 Open Journal of Psychiatry, 2011, 1, 1-7 doi:10.4236/ojpsych.2011.11001 Published Online April 2011 (http://www.SciRP.org/journal/OJPsych/ OJPscyh ). Published Online April 2011 in SciRes. http://www.scirp.org/journal/OJPsych Increased breath ethane and pentane concentrations in currently unmedicated patients with schizophrenia Brian M. Ross1, Sandeep Shah2, Malcolm Peet3 1Northern Ontario School of Medicine, Thunder Bay, Ontario, Canada; 2Sumandeep Vidyapeeth, AT&PO: Piparia, Vadodara, India; 3University of Sheffield, Sheffield, United Kingdom. Email: brian.ross@nosm.ca Received 19 March 2011; revised 21 April 2011; accepted 28 April 2011. ABSTRACT Schizophrenia is a common and debilitating mental illness. The disorder is thought to be developmental in origin, with oxidative stress being implicated as possible pathophysiological mechanism. Breath al- kanes provide a non-invasive means to assess oxida- tive stress, with ethane levels reportedly increased in medicated patients with schizophrenia. It is possible, however, that the psychotropic medications used to treat the disorder result in elevated breath ethane levels. We have therefore measured the con centra tion of ethane and pentane, markers of oxidative stress, in the breath of currently unmedicated patients with schizophrenia. Alveolar breath samples were col- lected, applied to thermal desorption tubes, and ana- lyzed using a combination of two-stage thermal de- sorption, gas chromatography and mass spectrome- try. Compared to healthy controls ethane and pen- tane levels were found to be elevated in patients with schizophrenia, while levels of butane were normal. Our data support the notion that oxidative stress is increased in schizophrenia and that this is unlikely to be a consequence of antipsychotic medications. In addition, breath alkane analysis may represent a rapid and non-invasive means to monitor oxidative stress occurring in schizophrenia. Keywords: Breath Analysis; Alkane, Schizophrenia; Ethane; Pentane 1. INTRODUCTION Schizophrenia is a serious mental illness which first presents in late adolescence or early adulthood. [1] The disorder, which affects approximately 1% of the popu- lation, is characterized by a range of symptoms includ- ing delusions, hallucinations, disordered thoughts and avolition. [1,2] Current treatments have limited efficacy in many patients, with the development of more effec- tive therapies being hampered by a lack of understanding of the pathophysiological mechanism (s) at work. [1] An emerging hypothesis states that disordered oxidative metabolism leads to the brain dysfunction which underl- ies the disorder. [3] This process, termed oxidative stress, comprises the reactions between metabolically generated free radicals (highly reactive molecules possessing un- paired electrons) and cellular constituents such as DNA, lipids and proteins. [4] The reactions are generally dele- terious, leading to a loss of, or altered, function of the cell which, if severe enough, can result in cell death. [4] To combat this process cells possess various antioxidant defenses the purpose of which is to detoxify free radicals. These defenses include enzymes, such as superoxide dismutase, glutathione peroxidase and catalase, and an- tioxidant compounds, such as vitamin E, which prefer- entially react with free radicals hence preserving other cellular constituents. [4] As such the degree of oxidative stress a cell experiences is determined by the balance between oxidative and anti-oxidative factors. In schizophrenia, a number of lines of evidence have suggested that oxidative stress is abnormal [3,5,6]. Since direct measurement of the short lived and reactive free radicals is extremely difficult, most information regard- ing oxidative stress in schizophrenia derives from the assay of specific components of the anti-oxidant system and/or measurement of the chemical products of oxida- tive damage. While generally supportive, when exami- ned in detail the findings are somewhat inconsistent. For example, peripheral superoxide dismutase activity, an enzyme which detoxifies superoxide radicals, is reported to be either decreased, increased or unchanged, with similar variability of results being reported for catalase and glutathione peroxidise. [3,5-13] It is notable, howe- ver, that when the system is considered as a whole, using methods which assess total antioxidant capacity, a consi- stent