 World Journal of AIDS, 2011, 1, 1-7 doi: 10.4236/wja.2011.11001 Published Online March 2011 (http://www.SciRP.org/journal/wja) Copyright © 2011 SciRes. WJA 1 Risk Factors for Prematurity among Neonates from HIV Positive Mothers in Cameroon Taguebue J1,2, Monebenimp F2, Zingg W1, Mve Koh V3, Atchoumi A3, Gervaix A1, Tetanye E2 1Department of Pediatrics and Adolescent Medicine, University Hospitals of Geneva, Geneva, Switzerland; 2Department of Pediat- rics, University of Yaoundé Hospital, Yaoundé, Cameroon; 3Department of Gynecology and Obstetrics, University of Yaoundé Hos- pital, Yaoundé Cameroon. Email: walter.zingg@hcuge.ch Received March 11th, 2011; revised March 15th, 2011; accepted March 18th. ABSTRACT Objective: Human immunodeficiency virus (HIV) infection is the most important chronic health condition among women in childbearing age in sub-Saharan Africa. There is sparse data about socio-economic factors in the context with adverse outcome in pregnancy. The objective of the study was to identify such factors for prematurity, low birth weight (LBW) and intrauterine growth retardation (IUGR) in infants born to HIV-positive women in Cameroon. Meth- ods: The study was done in Yaoundé between December 2001 and November 2007. Neonates born to HIV-positive mothers were monitored and clinical data as well as socio-economic factors were tested for association with prematur- ity, LBW and IUGR. Findings: In total, 264 neonates were analyzed. More prematurity occurred when mothers at- tended less than 4 prenatal care visits (OR [95% CI]: 2.7 [1.21 - 6.05]; p = 0.015). HIV-classification > 1 resulted in more IUGR (OR [95% CI]): 3.15 [1.4 - 7.4]; p = 0.01) and LBW (2.20 [1.1 - 4.6]; p = 0.03). Single women were more likely to attend 4 prenatal care visits or more (OR [CI95%]: 2.4 [1.6 - 3.4]; p < 0.001); higher education resulted in better compliance with anaemia p rophylaxis (OR [CI95%]: 3.0 [1.5 - 5.8]; p = 0.002) and antimalaria prophylaxis (OR [CI95%]: 2.1 [1.4 - 3.3]; p < 0.001); and was associated with early HIV diagnosis (p = 0.003). Conc lus ion : Prenatal care improves outcome in pregnancy of HIV-positive women. Single mothers compared to women in family settings are more likely to attend prenatal care visits, and HIV was diagnosed earlier in pregnancy in this population. More effort should be put to address women in family settings to early diagnose HIV and to increase compliance with prenatal care. Keywords: Neonates, HIV, Pregnancy, Prematurity, Low Birth Weight, I ntr a ut eri ne Growth Retardation, Cameroon, Africa, Education 1. Introduction Low birth weight (LBW), prematurity and intrauterine growth (IUGR) is associated with considerab le morbidity and mortality in the neonatal period as well as in the first year and adult life [1-5]. LBW often is due to IUGR, prematurity or a combination of both. However, other factors such as a lower socio economic status, a single- parent family, extreme maternal age at delivery ( < 20 or > 34 years), a lower education level, short intervals be- tween pregnancies, multiple pregnancy, tobacco and/or alcohol use during pregnancy, low weight gain during pregnancy, and chronic illness of the mother have been associated with LBW as well [6-10]. Human immunodeficiency virus (HIV) infection with or without acquired immunodeficiency syndrome (AIDS) is the most important chronic health condition among women in childbearing age in sub-Saharan Africa with an estimated 12.2 millions women affected. The overall HIV prevalence in Cameroun is 5.5%. The prevalence among women in childbearing age shows geographical distribution between 5.7% up to more than 12% [11]. Studies from central Africa found that HIV-positive moth- ers are especially at risk for preterm childbirth or giving birth to a child with IUGR or LBW [12-15]. There is a direct correlation between vertical HIV transmission, LBW and a high mortality [16-19]. Before 2008, ART was not available free of charge for the HIV-treatment during pregnancy in Cameroon. However, standardized HIV prophylaxis with nevirapine and zidovudine was offered at delivery. All