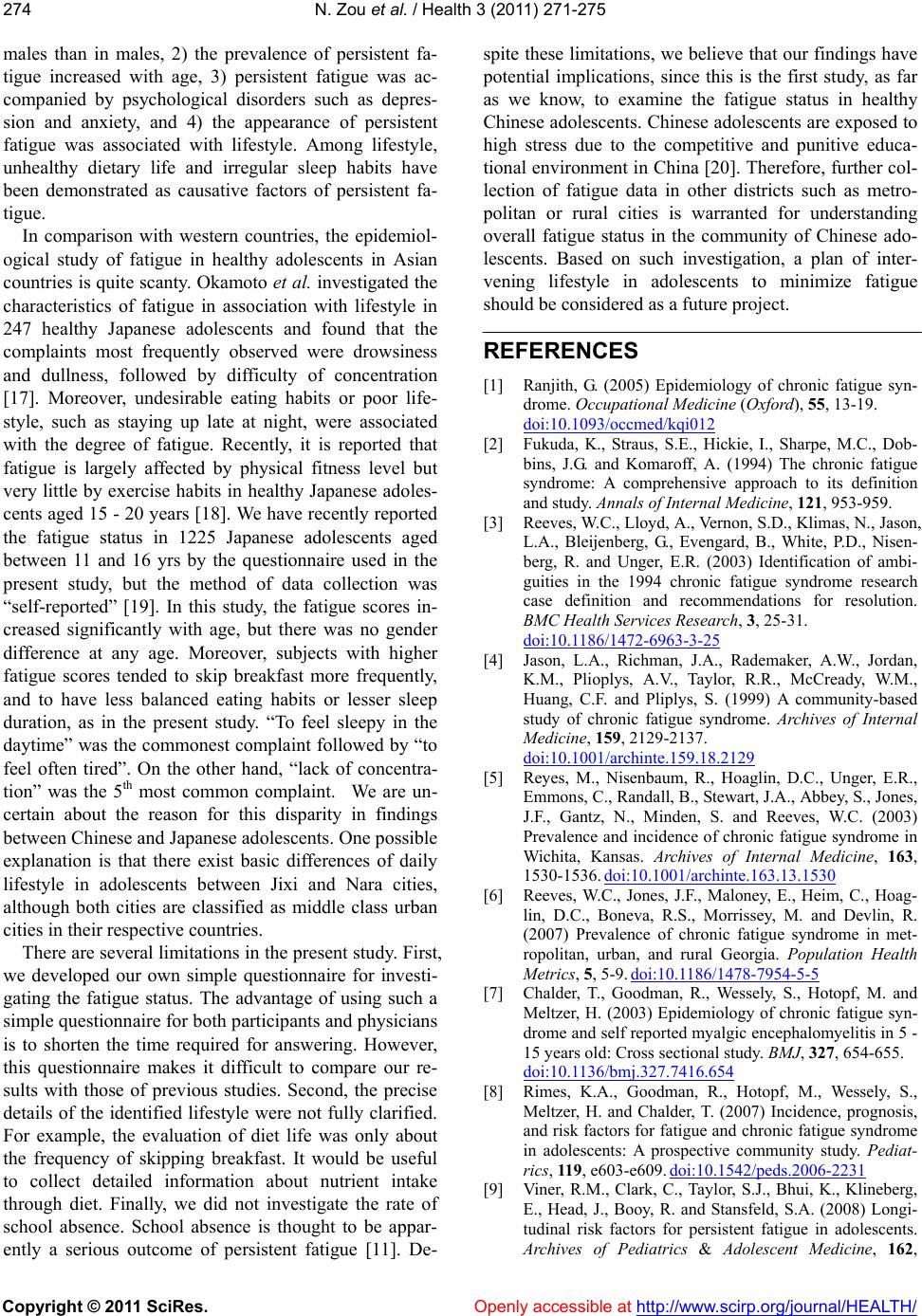
There are several limitations in the present study. First,
we developed our own simple questionnaire for investi-
gating the fatigue status. The advantage of using such a
simple questionnaire for both participants and physicians
is to shorten the time required for answering. However,
this questionnaire makes it difficult to compare our re-
sults with those of previous studies. Second, the precise
details of the identified lifestyle were not fully clarified.
