B. Sofiene et al.
3. Discussion
Osteosarcoma is the most common primary malignancy of bone and 5% to 6% arise in the craniofacial bones [1]
[4]. The etiology and precise pathogenesis of this disease remain unknown [1]. Osteogenic sarcoma is largely a
disease of the young but about one-third occurs in patients over 40 years of age [2] [5]. They are more common
in male than female and the vast majority of craniofacial Osteosarcomas are located in the zygomatic bone [6]
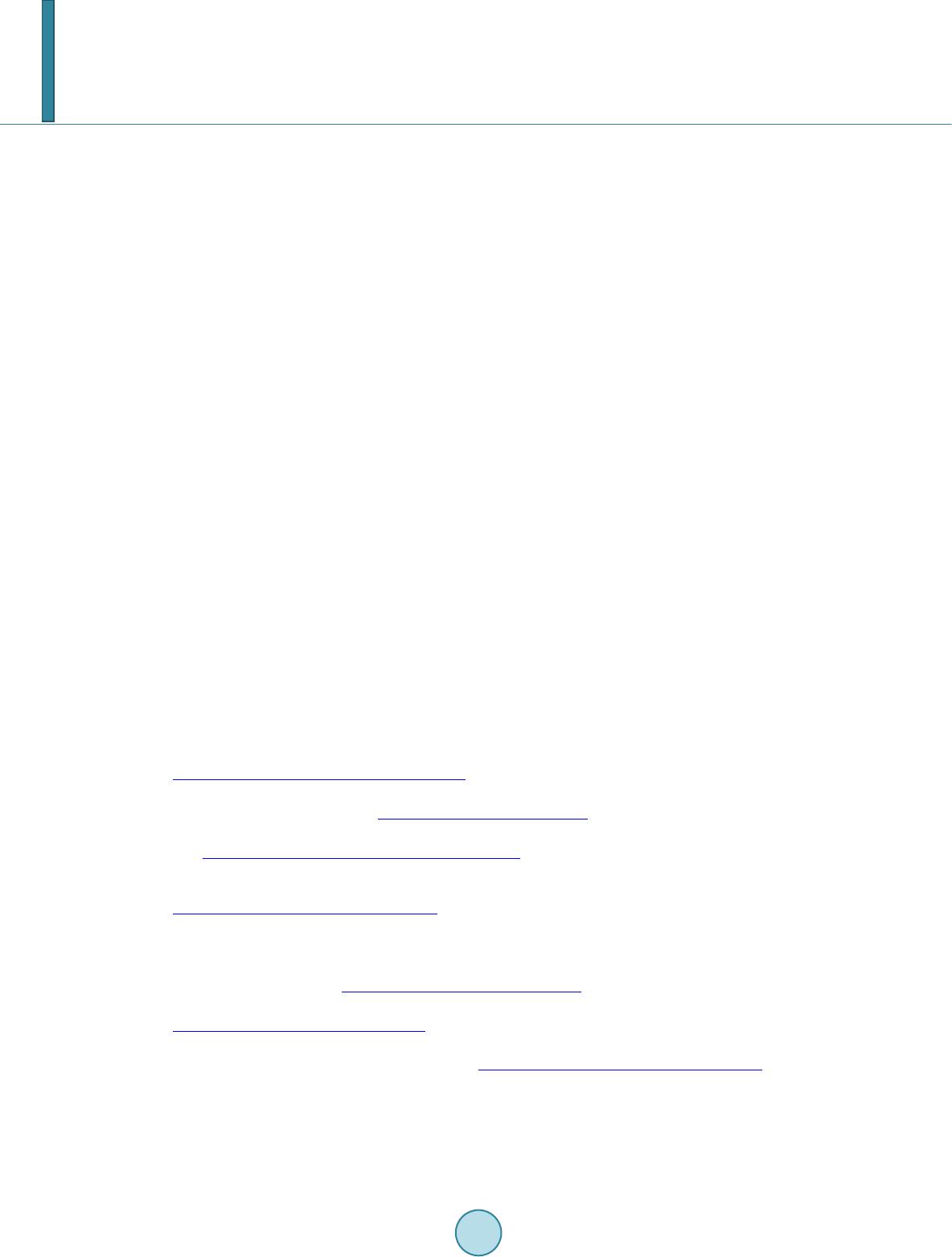
[7]. They are an aggressive neoplasm composed of spindle cells producing osteoid [8]. Clinical features are lo-
calized pain that frequently beg ins after injury.