newborns were treated with nevirapine single dose alone (before  Risk Factors for Prematurity Among Neonates from HIV Positive Mothers in Cameroon 2 2003) or in combination with zidovudine for 4 weeks (from 2003) [20]. With the introduction of such precau- tion measures for vertical transmission more and more women were offered an HIV-test during pregnancy. A steady increase of HIV-testing revealed to what extent of offspring was at risk for HIV and related health condi- tions in Cameroon. The aim of this study was 1) to iden- tify LBW, IUGR and prematurity of children born to HIV-positive mothers; and 2) to identify modifiable risk factors associated with LBW, IUGR and prematurity of infants born to HIV-positive women. 2. Methods Setting: This prospective cohort study was done at the University of Yaoundé Teaching Hospital (UYT), one of four university hospitals in Yaoundé. The department of gynaecology and obstetrics at the UYT has an estimated 2250 deliveries per year. Inclusion criteria: all neonates born to HIV positive mothers were prospectively included in the study be- tween December 2001 and November 2007 if: 1) they were born at UYT; 2) has an HIV-positive mother; who 3) attended at least one prenatal care visit at UYT. Only cases with at least 75% of data completed as required by the case related form (CRF) were included in the final analysis. Variables: Clinical data of neonates and mothers in- cluded in the study was obtained from patient charts. All mothers were checked clinically (fatigue, pallor) for anaemia on the occasion of prenatal care visits and at delivery. Haem oglobin levels were checked only if clinical signs for anaemia were present. Syphilis was routinely screened with a VDRL test at least once at the visit dur- ing pregnancy. Definitions: LBW was defined as a birth weight <2500 g. Prematurity was defined as a gestational age below 37 weeks. IUGR was defined as a birth weight below the 10th percentile of gestational age based on the UK Na- tional Healthcare Care intrauterine growth curve. The weight-to-length ratio (WLR) was calculated using the Rohrer’s ponderal index (100* weight/length3 where weight is indicated in grams and length in centimetres) [21]. A mother was considered HIV-positive when at least two different HIV antibody tests (either for HIV-1 or for HIV-2) were positive or if one positive antibody test was confirmed by a western-blot. Time of HIV-di- agnosis was stratified into four groups: 1) before preg- nancy; 2) during the first trimester; 3) during the second trimester; and 4) during the third trimester of pregnancy. Clinical stage of HIV disease was classified using the WHO clinical classification [22]. Antiretroviral therapy (ART) was defined as any combination of at least three antiretroviral drugs regardless of specific drug combina- tions or whether the substances were active or not. When available, HIV viral load, total lymphocyte cell counts, CD4 cell counts, and CD8 cell counts were recorded. The number of prenatal care visits was stratified into trimes- ters and a maximum of two visits per trimester was counted. Socioeconomic parameters such as matrimonial status, regular income and source of income of the mother were obtained from the patient files. Compliance with malaria prophylaxis was obtained from the patient charts and defined as sleeping under a mosquito net and/or taking an intermittent treatment of 1500 mg sul- fadoxine-pyrimethamine every 8-12 weeks beginning at 16 weeks of pregnancy. Malaria was suspected if the mother had a fever (>38˚C) during the pregnancy or at the time of delivery and confirmed if Plasmodium falci- parum was detected in the blood or when symptoms re- solved after anti-malaria treatment in the absence of other antimicrobial agents. Anaemia prophylaxis was defined as starting intake of iron and folic- acid daily in the third trimester or before. Anaemia was defined as haemoglobin of below 11 g/l. Syphilis was considered positive if a positive VDRL test was confirmed by a TPHA test. The diagnosis of eclampsia or preeclampsia was done on clinical grounds. Statistical