reduction in antioxidant activity in schizophrenia  B. M. Ross et al. / Open Journal of Psychiatry 1 (2011) 1-7 2 emerges, indicating an overall elevated susceptibility to free radical damage in the disorder. [14-16] This is sup- ported by several reports of increased levels of DNA, protein and lipid oxidation products in patients with schizophrenia. [17-21] Moreover, the use of an animal model of oxidative stress has indicated that free radical over-activity effects brain development and function, supporting the biological plausibility of oxidative stress playing a role in the disease. [22,23] As such, monitoring oxidative stress in patients may have some clinical utility. Relating the normally utilised peripheral measures of oxidative stress to that in the brain is challenging however, although evidence of oxi- dative damage has been detected post mortem in the cortex and hippocampus of patients with schizophrenia. [17,18,21] A recent study has correlated an index of sys- temic oxidative stress with changes in brain metabolism investigated using in vivo 31P magnetic resonance spec- troscopy. [24] The marker utilised was ethane, a terminal product of the oxidation of omega-3 polyunsaturated fatty acids [4], which has been shown to be elevated in schizophrenia in two previous studies [25,26], a finding supportive of the occurrence of increased oxidative stress. The other class of polyunsaturated fatty acids, omega-6 fatty acids, also give rise to an alkane oxidation product which differs from that of omega-3 fatty acids, this being pentane [4]. A generalised increase in oxidative stress in schizophrenia would predict that breath concentrations of pentane should be increased although the status of this compound in schizophrenia is currently unknown. Since ethane and pentane are both highly volatile they have the useful feature of equilibrating rapidly into the blood- stream, and subsequently crossing the alveolar mem- brane to be exhaled in the breath where they can be de- tected using a variety of analytical approaches including gas chromatography and various forms of chemical ioni- sation mass spectrometry. [27-29] So-called breath ana- lysis is an emerging methodology which, being non- invasive and rapid, is ideally suited to clinical monitor- ing. [30] Given the correlation of breath ethane with brain metabolism [24], measuring the breath concentra- tion of this compound may represent a useful means to examine oxidative stress in schizophrenia. Studies util- ising breath ethane in schizophrenia should be consid- ered preliminary, however, since only medicated patients with the disorder have been included. Indeed, recent reports have highlighted that pharmaceuticals can alter the chemical makeup of breath, and in fact can give rise to volatile metabolites raising the possibility that ethane may derive directly from such medications. [31,32] In addition, some antipsychotic medications, in particular clozapine and haloperidol, may actually cause increased oxidative stress [33-36], an effect which could again result in altered breath ethane abundance. As such, it presently cannot be ruled out that elevated breath ethane in schizophrenia is due to medication. In this paper we have therefore investigated breath concentrations of both ethane and pentane, as well as butane as a comparator, in a currently un-medicated population of patients with schizophrenia. 2. METHODS 2.1. Participants Subjects were recruited by invitation having given writ- ten informed consent under a protocol approved by the institutional ethics committee. Patients with schizophre- nia all had a clinical diagnosis of schizophrenia (n = 28) according to DSM-IV criteria. [37] Patients had not been in receipt of psychotropic medication for three weeks prior to participating in the study but had received me- dication prior to that (no patients were withdrawn from their medication for the purpose of this study; rather non-compliance with treatment had occurred). Healthy controls (n = 15) had neither history of mental illness nor any medicinal intake of any kind for the previous two weeks, and had no history of any psychotropic drug intake. Almost all subjects were smokers with only four non-smokers in the schizophrenia group and two in the healthy control group with the rate of smoking not dif- fering between groups (χ2 test; P > 0.05). No subject had smoked within the 2 hours prior to breath collection. No subjects had any potentially confounding medical illness. The age of patients with schizophrenia (33 6 years [mean sd]) did not differ significantly (two-tailed, un- paired t-test; P > 0.05) from that of the healthy control group (34 7 years). In addition the proportion of males to females in each group (15 females/13 males in the schizophrenia group vs. 8 males/7 females in the healthy control group) did not differ significantly (χ2 test; P > 0.05). 