For example, the evaluation of diet life was only about
the frequency of skipping breakfast. It would be useful
to collect detailed information about nutrient intake
through diet. Finally, we did not investigate the rate of
school absence. School absence is thought to be appar-
ently a serious outcome of persistent fatigue [11]. De-
spite these limitations, we believe that our findings have
potential implications, since this is the first study, as far
as we know, to examine the fatigue status in healthy
Chinese adolescents. Chinese adolescents are exposed to
high stress due to the competitive and punitive educa-
tional environment in China [20]. Therefore, further col-
lection of fatigue data in other districts such as metro-
politan or rural cities is warranted for understanding
overall fatigue status in the community of Chinese ado-
lescents. Based on such investigation, a plan of inter-
vening lifestyle in adolescents to minimize fatigue
should be considered as a future project.
REFERENCES
[1] Ranjith, G. (2005) Epidemiology of chronic fatigue syn-
drome. Occupational Medicine (Oxford), 55, 13-19.
doi:10.1093/occmed/kqi012
[2] Fukuda, K., Straus, S.E., Hickie, I., Sharpe, M.C., Dob-
bins, J.G. and Komaroff, A. (1994) The chronic fatigue
syndrome: A comprehensive approach to its definition
and study. Annals of Internal Medicine, 121, 953-959.
[3] Reeves, W.C., Lloyd, A., Vernon, S.D., Klimas, N., Jason,
L.A., Bleijenberg, G., Evengard, B., White, P.D., Nisen-
berg, R. and Unger, E.R. (2003) Identification of ambi-
guities in the 1994 chronic fatigue syndrome research
case definition and recommendations for resolution.
BMC Health Services Research, 3, 25-31.
doi:10.1186/1472-6963-3-25
[4] Jason, L.A., Richman, J.A., Rademaker, A.W., Jordan,
K.M., Plioplys, A.V., Taylor, R.R., McCready, W.M.,
Huang, C.F. and Pliplys, S. (1999) A community-based
study of chronic fatigue syndrome. Archives of Internal
Medicine, 159, 2129-2137.
doi:10.1001/archinte.159.18.2129
[5] Reyes, M., Nisenbaum, R., Hoaglin, D.C., Unger, E.R.,
Emmons, C., Randall, B., Stewart, J.A., Abbey, S., Jones,
J.F., Gantz, N., Minden, S. and Reeves, W.C. (2003)
Prevalence and incidence of chronic fatigue syndrome in
Wichita, Kansas. Archives of Internal Medicine, 163,
1530-1536. doi:10.1001/archinte.163.13.1530
[6] Reeves, W.C., Jones, J.F., Maloney, E., Heim, C., Hoag-
lin, D.C., Boneva, R.S., Morrissey, M. and Devlin, R.
(2007) Prevalence of chronic fatigue syndrome in met-
ropolitan, urban, and rural Georgia. Population Health
Metrics, 5, 5-9. doi:10.1186/1478-7954-5-5
[7] Chalder, T., Goodman, R., Wessely, S., Hotopf, M. and
Meltzer, H. (2003) Epidemiology of chronic fatigue syn-
drome and self reported myalgic encephalomyelitis in 5 -
15 years old: Cross sectional study. BMJ, 327, 654-655.
doi:10.1136/bmj.327.7416.654
[8] Rimes, K.A., Goodman, R., Hotopf, M., Wessely, S.,
Meltzer, H. and Chalder, T. (2007) Incidence, prognosis,
and risk factors for fatigue and chronic fatigue syndrome
in adolescents: A prospective community study. Pediat-
rics, 119, e603-e609. doi:10.1542/peds.2006-2231
[9] Viner, R.M., Clark, C., Taylor, S.J., Bhui, K., Klineberg,
E., Head, J., Booy, R. and Stansfeld, S.A. (2008) Longi-
tudinal risk factors for persistent fatigue in adolescents.
Archives of Pediatrics & Adolescent Medicine, 162,