Analysis: Sample size calculation was done using US-data and data from Rwanda as specific data on LBW in Cameroun are not available[19,23]. Categorical variables were compared using the x2 test; continuous variables were summarized as means or medians and compared using the Wilcoxon rank sum test. We used logistic regression to investigate the association between potential risk factors and IUGR as defined as birth weight < 10th percentile. We first investigated all poten- tial risk factors in univariate analysis. Variables associ- ated with an increased risk for IURG with a p-value < 0.2 were analyzed in multivariate analysis. A p-value < 0.05 was considered statistically significant and only variables meeting this criteria were kept in the final model. All statistical analyses were conducted using Stata 10.0 (Stata Corporation, College Station, Texas; USA). 3. Results Enrolment: Among a total of 15379 children born at UYT during the study period, 496 children were born to HIV-1-positive mothers (Figure 1): 119 neonates were excluded because their mothers did not have prenatal care at UYT and therefore information about pregnancy was not obtainable; 113 neonates were excluded from final analysis because documents were less than 75% complete. A total of 264 neonates were included in the final analysis (Figure 1). Patient Characteristics: A total of 264 neonates with a mean gestational age of 38.7 (SD: ± 2. 5 w eeks) were Copyright © 2011 SciRes. WJA  Risk Factors for Prematurity Among Neonates from HIV Positive Mothers in Cameroon3 Figure 1: Enrolment of neonates from HIV infected moth- ers for the study on risk factors of low birth weight (LBW) and intrauterine growth retardation (IUGR), University of Yaoundé Teaching Hospital, Cameroon (December2001- November 2007). (1UYT: University of Yaoundé Teaching Hospital) Table 1. Characteristics of neonates born from HIV positive mothers, University of Yaoundé Teaching Hospital, Cam- eroon (December2001- November 2007). Mean (SD1) Median (IQR2) Weight, g 3025.5 (599) 3,093 (2,752-3,388) Length, cm 48.9 (3.2) 50 (48-51) Head circumfere nc e , cm 33.6 (2.4) 34 (33-35) Weight to length ratio 2.56 (0.36) 2.53 (2.34-2.74) Gestational ages, weeks 38.7 (2.5) 39 (38-40) Age (mothers) , years 27.9 (4.8) 27 (25-31) 1SD: standa r d d eviation. 2IQR: interquartile range. included and analysed in the study (Table 1). Ten neo- nates were twins (3.8%) and 128 (48.5%) were female. A total of 39 (14.8%) had a LBW, 24 (9.1%) had an IUGR and 36 (13.6%) were premature. The mean birth weight, the mean birth length and the mean head circumference were 3026 g (SD: ± 599 g), 48.9 cm (SD: ± 3.2 cm) and 33.6 cm (SD: ± 2.4 cm), respectively; the median weight-to-length ratio was 2.53 (interquartile range [IQR]: 2.34 – 2.74); 26 (9.8%) neonates had a weight-to- length ratio below the 10th percentile (Table 1). A total of 259 HIV-positive mothers were included an d analysed in the study (Table 2). The median age was 27 years (IQR: 25-31 years) at the time of delivery. A total of 149 (58%) were married, and 148 (57%) were jobless. Only 10 (4%) HIV-positive mothers were illiterates. Most Table 2. Characteristic of HIV-positive mothers, University of Yaoundé Teaching Hospital, Cameroon (December2001- November 2007). HIV classification st age 2 or 3, n (%) 28/259 (10.8) Syphilis, n (%) 8/259 (3.1) Anaemia, n (%) 34/259 (13.1) Single, n (%) 149/259 (57.5) Jobless, n (%) 148/259 (57.1) Education Illiterate, n (%) 10/259 (3.9) Primary s ch o ol le v el , n (%) 67/259 (25.9) Secondary school level, n (%) 128/259 (49.4) University level, n (%) 54/259 (20.8) mothers ended school at secondary school level [n = 128 (49%)], followed by 67 (26%) who ended school at a primary school level, and 54 (21%) who had a university degree. Prenatal Care: A total of 96 (37%) mothers were first para, 82 (32%) second, 35 (13%) third, and 46 (18%) fourth para or more. Most (202; 78%) attended 4 prenatal care visits or more, 30 (12%) attended 3 visits, 22 (8%) attended 2 visits, and 4 (2%) attended only one visit. HIV was diagnosed among 89 (34%) mothers before