2.2. Breath Sampling Seated subjects were asked to breathe normally for 3 breaths and then exhale fully into a collection bag con- structed in our laboratory. The collection bag was made from PTFE with dimensions of approximately 10 cm × 15 cm and a volume of approximately 200 ml. The bag had both an inlet and outlet, with air from the inlet en- tering the bag via a unidirectional flow valve, while the outlet tube had a constricting clip attached with which the bag could be sealed. As the subject exhaled the bag inflated and breath passed through the bag to the outlet. When the subject had exhaled fully the bag therefore contained the final 200 ml of exhaled ‘alveolar’ breath. A similar collection method was also used for ambient air samples except that a syringe was used to inflate the bag. C opyright © 2011 SciRes. OJPsych  B. M. Ross et al. / Open Journal of Psychiatry 1 (2011) 1-7 3 2.3. Alkane Analysis Alkane analysis was performed as previously described with minor modifications. [24-26,29] The collection bag was connected via the outlet to a 130 ml PTFE syringe and a volume of gas removed. The syringe was then used to apply the gas sample to a thermodesorption tube (Markes Instruments, UK) containing Carbotrap 300 (Markes Instruments, UK), prior to analysis using Perkin- Elmer autosystem XL equipped with a Turbomass mass spectrometer (Perkin-Elmer, UK). The absorbed gases were desorbed at 320˚C onto a cold trap held at 5˚C. Secondary desorption at 350˚C released the volatiles into a 2 ml min-1 stream of helium onto a 30 m × 0.32 mm PLOT GQ column. The initial GC oven temperature of 45˚C was maintained for 10 min and increased at 200˚C at a rate of 14˚C min−1. Eluted gases were detected by electron ionisation mass spectrometry with ethane eluting at 2.6 min, butane at 9.6 min and pentane at 12.1 min, and quantified by comparison with a standard curve constructed using a C1-C6 alkane mix (Supelco, UK). 3. RESULTS Breath samples were collected from 28 patients with schizophrenia who have received no psychoactive medi- cations for at 2 - 3 weeks prior to sampling, and from 15 healthy controls, and assayed for ethane, butane and pentane. As is observed for other trace gases in breath [38,39], and for breath alkanes in our previous study [26], ethane, butane and pentane concentrations followed an apparent log normal distribution (Lilliefors test for normality of log transformed data; P > 0.05 for all groups). Due to this finding the log of the concentration was used in the statistical analysis of the data. Ethane and pentane concentrations were elevated in the breath of patients with schizophrenia compared to healthy con- trols (two-tailed, unpaired t-test; P < 0.01). Butane con- centrations did not differ significantly between the two groups (two-tailed, unpaired t-test; P > 0.05). Gender had no statistically significant effect upon the concentra- tions of either gas (two-tailed, unpaired t-test; P > 0.05). Age did not correlate significantly (P > 0.05) with con- centrations of each alkane (data not shown). Butane concentrations did not correlate significantly (P < 0.05) with ethane or pentane concentrations in either the schizophrenia (Figure 2) or healthy control groups (Pearson correlation coefficient = 0.06), but ethane con- centrations were correlated with pentane concentrations in the schizophrenia group (Pearson correlation coeffi- cient = 0.59; P < 0.001) but not in the healthy control group (Pearson correlation coefficient = 0.10; P > 0.05). Ambient alkane concentrations were below 1 PPBV for each gas, close to the limits of detection of the assay (approx. 0.1 PPBV), and did not differ significantly be- tween the schizophrenia and healthy control groups (t-test; P < 0.05). 