 Open Journal of Obstetrics and Gynecology, 2014, 4, 197-207 Published Online March 2014 in SciRes. http://www.scirp.org/journal/ojog http://dx.doi.org/10.4236/ojog.2014.44033 How to cite this paper: Devabhaktuni, P., Gupta, P.C., Bhupatiraju, S., Puranam, B. and Abdul, S.M. (2014) Uterine Fibro- myoma and Intravascular Thrombosis—Eight Cases. Open Journal of Obstetrics and Gynecology, 4, 197-207. http://dx.doi.org/10.4236/ojog.2014.44033 Uterine Fibromyoma and Intravascular Thrombosis—Eight Cases Pratibha Devabhaktuni1, Prem C. Gupta2, Somaraju Bhupatiraju3, Balamba Puranam4, Saleem M. Abdul5 1Department of Obstetrics and Gynaecology, CARE In stitu te of Medical Sciences, Hyderabad, India 2Department of Vascular Surgery, CAR E Institute of Medic al Sciences, Hyderabad, India 3Department of Cardiology, CARE Institute of Medical Sciences, Hy derab ad, India 4Institute of Obstetrics and Gynaecology, Osmania Medical College, Hyderabad, India 5Department of Surgery, CARE Institute of Medical Sciences, Hyderabad, India Email: dpdnk@yahoo.com Received 27 December 2013; revised 25 January 2014; accepted 3 February 2014 Copyright © 2014 by authors and Scientific Research Publishin g Inc. This work is licensed under the Creative Commons Attribution International License (CC BY). http://creativecommons.org/licenses/by/4.0/ Abstract Objectives: We pres ent eight cases of v ascular thrombosis of the pelvic vessels and deep venous thrombosis (DVT) of the low e r lim b, second ary to compression of the pelvic vessels by the uterine fibroid, m anaged ove r a span of twelve years from 2001 to 2013 . We discuss the mean size of the leiomyoma, the predi li cti on for DVT of the left low er limb, the role of or al contrace ptives when used in women wit h large fibroids, to increase the risk of DVT and present a brief literature review. Results: Age, the mean age of our patients was—41.12 yrs, range—18 yrs to 50 yrs. Parity and Menopausal Status: Seven were parous wome n. On e was unmarried, nulligravid. Seven wer e premenopausal and one was postmenopausal. Vascular Thrombosis: In one it was arterial thrombosis and in seven it was venous thrombosis. DVT was on the left side in −6/8 - 75%. Clinical Complaints: The presenting complaints were heavy menstrual bleeding in three, severe dysme- norrhoea and heavy bleeding in one, mass per abdomen in one, heavy mens es and abdomi nal mass in one, no complain ts apart fr om DVT in one. Uterine Enlargeme nt: The size of the uterus was between 12 to 26 weeks. The mean size was 20 weeks. It was a single fibromyoma in six and multiple, t wo in t wo. Use of Or al Contraceptives: OC pills were used to control heavy menstrual bleeding in three cases—3/8, 37.5%. Discussion: T he DVT was on the left side in six of our cases, 75% were on the left s ide in our series . Menstrual problems like heavy bleed ing can be secondary to fibromyoma. Three of the eight—37.5%, women used OC pills to control menorrhagia. One developed DVT after on e cycle of use of OC pi lls; th e second developed arterial thrombosis of the pelvic vessels after four cycles of OC pill use; the thir d used OC pills for a longer period, on and off.  