preg- nancy, among 74 (29%) mothers in the first trimester, among 63 (24%) in the second trimester and among 33 (13%) in the third trimester of pregnancy. Most HIV- positive mothers were at WHO-stage 1 at delivery [231 (89%)], 23 (9%) were at stage 2 and 5 (2%) at stage 3. Only 13 (5%) mothers were offered antiretro v iral therapy (ART) during pregnancy. HIV laboratory parameters such as viral load, CD4 cell counts, and CD8 cell counts were obtained only for 6 (2%) HIV-positive women. Anaemia prophylaxis was observed by the majority of the mothers 243 (94%). There was significantly more anaemia (p = 0.003) among mothers without taking a combination of folic acid and iron. Malaria prophylaxis was observed by 211 (81%) mothers. Sixteen (6%) were diagnosed with malaria in the third trimester or at deliv- ery. There was no significant association between com- pliance with malaria prophylaxis and clinical disease (p = 0.20). Eight mothers (3%) were diagnosed with syphilis and received benzathine penicillin treatment during pregnancy. No ne onate was found with congenital syph i- lis. Risk factor Analysis: Multivariate analysis showed that twins were significantly more at risk for LBW (OR [95% CI]: 11.5 [3.1 - 43.5]; p < 0.001), or being preterm (13.5 Copyright © 2011 SciRes. WJA 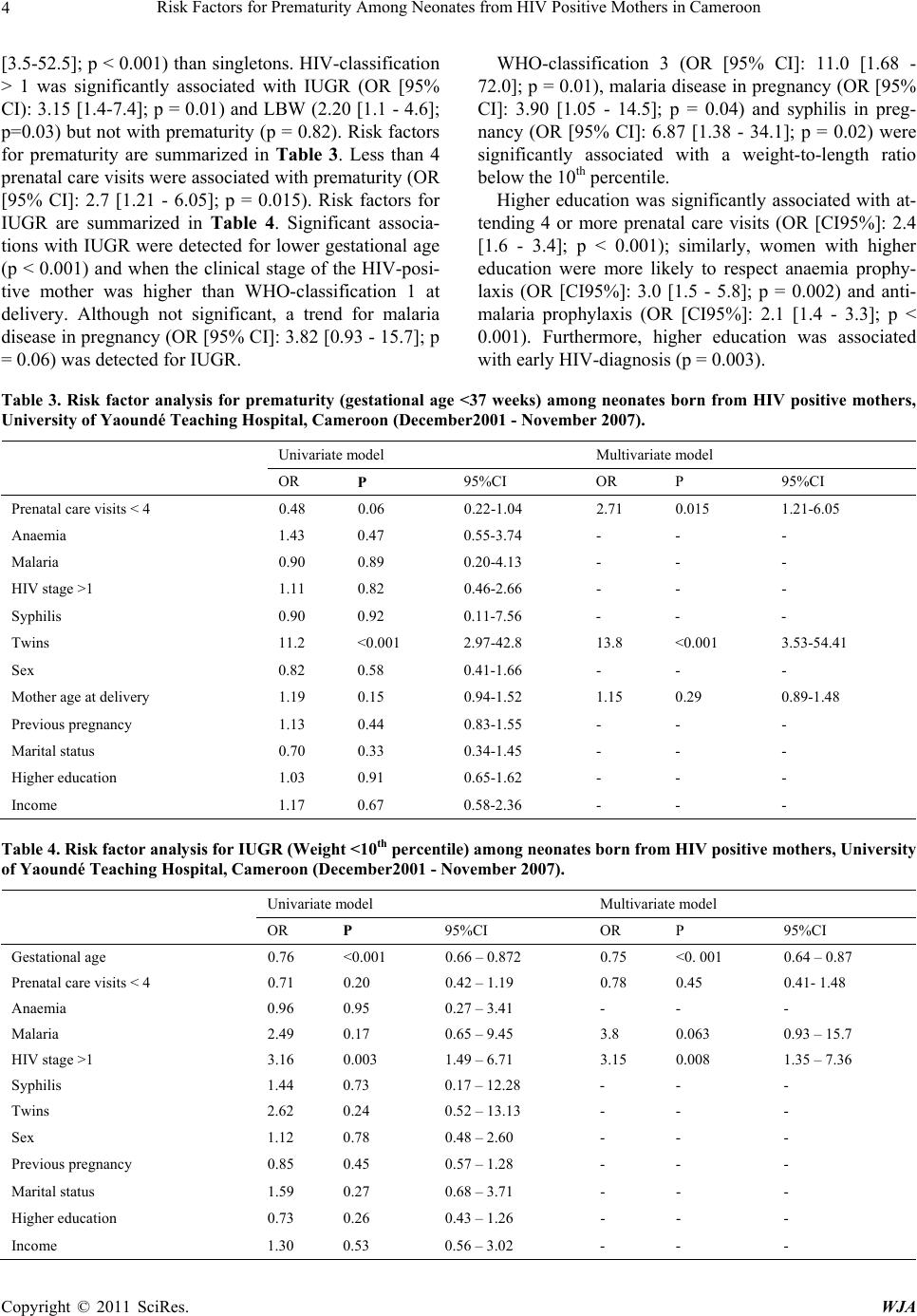 Risk Factors for Prematurity Among Neonates from HIV Positive Mothers in Cameroon Copyright © 2011 SciRes. WJA 4 [3.5-52.5]; p < 0.001) than singletons. HIV-classification > 1 was significantly associated with IUGR (OR [95% CI): 3.15 [1.4-7.4 ]; p = 0.01) and LBW (2.20 [1 .1 - 4.6]; p=0.03) but not with prematurity ( p = 0.82). Risk factors for prematurity are summarized in Table 3. Less than 4 prenatal care visits were associated with prematurity (OR [95% CI]: 2.7 [1.21 - 6.05]; p = 0.015). Risk factors for IUGR are summarized in Table 4. Significant associa- tions with IUGR were detected for lower gestational age (p < 0.001) and when the clinical stage of the HIV-posi- tive mother was higher than WHO-classification 1 at delivery. Although not significant, a trend for malaria disease in pregnan cy (OR [95% CI]: 3.82 [0.93 - 15 .7]; p = 0.06) was detected for IUGR. WHO-classification 3 (OR [95% CI]: 11.0 [1.68 - 72.0]; p = 0.01), malaria disease in pregnancy (OR [95% CI]: 3.90 [1.05 - 14.5]; p = 0.04) and syphilis in preg- nancy (OR [95% CI]: 6.87 [1.38 - 34.1]; p = 0.02) were significantly associated with a weight-to-length ratio below the 10th percentile. Higher education was significantly associated with at- tending 4 or more prenatal care visits (OR [CI95%]: 2.4 [1.6 - 3.4]; p < 0.001); similarly, women with higher education were more likely to respect anaemia prophy- laxis (OR [CI95%]: 3.0 [1.5 - 5.8]; p = 0.002) and anti- malaria prophylaxis (OR [CI95%]: 2.1 [1.4 - 3.3]; p < 0.001). Furthermore, higher education was associated with early HIV- diagnosis (p = 0.003). Table 3. Risk factor analysis for prematurity (gestational age <37 weeks) among neonates born from HIV positive mothers, University of Yaoundé Teaching Hospital, Cameroon (December2001 - November 2007). Univariate model Multivariate model OR P 95%CI OR P 95%CI Prenatal care visits < 4 0.48 0.06 0.22-1.04 2.71 0.015 1.21-6.05 Anaemia 1.43 0.47 0.55-3.74 - - - Malaria 0.90 0.89 0.20-4.13 - - - HIV stage >1 1.11 0.82 0.46-2.66 - - - Syphilis 0.90 0.92 0.11-7.56 - - - Twins 11.2 <0.001 2.97-42.8 13.8 <0.001 3.53-54.41 Sex 0.82 0.58 0.41-1.66 - - - Mother age at delivery 1. 19 0.15 0.94-1.52 1.15 0.29 0.89-1.48 Previous pregnancy 1.13 0.44 0.83-1.55 - - - Marital status 0.70 0.33 0.34-1.45 - - - Higher education 1.03 0.91 0.65-1.62 - - - Income 1.17 0.67 0.58-2.36 - - - Table 4. Risk factor analysis for IUGR (Weight <10th percentile) among neonates born from HIV positive mothers, University of Yaoundé Teaching Hospital, Cameroon (December2001 - November 2007). Univariate model Multivariate model OR P 95%CI OR P 95%CI Gestational age 0.76 <0.001 0.66 – 0.872 0.75 <0. 