K. Alexander et al. / Health 3 (2011) 263-270
Copyright © 2011 SciRes. http://www.scirp.org/journal/HEALTH/
269269
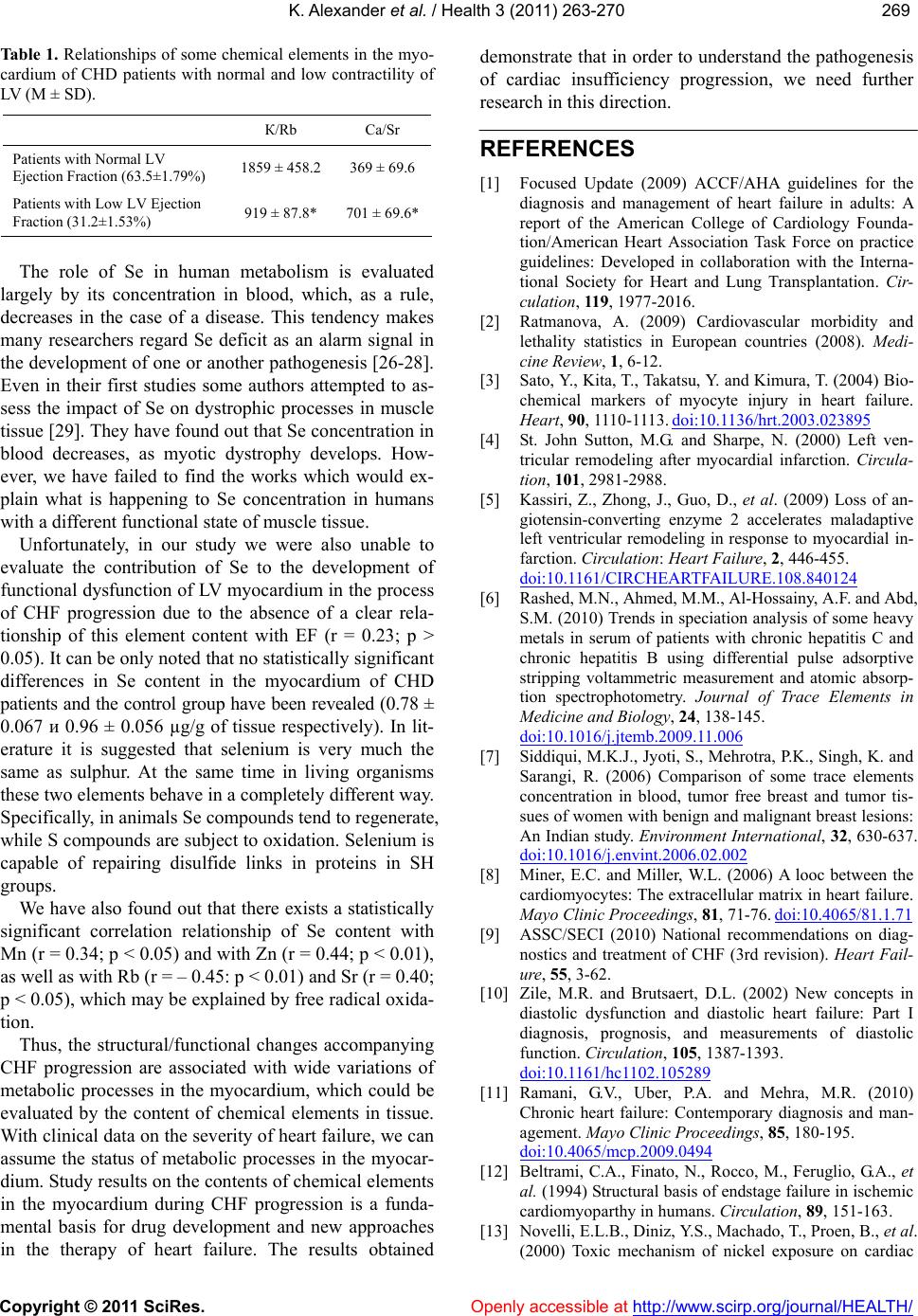
Table 1. Relationships of some chemical elements in the myo-
cardium of CHD patients with normal and low contractility of
LV (M ± SD).