P. Devabhaktuni et al. The woman who developed ar teri al thrombosis wa s usin g OC pills wi t h 50 mcgs of oestrogen and 0.5 mg norgestrel. Conclusions: Uterine lei omyoma can cause vascu lar thrombosis secondary to compression of the pelvic vessels. The mean size of the uterine enlargem ent by the fibromyoma was 20 weeks and in 6/8, it was a solitary fibromyoma. DVT was on the left side in 75% of our cases. Use of OC pills in women with an enlarged uterus with leiomy oma can incre ase the ris k of DVT. Keywords Fibroid; Leiomyoma; DVT; Intravascular Thrombosis; IVL; Intravenous Leiomyomatosis; PTE 1. Introduction Deep vein thrombosis (DVT) of the pelvic and femoral veins has been reported in association with uterine fi- bromyoma [1]-[16]. In women presenting with acute pulmonary thromboembolism, the possibility of uterine leiomyoma causing DVT of the pelvic vessels should be entertained [17]-[25]. Acute PTE secondary to a large uterine leiomyoma without DVT of the lower extremities has also been reported [26]. Multiple cer ebral emboli due to foramen ovale and u terine fibromyoma have been reported [27]. Chronic non healing leg ulcer secondary to compression of the pelvic veins by the fibromyoma, leading to venous insufficiency in the leg veins, resolu- tion and complete healing after hysterectomy has been reported [28]. Acute abdomen due to mesenteric vein thrombosis secondary to compression by a large fibroid [29] and claudication due to compression of the right il- iac artery by the fibroid have been reported [30]. Association of de ep venous thrombosis with fibromyoma has be en described in cas es of intravenous leio- myomatosis also [31] [32]. Intravenous leiomyomatosis (IVL), showing unusual growth patterns of uterine leiomyoma, is a rare neo- plasm characterised by intravascular proliferation of a histologically benign looking smooth muscle tumor mass, but not invading the tissue. The criteria for the diagnosis of IVL should take into account one of the following cir cumstances [33]: 1) Multiple uterine fibroids with pathologic changes involv ing parauterine tissues and annex, especially when worm like or cable like invasive tumors are found in the blood vessels under the microscope. 2) Patients have a history of uterine fibroids or uterine surgery, accompan ied by one of the following: the right atrium tumor, right heart dysfunction, inferior venacava obstruction syndrome, Budd Chiari syndrome or deep vein thrombosis. There is a need to increase the awareness regarding the assosciation between DVT due to compression of the pelvic vessels by a large fibroid and intravenous leiomyomatosis with fibromyoma, among gynaecologists, vas- cular surgeons and cardiologists for proper early diagnosis and management. We presen t eight cases of vascular thrombosis of the pelvic vessels secondar y to compression of the pelvic vessels by the uterine fibroid, managed over a span of twelve years from 2001 to 2013. 2. Material & Methods 2.1. Case One—2001 Mrs. C, 50 yrs, para-1, live-1, abortion-1, last child birth was 27 yrs ago, attain ed menopause 10 years ago, pre- sented with deep ve in thrombosis of left lower limb in the year 2001. Doppler venous study, duplex & real time ultrasonography confirmed left ilio femoral thrombosis. Therapeutic anticoagulation with unfractionated heparin was initiated and the patient was referred to the gynaec department of Government maternity hospital, Hydera- bad, from the medical ward of Nizams institute of medical sciences. On gynaecological examination a firm mass corresponding to 24 weeks gestation was detected and a provisional diagnosis of uterine fibromyoma was made. She had no menstrual problem prior to menopause and no postmenopausal bleeding per vaginum. She had no problem related to micturition. There was no evidence of pelvic malignancy. CA-125 levels were normal. Pap. smear was normal. 