001 0.64 – 0.87 Prenatal care visits < 4 0.71 0.20 0.42 – 1.19 0.78 0.45 0.41- 1.48 Anaemia 0.96 0.95 0.27 – 3.41 - - - Malaria 2.49 0.17 0.65 – 9.45 3.8 0.063 0.93 – 15.7 HIV stage >1 3.16 0.003 1.49 – 6.71 3.15 0.008 1.35 – 7.36 Syphilis 1.44 0.73 0.17 – 12.28 - - - Twins 2.62 0.24 0.52 – 13.13 - - - Sex 1.12 0.78 0.48 – 2.60 - - - Previous pregnancy 0.85 0.45 0.57 – 1.28 - - - Marital status 1.59 0.27 0.68 – 3.71 - - - Higher education 0.73 0.26 0.43 – 1.26 - - - Income 1.30 0.53 0.56 – 3.02 - - -  Risk Factors for Prematurity Among Neonates from HIV Positive Mothers in Cameroon5 4. Discussion This is the first and largest cohort study on neonates born to HIV-positive mothers in Central Africa. Three modi- fiable risk factors for LBW, IUGR or prematurity were detected: 1) poor prenatal care; 2) maternal HIV clinical stage of WHO-classification >1 at deliver y; 3) an d syph i- lis and malaria disease in pregnancy, resp ectively. While an advanced clinical stage of HIV infection was associ- ated with prematurity as well as IUGR, poor prenatal care was associated with prematurity and syphilis or ma- laria was associated with IUGR. Poor prenatal care in the absence of maternal illness has been shown to be associated with adverse outcome such as LBW in Pakistan and Madagascar [24-26]. A study which was done in the US did not show a differ- ence between two groups of different numbers of prena- tal care visits [27]. However, the mean number of visits was high (9 visits vs. 14 visits) compared to our popula- tion as well as to other populations in developing coun- tries. Prenatal care visits among HIV-positive women must be considered much more important. The finding that prematurity is associated with less prenatal care vis- its among a population without antiretroviral treatment as ours suggests that non-HIV-specific care is fundamental in the prevention of prematurity. Prenatal care includes physical examination, control of fetal growth and devel- opment, giving advice for a healthy diet, and motivating mothers to respect prophylaxis for malaria, anaemia and neural tube defects. Women attending prenatal care visits are more likely to respect such recommendations as we have seen in our population where the association be- tween the number of consultations and compliance with anaemia prophylaxis was significant (p < 0.001). Women with higher education were significantly more likely to attend prenatal care visits and to observe pro- phylaxis recommendations for anaemia, neural tube de- fects and malaria in our study. However, education level as well as other maternal socio-economic factors such as being married, having a job, or having regular income was not found to be significantly associated with LBW, IUGR or prematurity. This is most likely due to th e study size. Maternal illiteracy has been shown to be a risk for adverse outcome in pregnancy [6,7,12,16]. Similarly, even if a direct association between maternal education and LBW, IUGR or prematurity could not have been shown in our study, women with higher education at- tended prenatal care more often and were more likely to respect advice for prophylaxis. Higher education was found more often among unmarried women. Thus, un- married parenting women in our study were more likely to seek prenatal care. The finding that most HIV-positive women in our study were single represents an overall trend in Cameroon. The fact that single mothers in our study were more likely to seek help from hospital institu- tions can be interpreted as a positive finding. Once ART is made widely available for the treatment of pregnant women, regular prenatal care visits are essential. Thus it is good to know that single mothers who represent the majority of pregnant HIV-positive women can be moti- vated for regular prenatal controls. On the other hand, in industrialized countries it has been shown that prenatal stress is associated with prematurity and LBW [28]. Sin- gle parenting women usually face considerable pressure while working and car ing for a child already wh en being pregnant and being HIV-positive makes this even worse. Further studies would have to reveal what “stress” means in the setting of a developing country