4. DISCUSSION Our findings confirm previous reports [25,26] of ele- vated breath ethane concentrations in patients with schizophrenia in a different population indicating ele- vated oxidative damage to omega-3 PUFA. The breath concentrations observed are similar to that found in our previous investigation of schizophrenia [25,26,29], and for healthy controls are similar to that reported by other investigators. [40] In addition, we have also observed increased breath pentane concentrations in the breath of patients with schizophrenia, suggesting that omega-6 PUFA are similarly affected. A common mechanism un- derlying increased breath ethane and pentane, that of oxidative damage of PUFA, is supported by the correla- tion between the abundance of each alkane in the schizophrenia group (no significant correlation was ob- served in the healthy control group but this may be due to the rather low breath alkane concentrations <1 PPB being closer to the limits of detection for the assay). In- deed, reduced levels of PUFA have been reported to oc- cur in schizophrenia (for example see reference 41), an observation which may be due to elevated oxidative damage of these fatty acids in the disorder. On the other hand, ethane concentrations are not reported to be corre- lated with erythrocyte omega-3 PUFA abundance in Figure 1. Breath concentrations of ethane, pentane and butane were measured in patients with schizophrenia (SCZ) and healthy controls (HC). Note the logarithmic scale of the Y-axis. The bar indicates the median value. SCZ and HC groups were compared using an unpaired t-test with *indicating P < 0.01. PPBV – parts per billion by volume. C opyright © 2011 SciRes. OJPsych  B. M. Ross et al. / Open Journal of Psychiatry 1 (2011) 1-7 4 (a) (b) Figure 2. Correlation between alkane concentrations in breath in patients with schizophrenia. The log breath concentrations of (a) pentane or (b) butane are shown plotted against the log concentration of ethane in parts per billion by volume (PPBV). The dashed line shows the ‘best fit’ linear regression line along with the Pearson correlation coefficient with *indicating P < 0.001. medicated patients [26]. This suggests that other factors, such as dietary intake, may also underlie reduced fatty acid levels in addition to elevated oxidative stress [42] and that there is not a simple relationship between breath alkane concentrations and the abundance of their pre- cursor lipids. The magnitude of the increase in breath alkane con- centrations is similar to that observed in medicated pa- tients [26], even though our participants were unmedi- cated for at least 3 weeks prior to breath sampling. As such, increased breath ethane and pentane concentrations are likely not derived directly from any administered drugs, although we cannot rule out a longer term effect of any drug upon cellular metabolism given that the par- ticipants were not drug-naïve. Such findings are in agreement with data obtained using other experimental approaches which also suggest that psychoactive medi- cation is not an important mediator of oxidative stress in patients. [8,43] It is important to note that breath butane concentra- tions were normal in schizophrenia, and found to be un- correlated with ethane or pentane concentrations. We had previously observed increased breath butane con- centrations in schizophrenia, but reasoned that this find- ing was due to elevated ambient butane abundance in the sampling room used for patients, leading us to conclude that breath butane has an exogenous source. [26] How- ever, ambient butane concentrations were very low in the current study (< 1 PPBV) and breath butane concentra- tions were routinely above ambient. This does suggest a possible endogenous source for butane, as revealed by low ambient gas concentrations, although the mecha- nism leading to its production is presently unknown. Interestingly, in vitro chemical oxidation of erythrocytes does give rise to butane production although the chemi- cal source is unknown [44-46]. Nevertheless, the lack of correlation with butane, as well as reports that ambient C1 - C4 alkane concentrations are correlated in polluted environmental air [47], is supportive of breath ethane and pentane are predominantly endogenous metabolic products (at least when sampled in the absence of sig- nificant alkane air pollution as in the current investiga- tion). Notably, breath alkane concentrations were found to follow a log normal distribution, similar to that ob- served for other breath gases. [38,39] Most of our subjects were smokers, the rate of which did not differ between the schizophrenia and control groups in this Indian