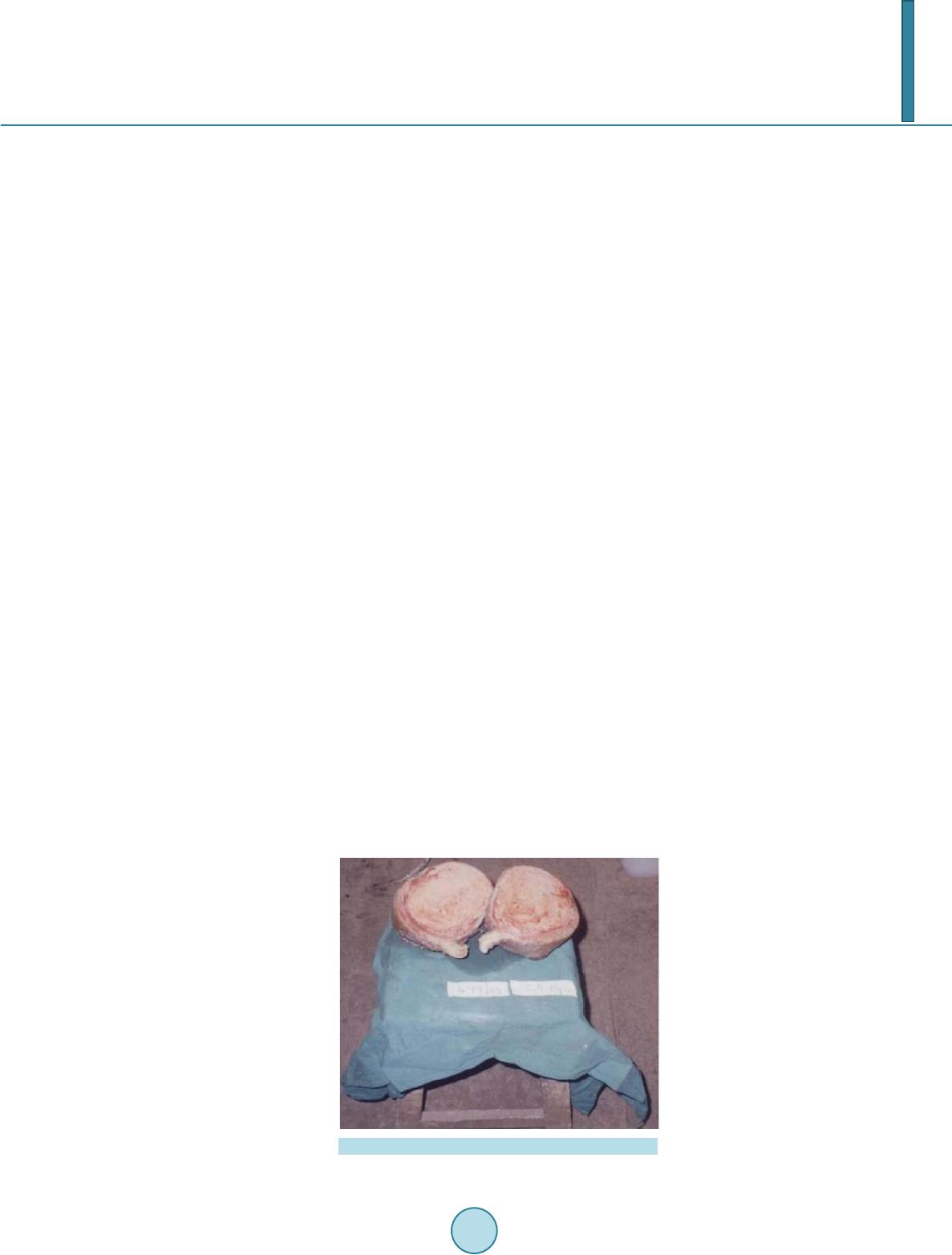 P. Devabhaktuni et al. Transvaginal ultrasonography and doppler blood flow to the mass were done, endometrium was thin (3 mm), endocervical canal was normal. Ectocervix was healthy. Other investigations were normal. Total abdominal hysterectomy and bilateral salpingo-oophorectomy were performed two months after anticoagulation, when doppler venous study revealed partial recanalisation of the thrombosed iliofemoral veins. The patient who was on oral anticoagulant after DVT, was given preoperatively and postoperatively low mo- lecular weight heparin and later again switched to ora l anticoa gulantion. Postoperativ e period was uneventful. Histopathology confirmed fibromyoma. Figure 1 shows the specimen of uterus enlarged to 20 weeks size due to a solitary fibromyoma—case one. 2.2. Case Two—2001 Miss S, 18 yrs, unmarried adolescent presented with mass per abdomen, swelling and pain over left lower limb, difficulty in walking and fever of one week duration. She gave history of mass per abdomen, gradually increas- ing in size since one year. She did not have any menstrual disturbances. Gynaecological examination revealed a 24 weeks s ize fibromyoma uterus. Duplex venous ultrasonography showed extensive thrombus extending from saphenous v ein in mid thigh upwards into femoral, external iliac and common iliac veins. A provisional diagno- sis of a large fibromyoma uterus causi n g DVT was made on 7.12.2001. She was on LMW Heparin from 17.12.01 till 8.01.02 and later on, oral anticoagulant was started. Repeat doppler studies on 11.01.02 and 29.01.02 revealed partial DVT, good collateral veins and absent thrombus in common iliac vein. She underwent Myomectomy on 7.02.2002. She was transfused three units of whole blood preoperatively and two units postoperatively. She was kept on oral anticoagulants for two months and discharged to attend the out patient department. 2.3. Case Three—2010 A 45 years woman, para 3, live 3, all three vaginal deliveries, presented to Kamineni hospital with abdominal pain and heavy menstrual bleeding of two months duration, was admitted on 18.05.2010. Clinical examination revealed the uterus to be enlarged to 26 weeks size, due to a large fibromyoma. Past history: She had deep ve- nous thrombosis in the left lower limb six years ago, she was on anticoagulants at that time. Though she was ad- vised surgery for fibroid, did not heed advise. Venus doppler study on 18.05.2010 demonstrated partial chronic thrombosis of femoral vein, saphenous vein and complete thrombosis of popliteal veins, incompetent left saph en o femoral junction with dilated great saphenous vein and varicos ities. She had TAH + BSO on 20.05.2010, received prophylactic anticoagulation, for four days postoperatively. She was advised screening for thrombophilia conditions. 2.4. Case Four—2011 A 49 years premenopausal woman was admitted with DVT of the left lower limb. Therapeutic intravenous Figure 1. Solitary uterine fibromyoma—case one.  P. Devabhaktuni et al. anticoagulation was initiated. Gynaecological examination reve a l ed the uterus enlarged due to a fibromyoma, confirmed by vaginal sonography, a solitary fibroid was detected and she was advised regarding the need to un- dergo hysterectomy at the time of discharge. But she did not report to us for surgery, must have had it elsewhere. 2.5. Case Five—2012 Mrs. N, 45 yrs, para 2, live 2, both normal vaginal deliveries, last childbirth was 22 yrs ago, tubectomy done, presented with heavy menstrual bleeding and sever e dysmenorrhoea of one year duration. She was hypothyroid on 100 mcgs. Of tab Eltroxin since four years, known hypertensive using drugs since three years . She had DVT in the rt. lower limb in July 2012, was on LMWH and chan ged over to oral anticoagulant. While on anticoagu- lants she had heavy vaginal bleeding and progesterones were given to arrest the bleeding episode. Uterus was enlarged to 14 to 16 weeks size, sonogr aphy revealed two fibroids of sizes 58 × 49 mm in fundus and 28 × 24 mm in the anterior wall of uterus. Dobutamine stress ech o was negative for inducible ischaemia, 2D ECHO was normal, cardiology fitness taken for surgery. On venus doppler of rt. lower limb on 13.09.12, there was no evi- dence of DVT. TAH + LSO were performed. Bicornuate uterus with two fibroids and a small polyp in the left cornua were noted on cut section. 