J. Y. LI ET AL.
142
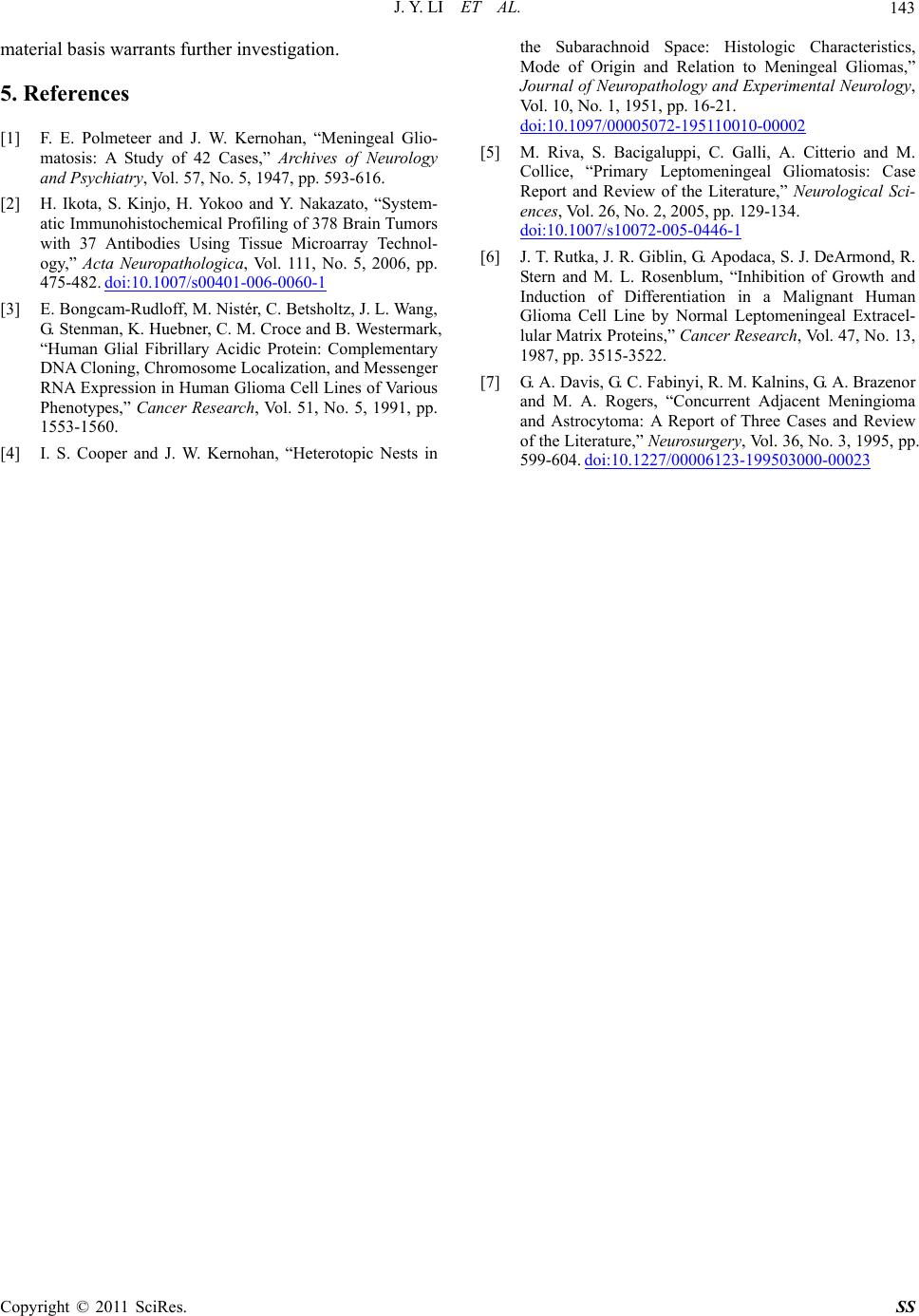
were active in growth and accompanied with abundant
vascular proliferation and extensive tissue necrosis. All
of these indicated glioma (Figure 2(a)). The immuno-
histochemical staining showed epithelial membrane an-
tigen (EMA) negative, GFAP positive (Figures 2(b) and
(c)). However, the inferior part of the tumor was outside
the cerebrum and based at the bottom of the middle fossa.