К/Rb Ca/Sr
Patients with Normal LV
Ejection Fraction (63.5±1.79%) 1859 ± 458.2 369 ± 69.6
Patients with Low LV Ejection
Fraction (31.2±1.53%) 919 ± 87.8* 701 ± 69.6*
Openly accessible at
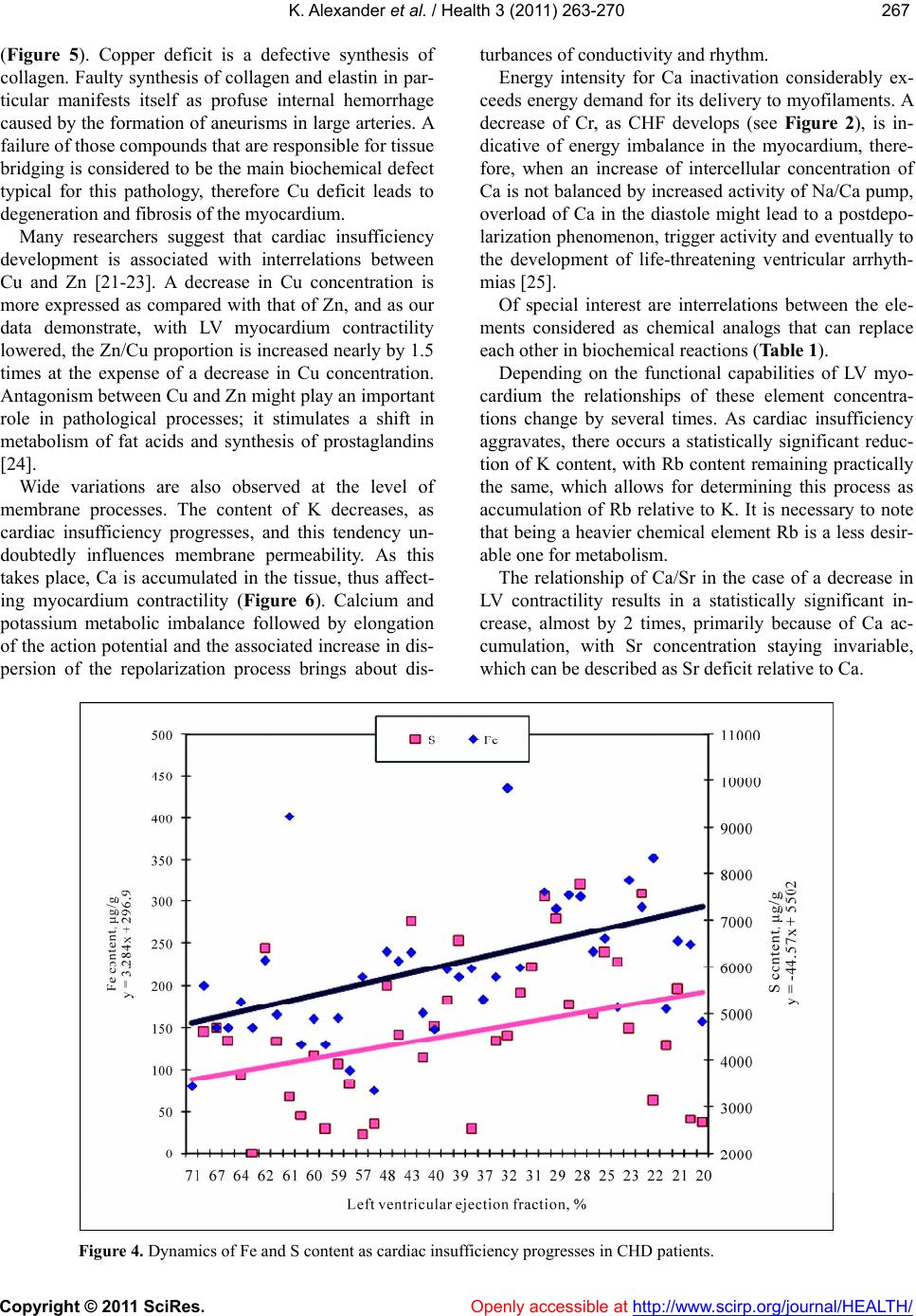
The role of Se in human metabolism is evaluated
largely by its concentration in blood, which, as a rule,
decreases in the case of a disease. This tendency makes
many researchers regard Se deficit as an alarm signal in
the development of one or another pathogenesis [26-28].
Even in their first studies some authors attempted to as-
sess the impact of Se on dystrophic processes in muscle
tissue [29]. They have found out that Se concentration in
blood decreases, as myotic dystrophy develops. How-
ever, we have failed to find the works which would ex-
plain what is happening to Se concentration in humans
with a different functional state of muscle tissue.