2.6. Case Six—2012 Mrs R, 42 yrs, P2 L1 D1 A2, presented with history of heavy menstrual bleeding of three years duration. She used oral contraceptives (OC) for controlling menorrhagia for one month, as per the gynaecologist advis e. Developed deep venous thrombosis of left lower limb three years ago. S onography confirmed the presence of uterine fi- broids. She postponed hysterectomy for three years and was on anticoagulants. Uterus was enlarged to 24 weeks size with multiple fibroids. She had chronic rheumatic heart disease, moderate mitral stenosis, mild mitral regur- gitation. She had hypertension. She was admitted on 5-03-2012 for severe anaemia and palpitations. Two units of packed cells were transfused and oral haematenics given. Underwent total abdominal hysterectomy on 26-3-2012. 2.7. Case Seven—2013 A 49 yrs, Mrs. S, P2, L2, had tubectomy, consulted for menorrhagia since four months and on hormonal therapy (Ovral G) to control heavy bleeding. She had pain in the right lower limb, painful blisters over the right little toe two months ago. She was taking treatment for diabetes mellitus since two months and for hypertension since 15 years. Examination revealed moderate pallor, BP = 150/100 mm of Hg, on speculum examination, cervix and vaginal mucosa were healthy, bleeding through the os was noted and vaginal examination noted the uterus enlarged to 12 weeks size, fixed and not tender. Her haemoglobin was 8.6 gms, sonography revealed intramural fibroid uterus, 98 × 48 mm size, in the posterior w a ll. CT-Angiogram was done, thrombosis in the right superficial femoral artery, popliteal, posterior tibial and profunda femoris arteries was identified. Vascular surgeon was consulted. Because of menorrhagia an emer- gency hysterectomy was planned as the first step. So emergency TAH + BSO was done under spinal anaesthesia, on 2nd Jan. 2013. Anti-coagulation, low molecular weight heparin, Inj. Clexane 40 mg SC, BD, started 12 hours after surgery. Histopathology reported as fibromyoma. Right transfemoral thrombectomy was done on 10th Jan. 2013. Tab. aspirin 150 mg OD and tab. warfarin 5 mg OD started from 11th January. 2.8. Case Eight—2013 Mrs. R.S. 31 yrs. P2, L2, both lscs, tubectomy done, had last child birth, three and a half years ago. She was on oral anticoagulants when she consulted at care hospital in March 2013 for DVT of external iliac and femoral veins of left lower limb. There was associated marked left hydronephrosis & le ft hydroureter and mild rt. hy- dronephrosis, which was considered secondary to extraneous pressure eff ect by the mass. The uterus was enlarged to 24 weeks size, non mobile and tender on examination. She had MRI and CT abdomen done in addi- tion to doppler. TAH was done on 8 03 13, a large mass stony hard in consistency, from the cerv ical region fill- ing the entire pelvis was noted with no plane of cleavage to enucleate the fibromyoma. W ith difficulty the mass had to be removed in pieces, unlike the enucleation of a fibroid. There was suspicion whether it was an adeno- myoma. There could have been small pieces left behind which could not be removed. The ovaries were healthy