Microscopically, this part composed of spindle cells ar-
ranged in whorl patterns. The cells grew slowly and
mildly with no karyokinesis. These were characteristics
of meningioma (Figure 2(d)) with EMA positive (Fig-
ure 2(e)) and GFAP positive (Figure 2(f)) of immuno-
histochemical staining. The patient recovered well after
operation, under advice of radiotherapy and chemother-
apy.
3. Discussion
In this case, we found the inferior part, extracerebral
smooth, tough, and firm tumor, which located in the bot-
tom of the middle cranial fossa, had defined and clear
border to the intracerebral upper part tumor. Pathological
findings indicated that the upper part tumor exhibits
morphological characteristics of glioma, as well as
GFAP positive and EMA negative. Meanwhile, inferior
part tumor reflect the morphing characteristic of men-
inges, but its immunohistochemical staining shows
GFAP positive, and EMA positive appeared in cells ar-
ranging in whorl patterns. EMA is specific marker for
normal epithelium or epithelial origin tumor which ex-
pressed in most meningioma, but usually negative in
glioma cells [2]. As a kind of intermediate filaments in
gliocyte, GFAP expressed in most astrocytoma and was
considered as the major evidence for diagnosing glioma
[2,3]. In our case, the inferior part tumor exhibits the
basement of meninges and there was a clear boundary
with the upper part tumor even though they were in one
solid mass in MRI. Positive of EMA indicated that tumor
cells of the inferior part originated from meningothelium,
and positive of GFAP indicated its features of glioma.
We think the term “meningioma-glioma” was more suit-
able than “meningeal glioma” for our case.
Our meningioma-glioma case is different from previ-
ously reported cases of meningeal gliomatosis. The latter
concerned with tumor-like lesions in meninges of the
brain or the spinal cord or the ependyma of the ventricu-
lar system caused by metastatic implantations from in-
tracerebral glioma. Those metastatic glioma cells estab-
lished themselves in multiple sites via CSF system,
caused clinical manifestation like meningitis, and usu ally,
there’re no differences in cell characteristics between
meningeal gliomatosis and intracerebral gliomas [4,5].
Moreover, previous researches showed that glioma cells
which were cultured in normal leptomeningeal extracel-
lular matrix proteins still kept the features of gliocytes
[6]. This suggested th at if glioma cells in vaded mening es
directly and proliferated, their features won’t be changed