sample. Such a finding differs from that in Western nations but is consistent with a previous report of cigarette use in this country [48]. The lack of a differential smoking rate between the two groups is an important consideration since there reports that smoking increases breath ethane levels although this is not a con- sistent finding [49,50]. We did not, however, assess the number of cigarettes smoked per day and hence cannot rule out that the schizophrenia group had a higher expo- sure to tobacco product use than the control group. We have previously reported, however, that there is no cor- relation between tobacco exposure and ethane concen- trations in patients with schizophrenia [26], which sup- ports our conclusion that increased breath alkane con- centrations in schizophrenia are consequent to a meta- bolic change associated with the illness. C opyright © 2011 SciRes. OJPsych 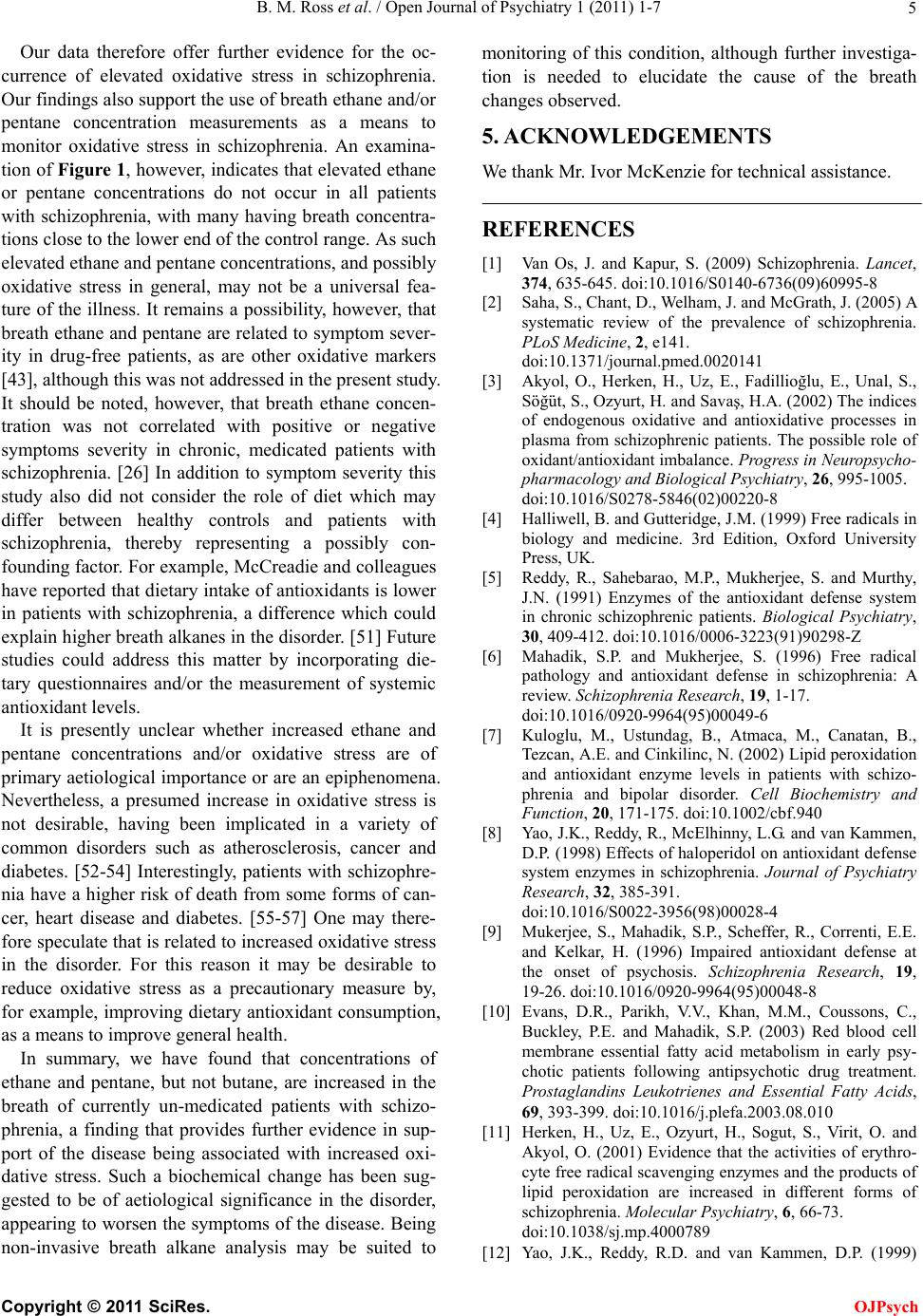 B. M. Ross et al. / Open Journal of Psychiatry 1 (2011) 1-7 5 Our data therefore offer further evidence for the oc- currence of elevated oxidative stress in schizophrenia. Our findings also support the use of breath ethane and/or pentane concentration measurements as a means to monitor oxidative stress in schizophrenia. An examina- tion of Figure 1, however, indicates that elevated ethane or pentane concentrations do not occur in all patients with schizophrenia, with many having breath concentra- tions close to the lower end of the control range. As such elevated ethane and pentane concentrations, and possibly oxidative stress in general, may not be a universal fea- ture of the illness. It remains a possibility, however, that breath ethane and pentane are related to symptom sever- ity in drug-free patients, as are other oxidative markers [43], although this was not addressed in the present study. It should be noted, however, that breath ethane concen- tration was not correlated with positive or negative symptoms severity in chronic, medicated patients with schizophrenia. [26] In addition to symptom severity this study also did not consider the role of diet which may differ between healthy controls and patients with schizophrenia, thereby representing a possibly con- founding factor. For example, McCreadie and colleagues have reported that dietary intake of antioxidants is lower in patients with schizophrenia, a difference which could explain higher breath alkanes in the disorder. [51] Future studies could address this matter by incorporating die- tary questionnaires and/or the measurement of systemic antioxidant levels. It is presently unclear whether increased ethane and pentane concentrations and/or oxidative stress are of primary aetiological importance or are an epiphenomena. Nevertheless, a presumed increase in oxidative stress is not desirable, having been implicated in a variety of common disorders such as atherosclerosis, cancer and diabetes. [52-54] Interestingly, patients with schizophre- nia have a higher risk of death from some forms of can- cer, heart disease and diabetes. [55-57] One may there- fore speculate that is related to increased oxidative stress in the disorder. For this reason it may be desirable to reduce oxidative stress as a precautionary measure by, for example, improving dietary antioxidant consumption, as a means to improve general health. In summary, we have found that concentrations of ethane and pentane, but not butane, are increased in the breath of currently un-medicated patients with schizo- phrenia, a finding that provides further evidence in sup- port of the disease being associated with increased oxi- dative stress. Such a biochemical change has been sug- gested to be of aetiological significance in the disorder, appearing to worsen the symptoms of the disease. Being non-invasive breath alkane analysis may be suited to monitoring of this condition, although further investiga- tion is needed to elucidate the cause of the breath changes observed. 5. ACKNOWLEDGEMENTS We thank Mr. Ivor McKenzie for technical assistance. REFERENCES [1] Van Os, J. and Kapur, S. (2009) Schizophrenia. Lancet, 374, 635-645. doi:10.1016/S0140-6736(09)60995-8 [2] Saha, S., Chant, D., Welham, J. and McGrath, J. (2005) A systematic review of the prevalence of schizophrenia. PLoS Medicine, 2, e141. doi:10.1371/journal.pmed.0020141 [3] Akyol, O., Herken, H., Uz, E., Fadillioğlu, E., Unal, S., Söğüt, S., Ozyurt, H. and Savaş, H.A. (2002) The indices of endogenous oxidative and antioxidative processes in plasma from schizophrenic patients. The possible role of oxidant/antioxidant imbalance. Progress in Neuropsycho- pharmacology and Biological Psychiatry, 26, 995-1005. doi:10.1016/S0278-5846(02)00220-8 [4] Halliwell, B. and Gutteridge, J.M. (1999) Free radicals in biology and medicine. 