and conserved . Histopathological examination confirmed uterine fibromyoma. Later after one month, renal  P. Devabhaktuni et al. function tests revealed the left kidney found to be non functional (95%). Rt. ureter stenting was done. On 8.08 2013, cystoscopy and rt. ureter stenting, laparoscopic left nephroureterectomy were performed. Exploratory laparotomy and removal of the mass remnants and bilateral oophorectomy were performed at the same sitting. Histopathology report was, adenomyoma, secr etory en dometrium, hydronephrosis and chronic pyelonephritis. ovaries—corpus luteal cyst rt ovary, follicular cyst lt ova ry. 3. Results 3.1. AGE The mean age of our patients was—41.12 yrs, range—18 yrs to 50 yrs. 3.2. Parity and Menopausal Status Parity: Seven were parous women. One was unmarried, nulligravid. Seven were premenopausal and one woman was ten years postmenopausal. 3.3. Vascular Thrombosis In one it was arterial thrombosis and in seven it was venous thrombosis. DVT was on the left side in −6/8 - 75%, and involving the right lower limb in −2/8 - 25%. 3.4. Clinical Complaints The presenting complaints were heavy menstrual bleeding in three, severe dysmenorrhoea and heavy bleeding in one, mass per abdomen in one, heavy menses and abdominal mass in one, no complaints apar t from DVT in one. 3.5. Uterine Enlargement The size of the uterus was between 12 to 26 weeks. The mean size was 20 weeks. It was a s ingle fibromyoma in six and multiple, two in two. 3.6. Use of Oral Contraceptives OC Pills were used to control heavy menstrual bleedig in three cases—37.5% and T. Medroxy progesterone acetate was used in one to control HMB, after DVT while she was on anticoagulants. 3.7. DVT to Surgery Interval The interval between DVT and surgery was, two months in three cases, one month in one, 3 years in one, 6 years in one and emergency hysterectomy in one, among the s even operated cases. 3.8. Comorbid Conditions Comorbid conditions were diabetes mellitus and HTN in one, hypothyroidism and HTN in one and chronic rheumatic heart disease in one. 3.9. Surgical Details Surgery: H ysterecto my was done in one case, myomectomy was done in one, hysterectomy with bilateral salpingo-oophorectomy in four and TAH + LSO in one. One patient did not report to us for surgery. A second surgical procedure five months later was needed in one, to remove the residual mass and ovarian removal, combined with left nephroureter ectomy. The clinical profile, hormonal use and surgical management are shown in Table 1. 3.10. Histopathology Histopathology reported as fibromyoma in six cases, fibromyoma and adenomyosis in one case.  P. Devabhaktuni et al. 不 Table 1. Fibromyoma & vascular thrombosis, clinical profile and surgical management of eight cases—2001 to 2013. -Total abdom inal hyste r ectomy & bilateral salp i ngo oophorectomy. 2. HMB-Heavy mens trual blee di ng. 3. OC pil l -Oral contraceptive pill. 4. CRHD-Chronic rheumatic heart dise ase.  P. Devabhaktuni et al. 4. Discussion During pregnancy, the enlarging uterus impeding blood flow in the pelvic venous system and the passage of fe- tal head through the birth canal causing trauma to the pelvic veins are two reasons mentioned, along with other hemostatic changes, to explain the greater occurrence of venous thromboembolism in pregnancy [34]. In a simi- lar manner an enlarged uterus with fibromyoma can cause impedence to blood flow in the pelvic veins predis- posing to thrombus formation. The mean age of our eight cases was 41 years, range 18 to 50 years, which is in agreement with other re- ports.Riat R. reported the mean age at presentation of th eir nine cases of fibroids