by extracellular environment of meningocytes. To our
meningioma-glioma case, it is not only there was a
boundary between the su perior an d infer ior parts but also
the cells of the meningeal glioma possess features like
meningioma cell rather than glioma cell, and immuno-
histochemical staining showed EMA positive. These
indicated that this inferior part tumor was not an invaded
or implanted tumor of intracerebral glioma cells but was
a tumor originated from the meningocytes.
Cooper and Kernohan ha d suggested that primary lep-
tomeningeal glioma originated from dedifferentiation of
heterotopic glial nests [4]. This suggestion seemed un-
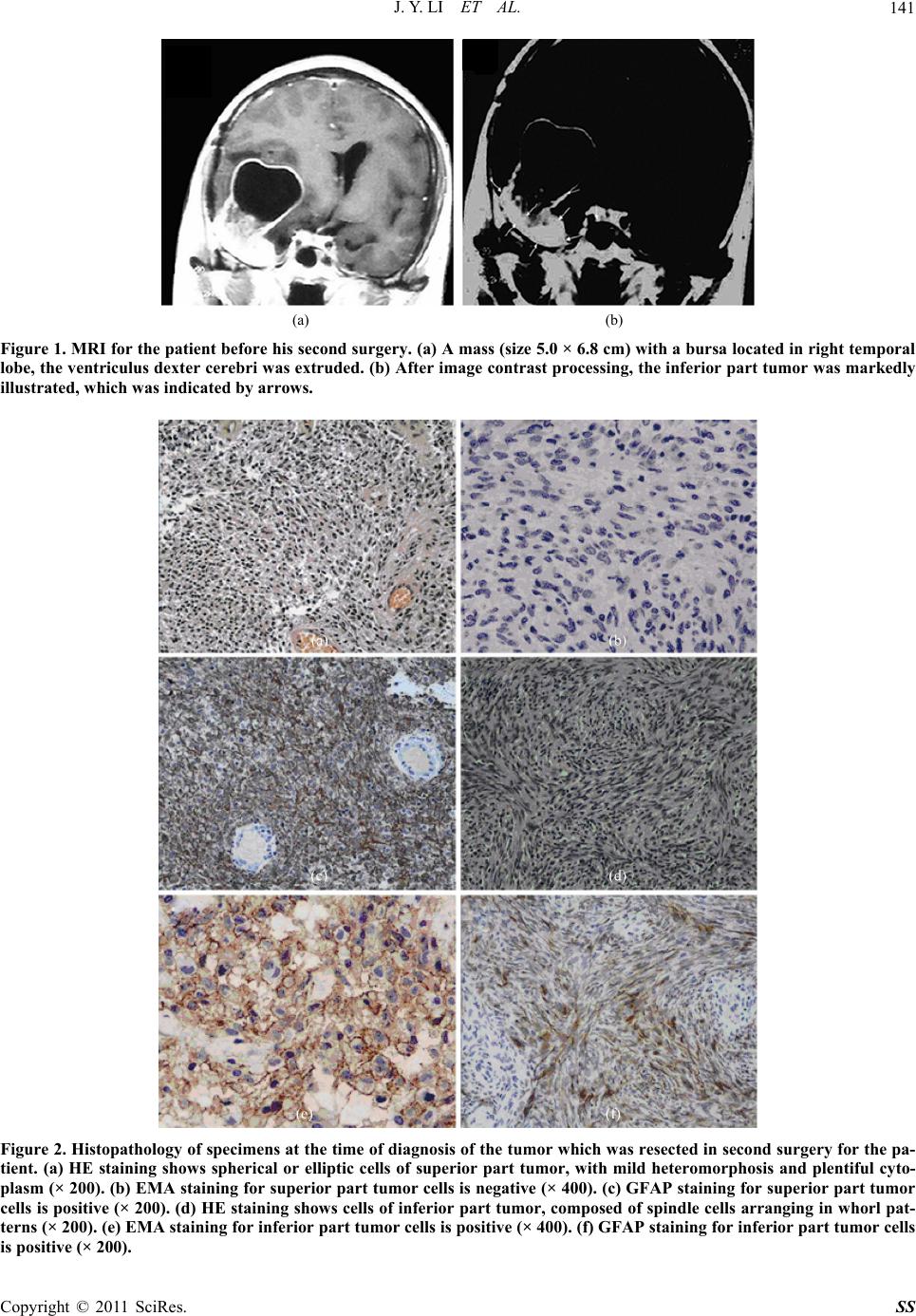
suitable for our case, since the tumor divided into two
parts (Figure 1) in one solid mass, the inferior men-
ingeal glioma tight conjuncted the superior glioma. And
there’s no neoplasm in meninges in first surgery for
glioma. We presumed that the recurrence malignant
glioma stimulated the adjacent meninges into neoplastic
proliferation, altho ugh ther e is n o more knowledg e about
the biomechanism or material basis relate to this irritant
action. For our case, this hypothesis seemed more rea-
sonable than “leptomeningeal gliomas originated from
dedifferentiation of heterotopic glial nests” [4]. Davis
had given similar hypothesis after their research of con-
current meningioma and astrocytoma growth [7]. They
considered that meningioma or glioma can stimulate the
adjacent brain parenchyma or arachnoid cells into neo-
plastic proliferation. To our case, we consider that the
irritant action from the malignant glioma not only caused
neoplastic proliferation of meninges but also changed
their phenotypes into expressing both EMA and GFAP.
Further more works are needed to demonstrate the bio-
mechanism and material basis relate to this kind of irri-
tant action.
4. Conclusions
Pathological examinations are necessary for men-
ingioma-glioma mixed tumor diagnosis. Specific immu-
nohistochemical staining should be an important deter-
mination in differential diagnosis and could help confirm
tumor histic origins. This rare tumor which we reported
was recurrent and had meningeal neoplastic proliferation
to primary tumor lesions and was considered as single
and unitary tumor in MRI scans and intraoperative find-
ings. Further pathological studies were necessary to re-
veal the tumor’s real characteristics. Our case demon-
strated that glioma may stimulate adjacent meninges into
neoplastic proliferation, but related biomechanism and
C
opyright © 2011 SciRes. SS