3rd Edition, Oxford University Press, UK. [5] Reddy, R., Sahebarao, M.P., Mukherjee, S. and Murthy, J.N. (1991) Enzymes of the antioxidant defense system in chronic schizophrenic patients. Biological Psychiatry, 30, 409-412. doi:10.1016/0006-3223(91)90298-Z [6] Mahadik, S.P. and Mukherjee, S. (1996) Free radical pathology and antioxidant defense in schizophrenia: A review. Schizophrenia Research, 19, 1-17. doi:10.1016/0920-9964(95)00049-6 [7] Kuloglu, M., Ustundag, B., Atmaca, M., Canatan, B., Tezcan, A.E. and Cinkilinc, N. (2002) Lipid peroxidation and antioxidant enzyme levels in patients with schizo- phrenia and bipolar disorder. Cell Biochemistry and Function, 20, 171-175. doi:10.1002/cbf.940 [8] Yao, J.K., Reddy, R., McElhinny, L.G. and van Kammen, D.P. (1998) Effects of haloperidol on antioxidant defense system enzymes in schizophrenia. Journal of Psychiatry Research, 32, 385-391. doi:10.1016/S0022-3956(98)00028-4 [9] Mukerjee, S., Mahadik, S.P., Scheffer, R., Correnti, E.E. and Kelkar, H. (1996) Impaired antioxidant defense at the onset of psychosis. Schizophrenia Research, 19, 19-26. doi:10.1016/0920-9964(95)00048-8 [10] Evans, D.R., Parikh, V.V., Khan, M.M., Coussons, C., Buckley, P.E. and Mahadik, S.P. (2003) Red blood cell membrane essential fatty acid metabolism in early psy- chotic patients following antipsychotic drug treatment. Prostaglandins Leukotrienes and Essential Fatty Acids, 69, 393-399. doi:10.1016/j.plefa.2003.08.010 [11] Herken, H., Uz, E., Ozyurt, H., Sogut, S., Virit, O. and Akyol, O. (2001) Evidence that the activities of erythro- cyte free radical scavenging enzymes and the products of lipid peroxidation are increased in different forms of schizophrenia. Molecular Psychiatry, 6, 66-73. doi:10.1038/sj.mp.4000789 [12] Yao, J.K., Reddy, R.D. and van Kammen, D.P. (1999) C opyright © 2011 SciRes. OJPsych 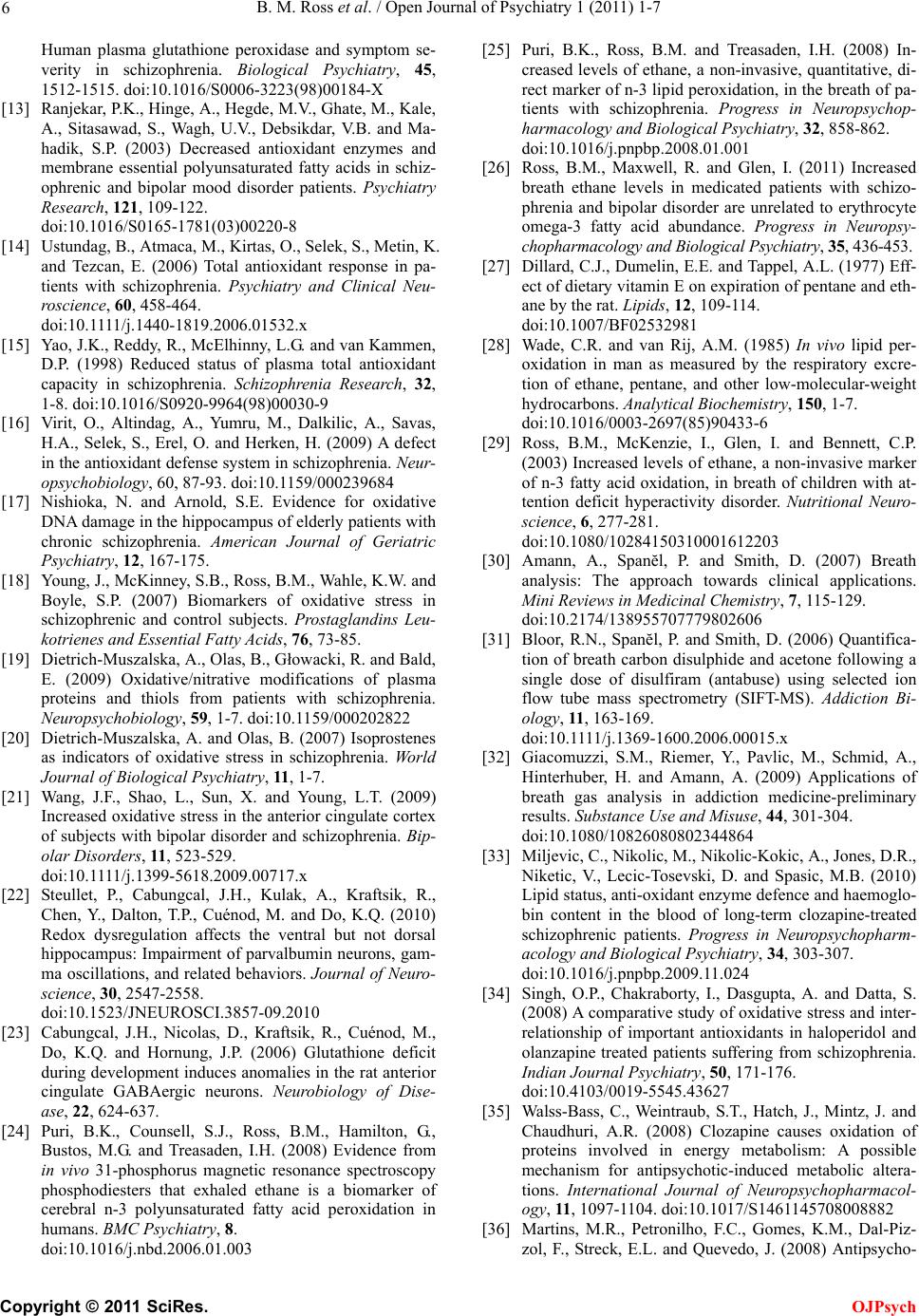 B. M. Ross et al. / Open Journal of Psychiatry 1 (2011) 1-7 6 Human plasma glutathione peroxidase and symptom se- verity in schizophrenia. Biological Psychiatry, 45, 1512-1515. doi:10.1016/S0006-3223(98)00184-X [13] Ranjekar, P.K., Hinge, A., Hegde, M.V., Ghate, M., Kale, A., Sitasawad, S., Wagh, U.V., Debsikdar, V.B. and Ma- hadik, S.P. (2003) Decreased antioxidant enzymes and membrane essential polyunsaturated fatty acids in schiz- ophrenic and bipolar mood disorder patients. Psychiatry Research, 121, 109-122. doi:10.1016/S0165-1781(03)00220-8 [14] Ustundag, B., Atmaca, M., Kirtas, O., Selek, S., Metin, K. and Tezcan, E. (2006) Total antioxidant response in pa- tients with schizophrenia. Psychiatry and Clinical Neu- roscience, 60, 458-464. doi:10.1111/j.1440-1819.2006.01532.x [15] Yao, J.K., Reddy, R., McElhinny, L.G. and van Kammen, D.P. (1998) Reduced status of plasma total antioxidant capacity in schizophrenia. Schizophrenia Research, 32, 1-8. doi:10.1016/S0920-9964(98)00030-9 [16] Virit, O., Altindag, A., Yumru, M., Dalkilic, A., Savas, H.A., Selek, S., Erel, O. and Herken, H. (2009) A defect in the antioxidant defense system in schizophrenia. Neur- opsychobiology, 60, 87-93. doi:10.1159/000239684 [17] Nishioka, N. and Arnold, S.E. Evidence for oxidative DNA damage in the hippocampus of elderly patients with chronic schizophrenia. American Journal of Geriatric Psychiatry, 12, 167-175. [18] Young, J., McKinney, S.B., Ross, B.M., Wahle, K.W. and Boyle, S.P. (2007) Biomarkers of oxidative stress in schizophrenic and control subjects. Prostaglandins Leu- kotrienes and Essential Fatty Acids, 76, 73-85. [19] Dietrich-Muszalska, A., Olas, B., Głowacki, R. and Bald, E. (2009) Oxidative/nitrative modifications of plasma proteins and thiols from patients with schizophrenia. Neuropsychobiology, 59, 1-7. doi:10.1159/000202822 [20] Dietrich-Muszalska, A. and Olas, B. (2007) Isoprostenes as indicators of oxidative stress in schizophrenia. World Journal of Biological Psychiatry, 11, 1-7. [21] Wang, J.F., Shao, L., Sun, X. and Young, L.T. (2009) Increased oxidative stress in the anterior cingulate cortex of subjects with bipolar disorder and schizophrenia. Bip- olar