S. SERELS
23
sobturator, by contrast, avoids the retropubic space,
decreasing complications such as bladder and bowel
s being different than the retropu-
bi
ferent than the other c
m
ten-
si
experience. Taken together, these data seem to initially
dispel some of the previously held misconceptions of
d the single-incision sling as tensioned
m
. Lose, D. Sykes, et al., “The Prevalence
continence in Women in Four European
he British Association of Urological
93, 2004, pp. 324-330.
ternational Urogynecology Journal and
injuries and is as efficacious as the retropubic method
with a reduction in adverse events [8-10]. Single inci-
sion slings provide the latest advance in midurethral
tensionless sling technology and require only one small
vaginal incision placed beneath the urethra thereby po-
tentially reducing post-operative pain and risk of com-
plications. However, minimal data are currently avail-
able on the long-term efficacy and safety of the sin-
gle-incision method.
Our ex per ie nce h as b een tha t most physicians view the
single incision sling a
c or transobturator slings. Furthermore, physicians of-
ten describe the single-incision as a “tight” sling. This
association of “tight” with the single-incision sling is
based primarily on perceived placement methodology,
and not on actual tensioning tests. For example, the ten-
sion of the single-incision sling is achieved by pushing
the sling into tissue rather than pulling up on it as is do ne
for the retropubic and transobturator slings. When the
coverings are taken off and any spacing devices are re-
moved from the multi-incision slings, there is further
retraction that occurs. Thus, the initial placement of the
multi-incision sling changes and the sling tightens a
small amount. In contrast, placement of the single inci-
sion sling does not change, and the site of the sling dur-
ing tensioning is where it remains. As a result, the sin-
gle-incision sling may seem slightly tighter on initial
placement, but appears the same as the others when the
sling is in its final position.
The purpose of this study was to determine if the sin-
gle-incision sling looks difom-
only used retropubic and obturator slings, and to de-
termine which of the three slings was identified by
trained physicians as being most correctly tensioned at
the mid urethra. The results showed that well-trained,
experienced incontinence surgeons could not visually
differentiate between sling placement methodologies.
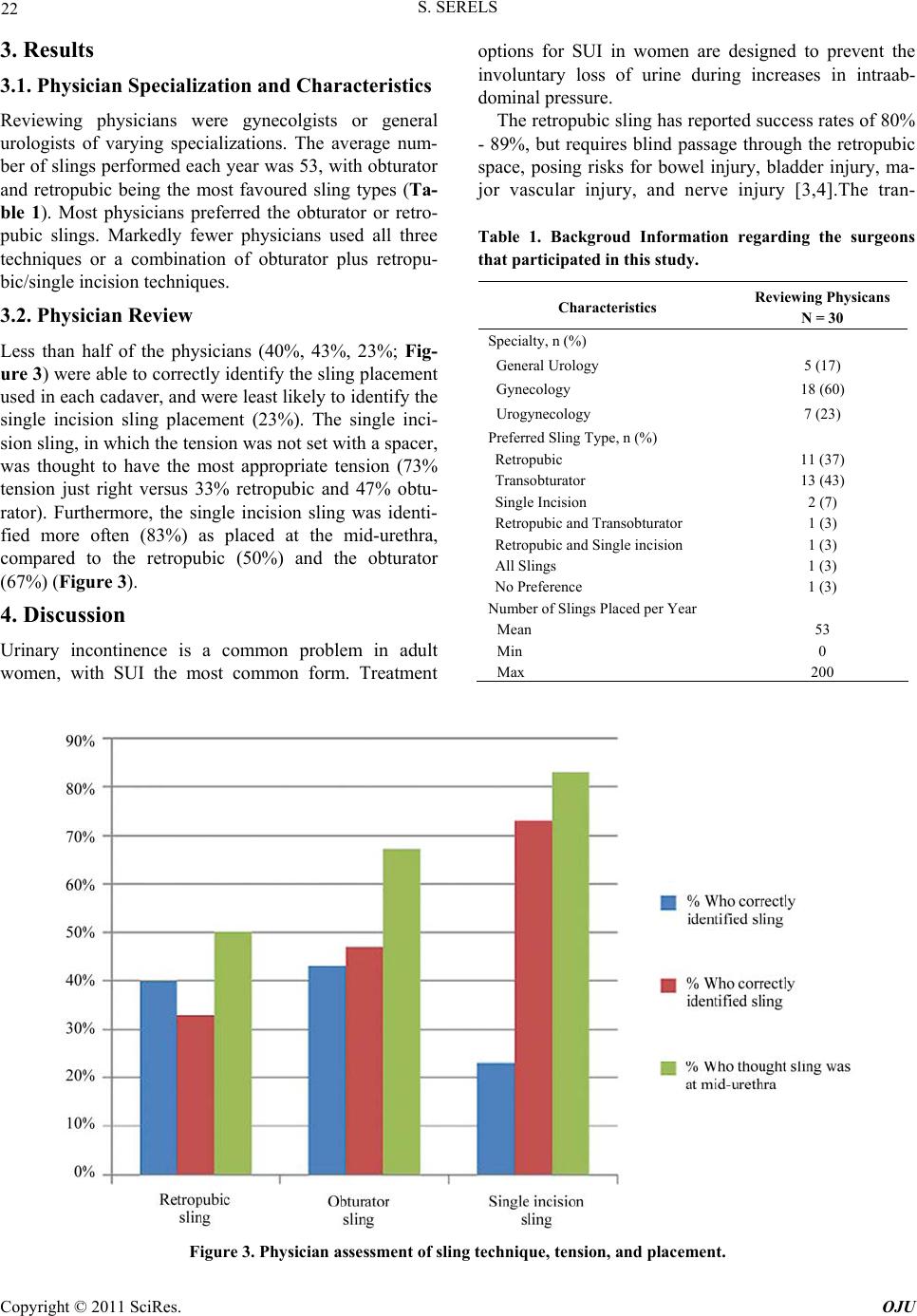
Less than half of the physicians (40%, 43%, 23%) were
able to correctly identify the sling placement used, and
were least likely to be able to identify a single-incision