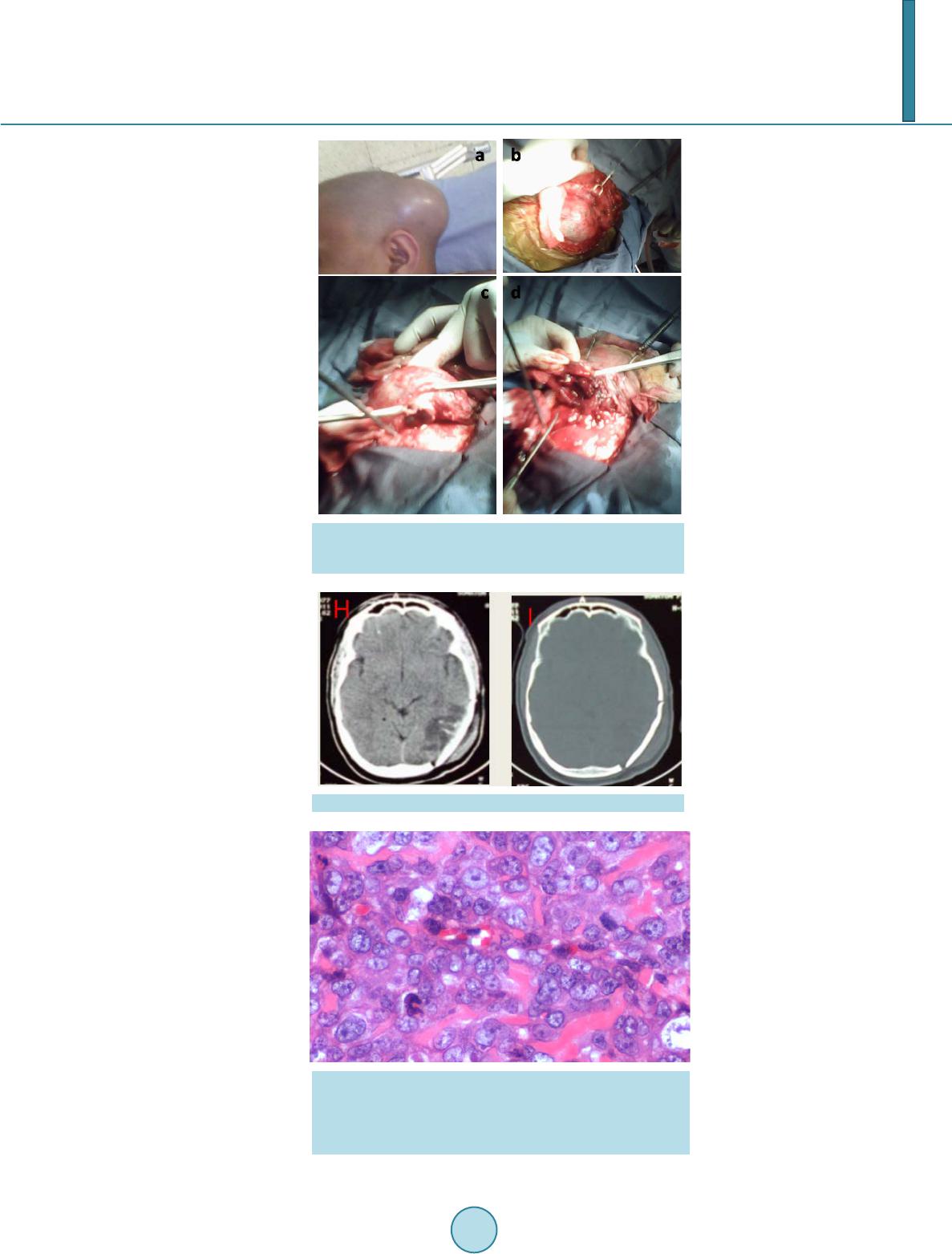
Common presenting symptoms were swelling, pain, or both and the most important finding in physical ex-
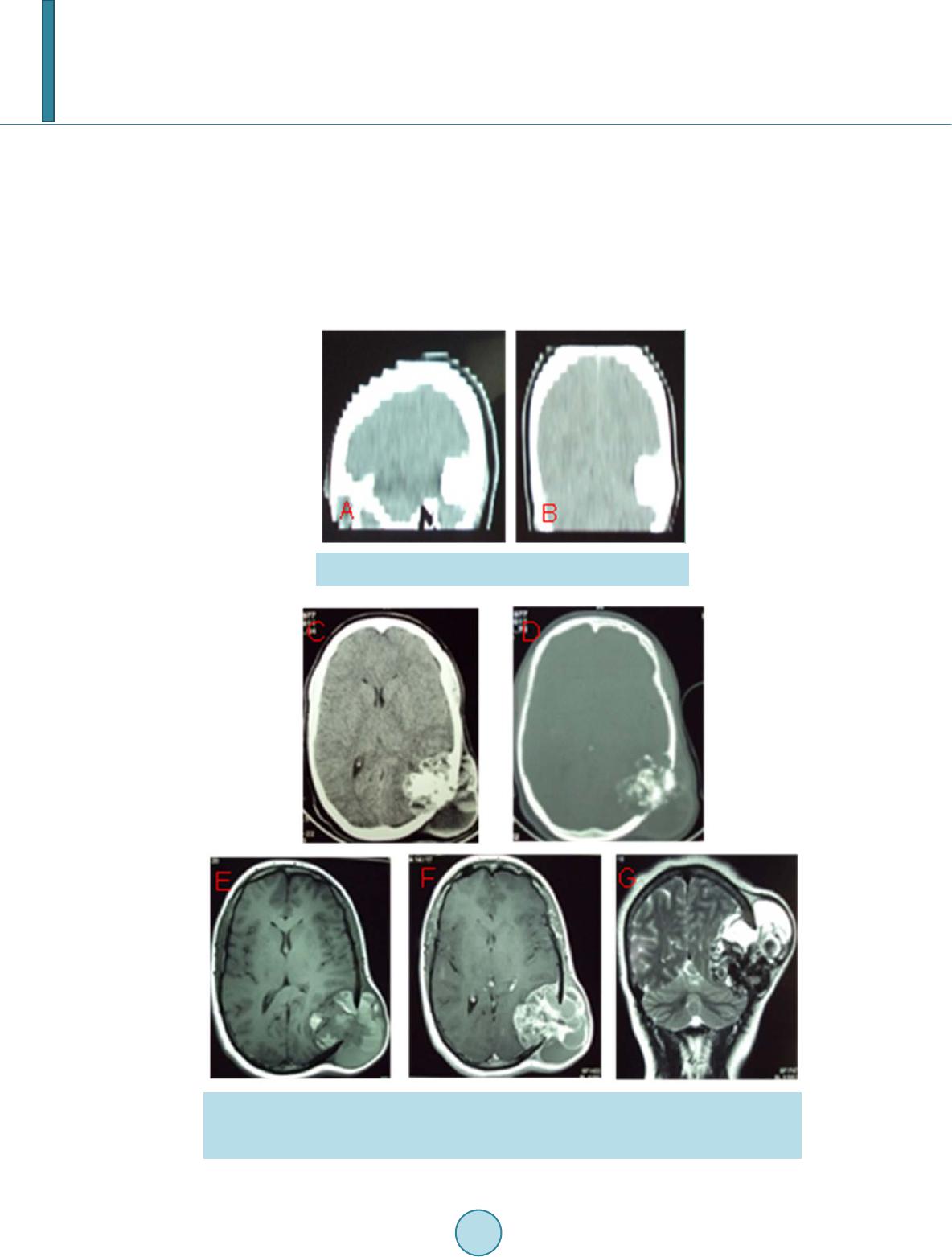
amination is a soft tissue mass, which is fr equently large and tender to palpation. Radiological investigations in-
clude CT-scan and MRI. The general radiographic features are not specific but may be osteolytic, osteoblastic or
mixed [1 ]. The spicular pattern of calcification is usually present and no radiographic finding is pathognomonic
[1] [2]. The final diagnosis of Osteosarcoma was only established by the histological studies [8].