such as Cameroon and whether the association would be similar. The finding that illiterate women are less likely to at- tend prenatal care visits is troubling. Such women are more often married and although they have a regular in- come and their nutritional status may be better they de- pend largely on their husbands while their illiteracy is a handicap to find a job. This prevents them from obtain- ing appropriate information about precaution measures in pregnancy. As a consequence, they have a low compli- ance with prophylaxis measures and worse, HIV-infection often is diagnosed not before the third trimester or at delivery (p < 0.001). In the light of efficient HIV-prophylaxis by ART during pregnancy which are now - available this finding is worrying. Much effort will have to be invested in reaching and motivating married women to get tested for HIV before or early in pregnancy and to attend regular prenatal care visits. Our risks for adverse outcomes such as LBW, IUGR and prematurity were similar to a study among 1500 women for maternal risk factors [29]. A total of 11.7% were HIV-positive and 9.9% had malaria (61% in our study). Rates for prematurity were similar but our study showed a higher proportion of LBW (15% vs. 8%). Similar to our study there was a significant association between IUGR and maternal malaria in pregnancy. Our numbers are in line also with others studies in developing countries [9-11,16,30]. It is somewhat surprising that our rates of adverse outcome were not much higher consid- ering the fact that all women we included in our study were HIV-positive. The most likely explanation for this is the fact that most HIV-positive women 236 (91%) in our study had HIV-disease of WHO-classification 1. Consequently, HIV-disease as measured by the WHO- classification in our study was independently associated with IUGR. HIV-status alone does not predict adverse outcome but severity of HIV-disease and AIDS does. Thus, a populatio n of HIV-positive women shou ld not be considered to be homogeneous. Copyright © 2011 SciRes. WJA 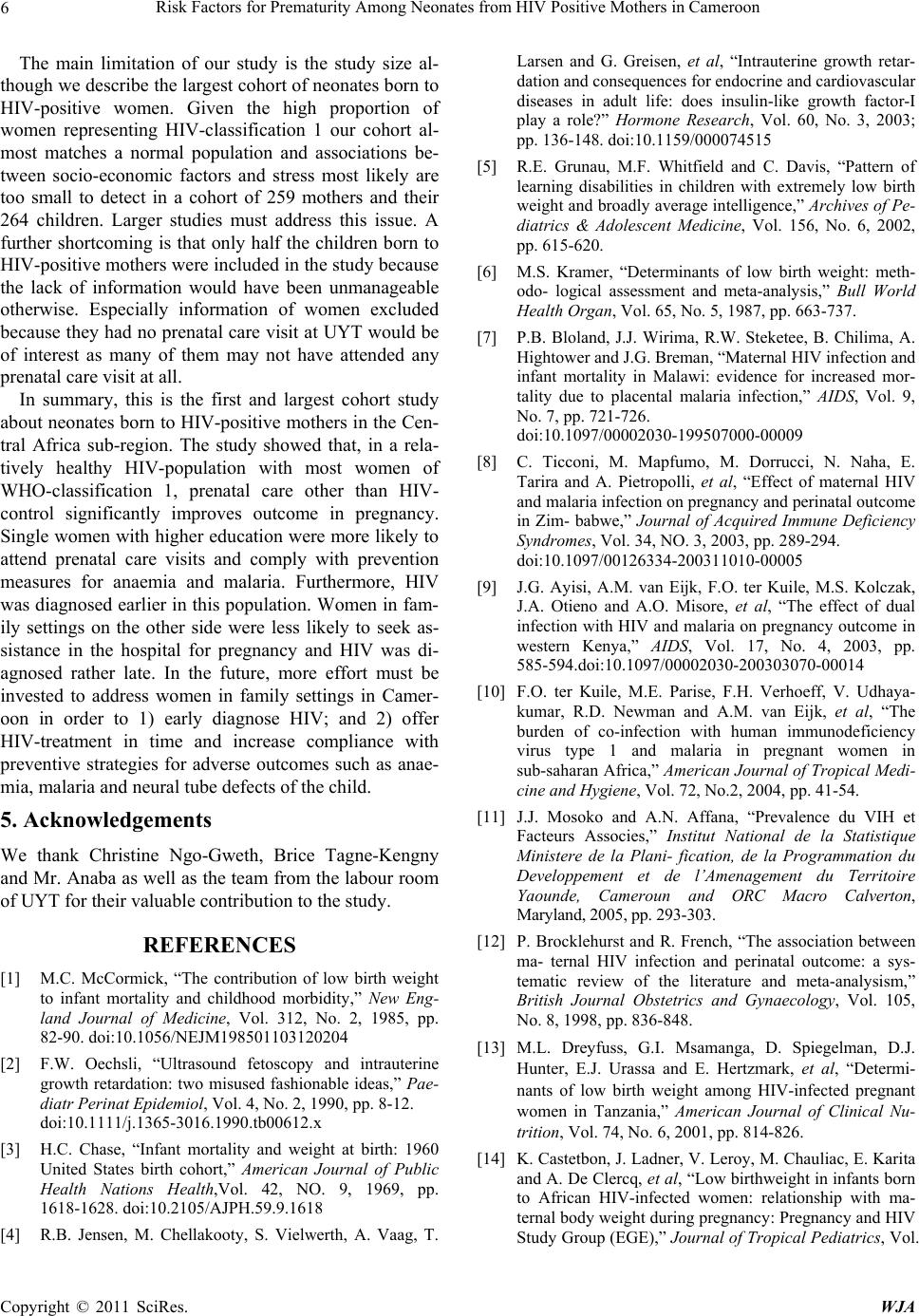 Risk Factors for Prematurity Among Neonates from HIV Positive Mothers in Cameroon 6 The main limitation of our study is the study size al- though we describe the largest cohort of neonates born to HIV-positive women. Given the high proportion of women representing HIV-classification 1 our cohort al- most matches a normal population and associations be- tween socio-economic factors and stress most likely are too small to detect in a cohort of 259 mothers and their 264 children. Larger studies must address this issue. A further shortcoming is that only half the children born to HIV-positive mothers were included in the study becaus e the lack of information would have been unmanageable otherwise. Especially information of women excluded because they had no prenatal care visit at UYT would be of interest as many of them may not have attended any prenatal care visit at all. In summary, this is the first and largest cohort study about neonates born to HIV-po sitive mothers in the Cen- tral Africa sub-region. The study showed that, in a rela- tively healthy HIV-population with most women of WHO-classification 1, prenatal care other than HIV- control significantly improves outcome in pregnancy. Single women with h igher education were more likely to attend prenatal care visits and comply with prevention measures for anaemia and malaria. Furthermore, HIV was diagnosed earlier in this population . Women in fam- ily settings on the other side were less likely to seek as- sistance in the hospital for pregnancy and HIV was di- agnosed rather late. In the future, more effort must be invested to address women in family settings in Camer- oon in order to 1) early diagnose HIV; and 2) offer HIV-treatment in time and increase compliance with preventive strategies for adverse outcomes such as anae- mia, malaria and neural tube defects of the child. 