with thrombosis was 41 years, range (33 - 51 years) [35]. The mean size of the fibroid uterus was 20 weeks, ran g e between 12 to 26 weeks and it was a solitary fibromyoma in 6/8 in our study. The incidence of DVT was found to be higher in cases where uterine weight was 1000 gms, or higher [8]. The DVT was on the left side in six of our cases, and on the right side in two, 75% were on the left side in our series. DVT were in the left leg in 81.9% during pregnancy [36]. Deep venous thrombosis occurred in the left lower extremity in 76% of the pregnant and 47% of the postpartum women [34]. In pregnant women with deep venous thrombosis, involvement of the left leg was reported in 82% and in 71% thrombosis was restricted to the proximal veins without involvement of the calf veins [37]. There is a greater predeliction for iliofemoral deep vein thrombosis on the left side, this may be as a consequence of the rt. iliac artery crossing the left iliac vein and compression of the left iliac vein by the gravid uterus [37]. One of the main p resenting complaints in women with uterine fibromyoma is heavy menstrual bleeding. Menstrual problems like heavy bleeding can be secondary to fibromyoma. Hormonal preparations ar e used to control heavy menstrual bleeding when mefenamic acid and tranexamic acid are unsuccessful. Three of the eight women used OC pills to control menorrhagia. One developed DVT after one cycle of use of OC pills, the second developed arterial thrombosis of the pelvic vessels after four cycles of OC pill use, the third used OC pills for a longer period, on and off. The woman who developed arterial thrombosis was using OC pills with 50 mcgs of oestrogen and 0.5 mg norgestrel. Medroxy progesterone acetate was used to control heavy menstrual bleeding in a woman on anticoagulants after she developed deep venous thrombosis. Currently available oral contraceptives still have a major impact on thrombosis occurrence and many women do not use the s af est brands with regards to the risk of venous thrombosis [38]. The risk of venous thrombosis with the cur rent oral contraceptives is fivefold compared with nouse and the risk differed with the type of pro- gestogen and dose of oestrogen. The risk of venous thrombosis in oral contraceptive users was fourfold with levonorgestrel progestogen, 5.6 fold for gestodene, 7.3 fold for desogestrel, 6.8 fold for cyproterone acetate and 6.3 fold for drospirenone, compared to nonusers [38 ]. Women taking third generation oral contraceptives have a 1.7 fold increased risk of venous thrombosis com- par ed with those taking second generation oral contraceptives [39]. Second and third generation oral contracep- tives increase the risk of venous thromboemblolism in carriers of factor V Le iden mutation by 3.3 fold and 4.2 fold respectively [40]. Factor V leiden may be important here since APC resistance has been reported in 30% of oral contraceptive pill associated thrombosis. Women using oral contraceptives with drospirenone are at similar risk of venous thromboembolism to those using oral contraceptives with desogestrel, gestodene or cyproterone and higher than those using oral contraceptives with levonorgestrel [41]. The risk of VTE was not reduced by using 20 mcg oestrogen instead of 30 mcg oestrogen in oral contraceptives with drospirenone [42]. Roberts L. N. have reported that deep venous thrombosis in association with leiomyoma was more common in women of Afro Caribbean descent and also that most women would not have thrombophilic disorders [43]. The prevalence of DVT amongst Indians was significantly higher as compared to whites an d blacks [44]. Amongst the known