It can be classified into three main subtype s : the chondroblastic, osteoblastic, a nd fibroblastic types [7] [8].
The recommended treatment has not yet been established, but radical surgery for extirpation including a large
margin of normal bone is the most significant factor contributing to a good outcome. Adjuvant therapy, such as
irradiation or chemotherapy can be performed if radical resection cannot be achieved. The role of chemotherapy
is less clear for cranial tumors [6 ] [7].
The 10 years survival following resection of large tumors was 69% if the resection was complete but was only
13% if excision was incomplete [1] [2].
4. Conclusion
Because of the rarity of this type of tumor and a very poor prognosis, treatment of Osteosarcomas has not yet
benefited from a rigorous evaluation and needs more studies to research the role of chemo and radiotherapy.
Conflicts of Interest
All authors declare no conflict of interest.
References
[1] Benson, J.E., Goske, M., Han, J.S., et al. (1984) Primary Osteogenic Sarcoma of the Calvaria. American Journal of
Neuroradiology, 5, 810-813.
[2] Bose, B. (2002) Primary Osteogenic Sarcoma of the Skull. Surgical Neurology, 58, 234-240.
http://dx.doi.org/10.1016/S0090-3019(02)00864-9
[3] Kanazawa, R., Yoshida, D., Takahashi, H., et al. (2003) Osteosarcoma Arising from the Skulle Case Report. Neurolo-
gia Medico-Chirurgica, 43, 88-91. http://dx.doi.org/10.2176/nmc.43.88
[4] Sturgis, E.M. and Potter, B.O. (2003) Sarcomas of the Head and Neck Region. Current Opinion in Oncology, 15, 239-
252. http://dx.doi.org/10.1097/00001622-200305000-00011
[5] Chennupati, S.K., Norris, R., Dunham, B. and Kazahaya, K. (2008) Osteosarcoma of the Skull Base: Case Report and
Review of Literature. International Journal of Pediatric Otorhinolaryngology, 72, 115-119.
http://dx.doi.org/10.1016/j.ijporl.2007.08.015
[6] Chang, C.S. (2010) Craniofacial Reconstruction of Primary Osteogenic Sarcoma of the Skull. Journal of Plastic, Re-
constructive & Aesthetic Surgery, 63, 1265-1268.
[7] Saeter, G. (2005) Minimum Clinical Recommendations for Diagnosis, Treatment and Follow-Up of Osteosarcoma. An-
nals of Oncology, 16, 71-72. http://dx.doi.org/10.1093/annonc/mdi822
[8] Fukunaga, M. (2005) Low-Grade Central Osteosarcoma of the Skull. Pathology-Research and Practice, 201, 131-135.
http://dx.doi.org/10.1016/j.prp.2004.12.001
[9] Maurizio, S. (1994) Radiation-Induced Osteosarcomas of the Skull: Report of Two Cases and Review of the Literature.
Clinical Neurology and Neurosurgery, 96, 226-229. http://dx.doi.org/10.1016/0303-8467(94)90073-6