Disorders, 11 , 523-529. doi:10.1111/j.1399-5618.2009.00717.x [22] Steullet, P., Cabungcal, J.H., Kulak, A., Kraftsik, R., Chen, Y., Dalton, T.P., Cuénod, M. and Do, K.Q. (2010) Redox dysregulation affects the ventral but not dorsal hippocampus: Impairment of parvalbumin neurons, gam- ma oscillations, and related behaviors. Journal of Neuro- science, 30, 2547-2558. doi:10.1523/JNEUROSCI.3857-09.2010 [23] Cabungcal, J.H., Nicolas, D., Kraftsik, R., Cuénod, M., Do, K.Q. and Hornung, J.P. (2006) Glutathione deficit during development induces anomalies in the rat anterior cingulate GABAergic neurons. Neurobiology of Dise- ase, 22, 624-637. [24] Puri, B.K., Counsell, S.J., Ross, B.M., Hamilton, G., Bustos, M.G. and Treasaden, I.H. (2008) Evidence from in vivo 31-phosphorus magnetic resonance spectroscopy phosphodiesters that exhaled ethane is a biomarker of cerebral n-3 polyunsaturated fatty acid peroxidation in humans. BMC Psychiatry, 8. doi:10.1016/j.nbd.2006.01.003 [25] Puri, B.K., Ross, B.M. and Treasaden, I.H. (2008) In- creased levels of ethane, a non-invasive, quantitative, di- rect marker of n-3 lipid peroxidation, in the breath of pa- tients with schizophrenia. Progress in Neuropsychop- harmacology and Biological Psychiatry, 32, 858-862. doi:10.1016/j.pnpbp.2008.01.001 [26] Ross, B.M., Maxwell, R. and Glen, I. (2011) Increased breath ethane levels in medicated patients with schizo- phrenia and bipolar disorder are unrelated to erythrocyte omega-3 fatty acid abundance. Progress in Neuropsy- chopharmacology and Biological Psychiatry, 35, 436-453. [27] Dillard, C.J., Dumelin, E.E. and Tappel, A.L. (1977) Eff- ect of dietary vitamin E on expiration of pentane and eth- ane by the rat. Lipids, 12, 109-114. doi:10.1007/BF02532981 [28] Wade, C.R. and van Rij, A.M. (1985) In vivo lipid per- oxidation in man as measured by the respiratory excre- tion of ethane, pentane, and other low-molecular-weight hydrocarbons. Analytical Biochemistry, 150, 1-7. doi:10.1016/0003-2697(85)90433-6 [29] Ross, B.M., McKenzie, I., Glen, I. and Bennett, C.P. (2003) Increased levels of ethane, a non-invasive marker of n-3 fatty acid oxidation, in breath of children with at- tention deficit hyperactivity disorder. Nutritional Neuro- science, 6, 277-281. doi:10.1080/10284150310001612203 [30] Amann, A., Spanĕl, P. and Smith, D. (2007) Breath analysis: The approach towards clinical applications. Mini Reviews in Medicinal Chemistry, 7, 115-129. doi:10.2174/138955707779802606 [31] Bloor, R.N., Spanĕl, P. and Smith, D. (2006) Quantifica- tion of breath carbon disulphide and acetone following a single dose of disulfiram (antabuse) using selected ion flow tube mass spectrometry (SIFT-MS). Addiction Bi- ology, 11, 163-169. doi:10.1111/j.1369-1600.2006.00015.x [32] Giacomuzzi, S.M., Riemer, Y., Pavlic, M., Schmid, A., Hinterhuber, H. and Amann, A. (2009) Applications of breath gas analysis in addiction medicine-preliminary results. Substance Use and Misuse, 44, 301-304. doi:10.1080/10826080802344864 [33] Miljevic, C., Nikolic, M., Nikolic-Kokic, A., Jones, D.R., Niketic, V., Lecic-Tosevski, D. and Spasic, M.B. (2010) Lipid status, anti-oxidant enzyme defence and haemoglo- bin content in the blood of long-term clozapine-treated schizophrenic patients. Progress in Neuropsychopharm- acology and Biological Psychiatry, 34, 303-307. doi:10.1016/j.pnpbp.2009.11.024 [34] Singh, O.P., Chakraborty, I., Dasgupta, A. and Datta, S. (2008) A comparative study of oxidative stress and inter- relationship of important antioxidants in haloperidol and olanzapine treated patients suffering from schizophrenia. Indian Journal Psychiatry, 50, 171-176. doi:10.4103/0019-5545.43627 [35] Walss-Bass, C., Weintraub, S.T., Hatch, J., Mintz, J. and Chaudhuri, A.R. (2008) Clozapine causes oxidation of proteins involved in energy metabolism: A possible mechanism for antipsychotic-induced metabolic altera- tions. International Journal of Neuropsychopharmacol- ogy, 11, 1097-1104. doi:10.1017/S1461145708008882 [36] Martins, M.R., Petronilho, F.C., Gomes, K.M., Dal-Piz- zol, F., Streck, E.L. and Quevedo, J. (2008) Antipsycho- C opyright © 2011 SciRes. OJPsych  B. M. Ross et al. / Open Journal of Psychiatry 1 (2011) 1-7 Copyright © 2011 SciRes. 7 OJPsych tic-induced oxidative stress in rat brain. Neurotoxicolgy Research, 13, 63-69. doi:10.1007/BF03033368 [37] American Psychiatric Association. (1994) Diagnostic and statistical manual of mental health disorders. 