thrombophilia markers, only homocysteine was significantly higher in males compared with females (P = 0.006) [44]. A study on common thrombophilia markers and risk factors in Indian patients with primary DVT revealed that the commonest were elevated fibrinogen and APC-resistance (17.9% each) followed by low protein S (16.6%) [45] [46]. Thrombophilia was noted in 20% - 50% of women who experi ence VTE during Pregn ancy [47]. Our women,though advised did not get the screening tests for thrombophilia. Thrombophilia screening in women having DVT with fibromyoma would enable us to understand be tter the role of fibromyoma and throm- bophilias in the occurrence of DVT. Oral contraceptives, estrogen alone, estrogen plus progestin and progestin with or without estrogen are inde- pendent VTE risk factors [48]. As per the WHO medical eligibility criteria for contraceptive use 2009, OC pills  P. Devabhaktuni et al. can be safely advised to women with uterine fibroids without any fear of increase in the size of the fibroid, category-1 [49]. If large fibroids are accepted as an independent risk factor for DVT, th en use of OC pills in such women would compound the risk, as see n in our study. In one of our cases the tumor could not be removed in toto, she underw en t a second surgical procedure, five months later in August 2013, to resect the residual mass in the pelvis, bilateral oophorectomy was performed to prevent recu rrence and she had left laparoscopic nephroureterectomy as the left kidney was non functional. A two stage operation was performed, hysterectomy for uterine leiomyoma followed by arterial thrombec- tomy ten days later in one of our cases. In cases of IVL a cytogenetic characterization of the disease has more recently been described, consisting of the karyotype, 45, XX,der(14)t(12;14) (q15;q24),-22. These chromosomal aneusomies have been detected at different tumor sites and in different cases of intravascular and uterine leiomyomatosis, in separate patients, im- plying that the pathogenesis of both is closely related [50]. Cyto genetic studies would help to differentiate be- tween fibroids causing DVT due to compression and intravenous leiomyomatosis causing DVT, in addition to histopathology. 5. Conclusions A greater awareness regarding the uterine fibroids which are considered benign tumors and complications like DVT, IVL, ICL leading to life threatening emergency situations is necessary among gynaecologists, vascular surgeons and cardiac surgeons. From these eight cases we conclude that a uterus enlarged to 20 w eeks gestation s ize by a fibromyoma would fill the capacity of the pelvis, leading to compression of the vessels, stasis and predisposes to deep venous thrombosis. In the cas es of IVL and uterine myomas, oophorectomy has to be considered in special situations of incom- plete resection of the tumor mass [33]. Antiestrogen therapy has been used in the cases of residual tumor mass being left behind [33]. Use of OC pills, especially with high dose estrogens and third generation progestins in patients with an enlarged uter u s with leiomyoma can increase the risk of DVT. Indiscriminate use of o ral contraceptiv es without knowledge about the dose of oestrogen and the type of progestogen to control heavy menstrual bleeding needs to be curbed. It is necessary to educate the public regarding the need for surgery, when the fibroids cause the u t erus to be enlarged to 16 to 18 week s size, without procrastination, lest life threatening complications like pulmonary thromboembolism may occur. Regarding the use of oral contraceptives in women with large uterine fibromyomas, keeping th e