5. Acknowledgements We thank Christine Ngo-Gweth, Brice Tagne-Kengny and Mr. Anaba as well as the team from the labour room of UYT for their valuable contribution to the study. REFERENCES [1] M.C. McCormick, “The contribution of low birth weight to infant mortality and childhood morbidity,” New Eng- land Journal of Medicine, Vol. 312, No. 2, 1985, pp. 82-90. doi:10.1056/NEJM198501103120204 [2] F.W. Oechsli, “Ultrasound fetoscopy and intrauterine growth retardation: two misused fashionable ideas,” Pae- diatr Perinat Epidemiol, Vol. 4, No. 2, 1990, pp. 8-12. doi:10.1111/j.1365-3016.1990.tb00612.x [3] H.C. Chase, “Infant mortality and weight at birth: 1960 United States birth cohort,” American Journal of Public Health Nations Health,Vol. 42, NO. 9, 1969, pp. 1618-1628. doi:10.2105/AJPH.59.9.1618 [4] R.B. Jensen, M. Chellakooty, S. Vielwerth, A. Vaag, T. Larsen and G. Greisen, et al, “Intrauterine growth retar- dation and consequences for endocrine and cardiovascular diseases in adult life: does insulin-like growth factor-I play a role?” Hormone Research, Vol. 60, No. 3, 2003; pp. 136-148. doi:10.1159/000074515 [5] R.E. Grunau, M.F. Whitfield and C. Davis, “Pattern of learning disabilities in children with extremely low birth weight and broadly average intelligence,” Archives of Pe- diatrics & Adolescent Medicine, Vol. 156, No. 6, 2002, pp. 615-620. [6] M.S. Kramer, “Determinants of low birth weight: meth- odo- logical assessment and meta-analysis,” Bull World Health Organ, Vol. 65, No. 5, 1987, pp. 663-737. [7] P.B. Bloland, J.J. Wirima, R.W. Steketee, B. Chilima, A. Hightower and J.G. Breman, “Maternal HIV infection and infant mortality in Malawi: evidence for increased mor- tality due to placental malaria infection,” AIDS, Vol. 9, No. 7, pp. 721-726. doi:10.1097/00002030-199507000-00009 [8] C. Ticconi, M. Mapfumo, M. Dorrucci, N. Naha, E. Tarira and A. Pietropolli, et al, “Effect of maternal HIV and malaria infection on pregnancy and perinatal outcome in Zim- babwe,” Journal of Acquired Immune Deficiency Syndromes, Vol. 34, NO. 3, 2003, pp. 289-294. doi:10.1097/00126334-200311010-00005 [9] J.G. Ayisi, A.M. van Eijk, F.O. ter Kuile, M.S. Kolczak, J.A. Otieno and A.O. Misore, et al, “The effect of dual infection with HIV and malaria on pregnancy outcome in western Kenya,” AIDS, Vol. 17, No. 4, 2003, pp. 585-594.doi:10.1097/00002030-200303070-00014 [10] F.O. ter Kuile, M.E. Parise, F.H. Verhoeff, V. Udhaya- kumar, R.D. Newman and A.M. van Eijk, et al, “The burden of co-infection with human immunodeficiency virus type 1 and malaria in pregnant women in sub-saharan Africa,” American Journal of Tropical Medi- cine and Hygiene, Vol. 72, No.2, 2004, pp. 41-54. [11] J.J. Mosoko and A.N. Affana, “Prevalence du VIH et Facteurs Associes,” Institut National de la Statistique Ministere de la Plani- fication, de la Programmation du Developpement et de l’Amenagement du Territoire Yaounde, Cameroun and ORC Macro Calverton, Maryland, 2005, pp. 293-303. [12] P. Brocklehurst and R. French, “The association between ma- ternal HIV infection and perinatal outcome: a sys- tematic review of the literature and meta-analysism,” British Journal Obstetrics and Gynaecology, Vol. 105, No. 8, 1998, pp. 836-848. [13] M.L. Dreyfuss, G.I. Msamanga, D. Spiegelman, D.J. Hunter, E.J. Urassa and E. Hertzmark, et al, “Determi- nants of low birth weight among HIV-infected pregnant women in Tanzania,” American Journal of Clinical Nu- trition, Vol. 74, No. 6, 2001, pp. 814-826. [14] K. Castetbon, J. Ladner, V. Leroy, M. Chauliac, E. Karita and A. De Clercq, et al, “Low birthweight in infants born to African HIV-infected women: relationship with ma- ternal body weight during pregnancy: Pregnancy and HIV Study Group (EGE),” Journal of Tropical Pediatrics, Vol. Copyright © 2011 SciRes. WJA  Risk Factors for Prematurity Among Neonates from HIV Positive Mothers in Cameroon Copyright © 2011 SciRes. WJA 7 45, No. 3, 1999, pp. 152-7. doi:10.1093/tropej/45.3.152 [15] M. Bulterys, A. Chao, S. Munyemana, J.B. Kurawige, P. Naw- rocki and P. Habimana, et al, “Maternal human immunodefi- ciency virus 1 infection and intrauterine growth: a pro- spective cohort study in Butare, Rwanda,” Pediatric Infectious Disease Journal, Vol. 13, No. 2, pp. 