4th Edition, American Psychiatric Publishing, Washington, DC. [38] Smith, D., Španěl, P., Enderby, B., Lenney, W., Turner, C. and Davies, S.J. (2010) Isoprene levels in the exhaled breath of 200 healthy pupils within the age range 7–18 years studied using SIFT-MS. Journal of Breath Re- search, 4, 017101. [39] Smith, D., Turner, C. and Spaněl, P. (2007) Volatile me- tabolites in the exhaled breath of healthy volunteers: Their levels and distributions. Journal of Breath Re- search, 1, 014004. 2007doi:10.1088/1752-7155/1/1/014004 [40] Abela, J.E., Skeldon, K.D., Stuart, R.C. and Padgett, M.J. (2009) Exhaled ethane concentration in patients with cancer of the upper gastrointestinal tract - A proof of con- cept study. Bioscience Tre nds, 3, 110-114. [41] Reddy, R.D., Keshavan, M.S. and Yao, J.K. (2004) Re- duced red blood cell membrane essential polyunsaturated fatty acids in first episode schizophrenia at neurolep- tic-naive baseline. Schizophrenia Bulletin, 30, 901-911. [42] Peet, M., Shah, S., Selvam, K. and Ramchand, C.N. (2004) Polyunsaturated fatty acid levels in red cell mem- branes of unmedicated schizophrenic patients. World Journal of Biological Psychiatry, 5, 92-99. doi:10.1080/15622970410029917 [43] Raffa, M., Mechri, A., Othman, L.B., Fendri, C., Gaha, L. and Kerkeni, A. (2009) Decreased glutathione levels and antioxidant enzyme activities in untreated and treated schizophrenic patients. Progress in Neuropsychophar- macology and Biological Psychiatry, 33, 1178-1183. doi:10.1016/j.pnpbp.2009.06.018 [44] Clemens, M.R., Remmer, H. and Waller, H.D. (1984) Phenylhydrazine-induced lipid peroxidation of red blood cells in vitro and in vivo: Monitoring by the production of volatile hydrocarbons. Biochemical Pharmacology, 33, 1715-1718. doi:10.1016/0006-2952(84)90338-1 [45] Clemens, M.R. and Remmer, H. (1982) Volatile alkanes produced by erythrocytes: An assay for in vitro studies on lipid peroxidation. Blut, 45, 329-335. doi:10.1007/BF00319527 [46] Einsele, H., Clemens, M.R. and Remmer, H. (1987) In vitro aging of red blood cells and lipid peroxidation. Ar- chives of Toxicology, 60, 163-166. doi:10.1007/BF00296972 [47] Fowler, D., Coyle, M. and Anderson, R. (1997) Ozone in the United Kingdom. The Fourth Report of the Oxidants Review Group. Department of the Environment, Trans- port and the Regions, London, UK. [48] Srinivasan, T.N. and Thara, R. (2002) Smoking in schiz- ophrenia - All is not biological. Schizophrenia Research, 56, 67-74. doi:10.1016/S0920-9964(01)00187-6 [49] Puri, B.K., Treasaden, I.H., Cocchi, M., Tsaluchidu, S., Tonello, L. and Ross, B.M. (2008) A comparison of oxi- dative stress in smokers and non-smokers: An in vivo human quantitative study of n-3 lipid peroxidation. MC Psychiatry, 8, Suppl 1:S4. doi:10.1186/1471-244X-8-S1-S4 [50] Habib, M.P., Clements, N.C. and Garewal, H.S. (1995) Cigarette smoking and ethane exhalation in humans. American Journal of Respiratory and Critical Care Medicine, 151, 1368-1372. [51] McCreadie, R.G. (2003) Diet, smoking and cardiovascu- lar risk in people with schizophrenia. British Journal of Psychiatry, 183, 534-539. doi:10.1192/bjp.183.6.534 [52] Wei, W., Liu, Q., Tan, Y., Liu, L., Li, X. and Cai, L. Oxi- dative stress, diabetes, and diabetic complications. Hem- oglobin, 33, 370-377. doi:10.3109/03630260903212175 [53] Bruckdorfer, K.R. (2008) Antioxidants and CVD. Pro- ceedings of the Nutrition Society, 67, 214-222. doi:10.1017/S0029665108007052 [54] Visconti, R. and Grieco, D. (2009) New insights on oxi- dative stress in cancer. Current Opinions in Drug Dis- covery Development, 12, 240-245. [55] Bushe, C.J., Bradley, A.J., Wildgust, H.J. and Hodgson, R.E. (2009) Schizophrenia and breast cancer incidence: A systematic review of clinical studies. Schizophrenia Re- search, 114, 6-16. doi:10.1016/j.schres.2009.07.012 [56] Koponen, H., Alaräisänen, A., Saari, K., Pelkonen, O., Huikuri, H., Raatikainen, M.J., Savolainen, M. and Iso- hanni, M. (2008) Schizophrenia and sudden cardiac death: A review. Nordic Journal of Psychiatry, 62, 342-345. doi:10.1080/08039480801959323 [57] Suvisaari, J., Perälä, J., Saarni, S.I., Härkänen, T., Pirkola, T., Joukamaa, M., Koskinen, S., Lönnqvist, J. and Re- unanen, A. (2008) Type 2 diabetes among persons with schizophrenia and other psychotic disorders in a general population survey. European Archives of Psychiatry and Clinical Neuroscience, 258, 129-136.
|