Unfortunately, in our study we were also unable to
evaluate the contribution of Se to the development of
functional dysfunction of LV myocardium in the process
of CHF progression due to the absence of a clear rela-
tionship of this element content with EF (r = 0.23; p >
0.05). It can be only noted that no statistically significant
differences in Se content in the myocardium of CHD
patients and the control group have been revealed (0.78 ±
0.067 и 0.96 ± 0.056 µg/g of tissue respectively). In lit-
erature it is suggested that selenium is very much the
same as sulphur. At the same time in living organisms
these two elements behave in a completely different way.
Specifically, in animals Se compounds tend to regenerate,
while S compounds are subject to oxidation. Selenium is
capable of repairing disulfide links in proteins in SH
groups.
We have also found out that there exists a statistically
significant correlation relationship of Se content with
Mn (r = 0.34; p < 0.05) and with Zn (r = 0.44; p < 0.01),
as well as with Rb (r = – 0.45: p < 0.01) and Sr (r = 0.40;
p < 0.05), which may be explained by free radical oxida-
tion.
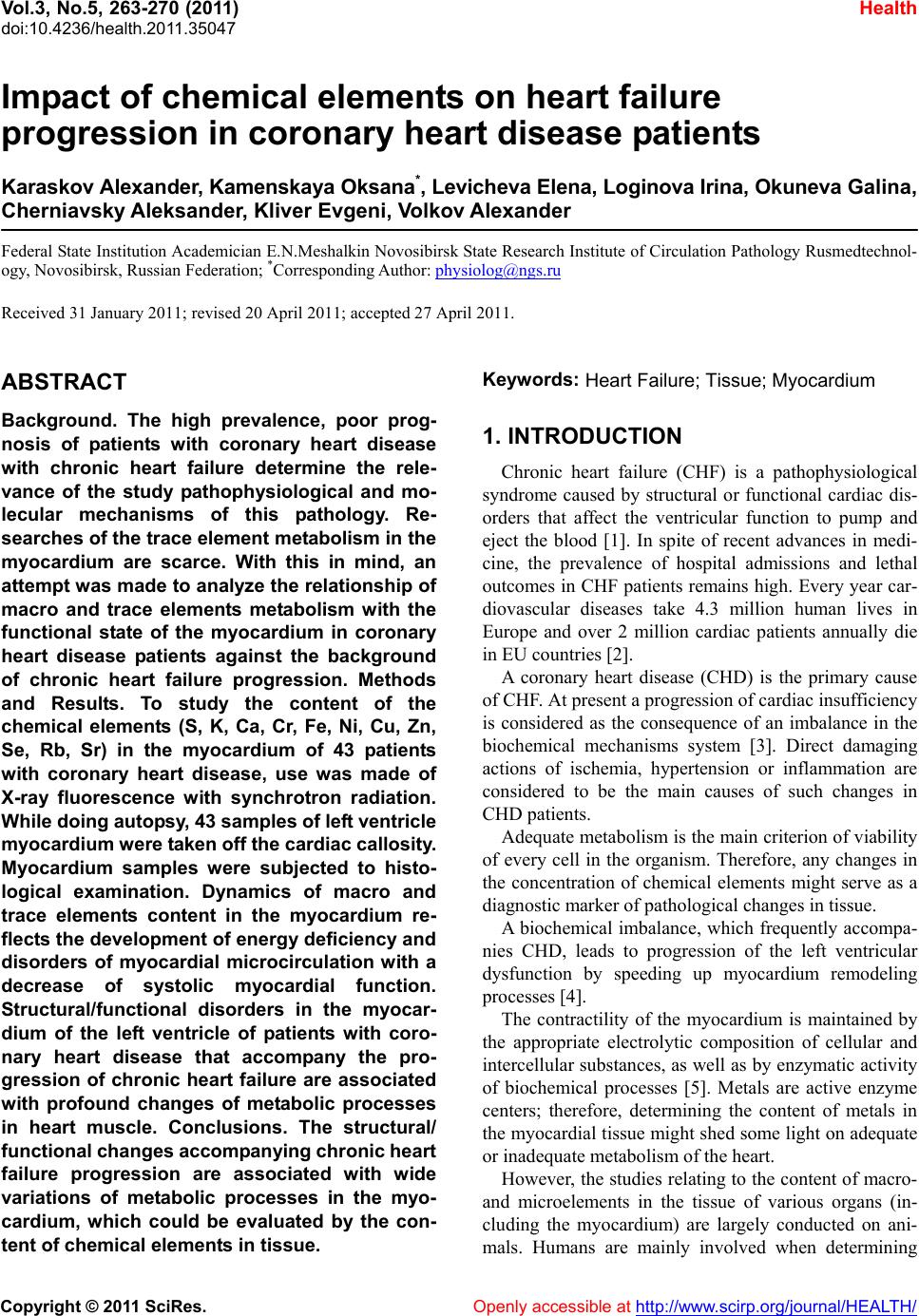
Thus, the structural/functional changes accompanying
CHF progression are associated with wide variations of
metabolic processes in the myocardium, which could be
evaluated by the content of chemical elements in tissue.