94-100. doi:10.1097/00006454-199402000-00003 [16] P. Lepage, P. Msellati, P. Van de Perre, D.G. Hitimana and F. Dabis, “Characteristics of newborns and HIV-1 infection in Rwanda,” AIDS, Vol. 6, No. 8, 1992, pp. 882-883. [17] P. Nair, L. Alger, S. Hines, S. Seiden, R. Hebel and J.P. Johnson, “Maternal and neonatal characteristics associ- ated with HIV infection in infants of seropositive women,” Journal of Acquired Immune Deficency Syndromes, Vol. 6, No. 3, 1993, pp. 298-302. [18] T.E. Taha, G.A. Dallabetta, J.K. Canner, J.D. Chiphangwi, G. Liomba and D.R. Hoover, et al, “The effect of human im- munodeficiency virus infection on birthweight, and infant and child mortality in urban Malawi,” International journal of Epidemiology, Vol. 24, No. 5, 1995, pp. 1022-1029. doi:10.1093/ije/24.5.1022 [19] S. Weng, M. Bulterys, A. Chao, C.A. Stidley, A. Dushimimana and E. Mbarutso, et al, “Perinatal human immunodeficiency virus-1 transmission and intrauterine growth: a cohort study in Butare, Rwanda,” Pediatrics, Vol. 102, No. 2, 1998, p. 24. doi:10.1542/peds.102.2.e24 [20] J.B. Jackson, P. Musoke, T. Fleming, L.A. Guay, D. Bagenda and M. Allen, et al, “Intrapartum and neonatal single-dose nevi- rapine compared with zidovudine for prevention of mother-to-child transmission of HIV-1 in Kampala, Uganda: 18-month follow-up of the HIVNET 012 ran- domised trial,” Lancet, Vol. 362, No. 9387, 2003, pp. 859-868. doi:10.1016/S0140-6736(03)14341-3 [21] L.O. Lubchenco, C. Hansman and E. Boyd, “Intrauterine growth in length and head circumference as estimated from live births at gestational ages from 26 to 42 weeks,” Pediatrics, Vol. 37, No. 3, 1966, pp. 403-408. [22] R. Teck, O. Ascurra, P. Gomani, M. Manzi, O. Pasulani and J. Kusamale, et al, “WHO clinical staging of HIV in- fection and disease, tuberculosis and eligibility for anti- retroviral treatment: relationship to CD4 lymphocyte counts,” International Journal of Tuberculosis and Lung Disease, Vol. 9, No. 3, 2005, pp. 258-262. [23] J. Schulte, K. Dominguez, T. Sukalac, B. Bohannon and M.G. Fowler, “Declines in low birth weight and preterm birth among infants who were born to HIV-infected women during an era of increased use of maternal anti- retroviral drugs: Pediatric Spectrum of HIV Disease, 1989-2004,” Pediatrics, Vol. 119, No. 4, 2007, pp. e900-6. doi:10.1542/peds.2006-1123 [24] R.C. Andriamady, J.M. Rasamoelisoa, H. Ravaonarivo and R.J. Ranjalahy, “Premature rupture of membranes seen at the Befelatanana maternity, Antananarivo Univer- sity Hos- pital Center,” Arch Inst Pasteur Madagascar Vol.65, No. 1-2, 1999, pp. 100-102. [25] N. Tasnim, G. Mahmud and M.S. Arif, “Impact of re- duced prenatal visit frequency on obstetric outcome in low-risk mothers,” Journal of College of Physicians Sur- geons Pakistan, Vol. 15, No. 1, 2005, pp. 26-9. [26] E.J. Kongnyuy, P.N. Nana, N. Fomulu, S.C. Wiysonge, L. Kouam and A.S. Doh, “Adverse perinatal outcomes of ado- lescent pregnancies in Cameroon,” Maternal and Child Health Journal, Vol. 12, No. 2, 2008, pp. 149-154. doi:10.1007/s10995-007-0235-y [27] R.S. McDuffie Jr., A. Beck, K. Bischoff and J. Cross, “Orleans M. Effect of frequency of prenatal care visits on perinatal outcome among low-risk women. A randomized con- trolled trial,” Journal of the American Medical As- sociation, Vol. 275, No. 11, 1996, pp. 847-851. doi:10.1001/jama.275.11.847 [28] P.H. Rondo, R.F. Ferreira, F. Nogueira, M.C. Ribeiro, H. Lobert and R. Artes, “Maternal psychological stress and distress as predictors of low birth weight, prematurity and intrauter- ine growth retardation,” European Journal of Clinical Nutrition, Vol. 57, No. 2, 2003, pp. 266-72. doi:10.1038/sj.ejcn.1601526 [29] D. Watson-Jones, H.A. Weiss, J.M. Cha ngalucha, J. Todd, B. Gumodoka and J. Bulmer, et al, “Adverse birth out- comes in United Republic of Tanzania--impact and pre- vention of maternal risk factors,” Bull World Health Or- gan, Vol. 85, No. 1, 2007, pp. 9-18. doi:10.2471/BLT.06.033258 [30] M.S. Kramer, “The epidemiology of adverse pregnancy outcomes: an overview,” Journal of Nutrition, Vol. 133, No. 5, Suppl.2, 2003, pp. 1592S-6S.
|