sling placement (23% correctly identified).
Furthermore, the results showed that the single inci-
sion sling was identified as having the most correct
on (73% tension just right versus 33% retropubic and
47% obturator) and the most correct mid-urethral posi-
tioning (83% versus 50%retropubic and 67% obturator).
Of note, 6 physicians who were highly experienced in
sling placement (> 100 procedures/year each). There
were no clear trends in the ability to appropriately iden-
tify the sling placement method used based on physician
how a single-incision sling differs from multi-incision
sling procedures and indicate that the biases toward the
single incision sling typically voiced by practicing phy-
sicians seem to be rooted in preconceived misconcep-
tions and not on actual results, regardless of experience
or specialty.
Conclusions: This study showed that after placement
of a midurethral synthetic sling it is difficult to deter-
mine the placement method used and that most physi-
cians assesse
ost appropriately and most likely positioned at the
mid-urethra.
5. Acknowledgements
This study was supported by an unrestricted grant from
Boston Scientific.
6. References
[1] S. Hunskaar, G
of Urinary In
Countries,” Journal of t
Surgeons, Vol.
[2] P.E Petros and U. Ulmsten, “An Integral Theory of
Female Urinary Incontinence,” Acta Obstetricia et
Gynecologica Scandinavica, Supplement 153, Vol. 69,
1990, pp. 7-31.
[3] C. G. Nilsson, N. Kuuva, C. Falconer, et al., “Long-Term
Results of the Tension-Free Vaginal Tape (TVT)
Pr oc ed ur e for Surgical Treatme nt of Female Stress Urinary
Incontinence,” In
Pelvic Floor Dysfunction, Supplement 2, Vol. 12, 2001,
pp. S5-S8. doi:10.1007/s001920170003
[4] K. L. Ward and P. Hilton, “UK and Ireland TVT Trial
Group. Tension-Free Vaginal Tape Versus Colposuspension
for Primary Urodynamic Stress Incontinence: 5-Year
Follow Up,” BJOG, Vol. 115, No. 2, 2008, pp. 226-233.
doi:10.1111/j.1471-0528.2007.01548.x
[5] V. W. Sung, M. D. Schleinitz, C. R. Rardin, et al.,
“Com parison of Retropubic versus Transobturator Approach
to Midurethral Slings: A Systematic Review and Meta-
Analysis,” American Journal of
Obstetrics and
Gynecology, Vol. 197, No. 1, 2007, pp. 3-11.
doi:10.1016/j.ajog.2006.09.025
[6] A. C. Wang, “The Techniques of Trocar Insertion and
Intraoperative Urethrocystoscopy in Tension-Free
Vaginal Taping: An Experience of 600 Ca
Obstetricia et Gynecologica Scases,” Acta
ndinavica, Vol. 83, No. 3,
6-1313.
2004, pp. 293-298.
[7] E. Delorme, “Transobturator Urethral Suspension: Mini-
Invasive Procedure in the Treatment of Stress Urinary
Incontinence in Women [in French],” Prog Urol, Vol. 11,
No. 6, 2001, pp. 130
Copyright © 2011 SciRes. OJU