With clinical data on the severity of heart failure, we can
assume the status of metabolic processes in the myocar-
dium. Study results on the contents of chemical elements
in the myocardium during CHF progression is a funda-
mental basis for drug development and new approaches
in the therapy of heart failure. The results obtained
demonstrate that in order to understand the pathogenesis
of cardiac insufficiency progression, we need further
research in this direction.
REFERENCES
[1] Focused Update (2009) ACCF/AHA guidelines for the
diagnosis and management of heart failure in adults: A
report of the American College of Cardiology Founda-
tion/American Heart Association Task Force on practice
guidelines: Developed in collaboration with the Interna-
tional Society for Heart and Lung Transplantation. Cir-
culation, 11 9, 1977-2016.
[2] Ratmanova, A. (2009) Cardiovascular morbidity and
lethality statistics in European countries (2008). Medi-
cine Review, 1, 6-12.
[3] Sato, Y., Kita, T., Takatsu, Y. and Kimura, T. (2004) Bio-
chemical markers of myocyte injury in heart failure.
Heart, 90, 1110-1113. doi:10.1136/hrt.2003.023895
[4] St. John Sutton, M.G. and Sharpe, N. (2000) Left ven-
tricular remodeling after myocardial infarction. Circula-
tion, 101, 2981-2988.
[5] Kassiri, Z., Zhong, J., Guo, D., et al. (2009) Loss of an-
giotensin-converting enzyme 2 accelerates maladaptive
left ventricular remodeling in response to myocardial in-
farction. Circulation: Heart Failure, 2, 446-455.
doi:10.1161/CIRCHEARTFAILURE.108.840124
[6] Rashed, M.N., Ahmed, M.M., Al-Hossainy, A.F. and Abd,
S.M. (2010) Trends in speciation analysis of some heavy
metals in serum of patients with chronic hepatitis C and
chronic hepatitis B using differential pulse adsorptive
stripping voltammetric measurement and atomic absorp-
tion spectrophotometry. Journal of Trace Elements in
Medicine and Biology, 24, 138-145.
doi:10.1016/j.jtemb.2009.11.006
[7] Siddiqui, M.K.J., Jyoti, S., Mehrotra, P.K., Singh, K. and
Sarangi, R. (2006) Comparison of some trace elements
concentration in blood, tumor free breast and tumor tis-
sues of women with benign and malignant breast lesions:
An Indian study. Environment International, 32, 630-637.
doi:10.1016/j.envint.2006.02.002
[8] Miner, E.C. and Miller, W.L. (2006) A looc between the
cardiomyocytes: The extracellular matrix in heart failure.
Mayo Clinic Proceedings, 81, 71-76. doi:10.4065/81.1.71
[9] ASSC/SECI (2010) National recommendations on diag-
nostics and treatment of CHF (3rd revision). Heart Fail-
ure, 55, 3-62.
[10] Zile, M.R. and Brutsaert, D.L. (2002) New concepts in
diastolic dysfunction and diastolic heart failure: Part I
diagnosis, prognosis, and measurements of diastolic
function. Circulation, 105, 1387-1393.
doi:10.1161/hc1102.105289
[11] Ramani, G.V., Uber, P.A. and Mehra, M.R. (2010)
Chronic heart failure: Contemporary diagnosis and man-
agement. Mayo Clinic Proceedings, 85, 180-195.
doi:10.4065/mcp.2009.0494
[12] Beltrami, C.A., Finato, N., Rocco, M., Feruglio, G.A., et
al. (1994) Structural basis of endstage failure in ischemic
cardiomyoparthy in humans. Circulation, 89, 151-163.
[13] Novelli, E.L.B., Diniz, Y.S., Machado, T., Proen, B., et al.
(2000) Toxic mechanism of nickel exposure on cardiac