risk of vas- cular thrombosis in mind, whether the WHO medical eligibility criteria should be revisited or modified is for the learned to muse. Deep venous thrombosis is also seen in women with intravascular leiomyomatosis, in addition to leiomyoma causing deep venous thrombosis, whether these two are two distinct entities or not, the cytogenetic studies may clarify. Acknowledgements We thank the team of doctors at CARE hospitals, Government Maternity Hospital/Osmania Medical College, Kamineni Hospital and Apollo Hospital who helped us to manage these cases. References [1] Stanko, C.M., Severson, M.A. 2n d and Molpus, K.L. (2001) Deep Venous Thrombosis Associated with Large Leio- myomata Uteri. A Case Report. The Journal of Reproductive Medicine, 46, 405-407. [2] Hawes, J., Lohr, J., Blum, B., et al. (2006) Large Uterine Fibroids Causing Mechanical Obstruction of the Inferior Vena Cava and Subsequent Thrombosis: A Case Report. Vascular and Endovascular Surgery, 40, 425-427. http://dx.doi.org/10.1177/1538574406291333 [3] Barsam, S., Bagot, C., Patel, R., et al. (2006) Extrinsic Venous Compression: A Su fficient Explanation for Venous Thromboembolism Due to Massive Fibroid s? Thrombosis and Haemostasis, 96, 694-696.  P. Devabhaktuni et al. [4] Phupong, V., Tresukosol, D., Taneepanichskul, S. and Oonkasemsanti, W. (2001) Unilateral Deep Vein Thrombosis Associated with a Large My oma Uteri: A Case Report. The Journal of Reproductive Medicine, 46, 618-620. [5] Dekel, A., Rabinerson, D., Dicker, D. and Ben-Rafael, Z. (1998) Thrombosis of the Pelvis Veins Associated with a Large Myomatous Uterus. Obstetric s & Gynecology, 92, 646-647. http://dx.doi.org/10.1016/S0029-7844(98)00203-8 [6] Chong, Y.S., Fong, Y.F., Chyne and Ng, S. (1998) Deep Vein Thrombosis in Patient with Large Uterine Myomata. Obstetrics & Gynecology, 92, 707. [7] Chandra, B.S., Nibedita, C., Ramprasad, D., Ranu, R.B., Narayan, J. and Asutosh, G. (2010) Deep Venous Thrombosis Associated with Fibroid Utrrus in a Woman Complicates by Diabetes, Hypertension and Hemiparesis. The Journal of Obstetrics and Gynecology of India, 60, 240-241. [8] Shiota, M., Kotani, Y., Umemoto, M., Tobiume, T., Tsuritani, M., Shimaoka, M. and Hoshiai, H. (2011) Deep-Vein Thrombosis Is Associated with Large Uterine Fibroids. The Tohoku Journal of Experimental Medicine, 224, 87-89. http://dx.doi.org/10.1620/tjem.224.87 [9] Khilanani, R. and Dandolu, V. (2007) Extensive Iliac Vein Thrombosis as a Rare Complication of a Uterine Leio- myoma: A Case Report. The Journal of Reproductive Medicine, 52, 537-538. [10] Asciutto, G., Mumme, A., Marpe, B., Hummel, T., Asciutto, K.C. and Geier, B. (2008) Deep Venous Thrombosis in a Patient with Large Uterine Myomata. Case Rep or t. Minerva Ginecologica, 60, 451-453. [11] Bonito, M., Gulemì, L., Basili, R., Brunetti, G. and Roselli, D. (2007) Thrombosis Associated with a Large Uterine Myoma: Case Report. Clinical & Experimental Obstetrics & Gynecology, 34, 188-189. [12] Brucka1, A., Szyłło1, K., Stefańczyk, L. and Dobrowolski1, Z. (2010) Deep Venous Thrombosis Due to Massive Compression by Uterine Myoma. Przegląd Menopauzalny, 5, 334-340. [13] Belete, H. (2012) Acute DVT Associated with IVC Compression by a U terine Mass. ConsultantLive.com [14] Osoba, L. and Ogden, J.R. (1998) Deep Vein Thrombosis Secondary to Compression by Uterine Leiomyoma. Journal of Obstetrics & Gynaecology, 18, 397. http://dx.doi.org/10.1080/01443619867290 [15] Lee, D.H., Kim, C.W., Kim, S.E. and Lee, S.J. (2012) DVT Caused by a Huge Uterine Myo ma. Hong Kong Journal of Emergency Medicine, 19, 361-363. [16] Kuwano, T., Miura, S., Nishikawa, H., Shirai, K. and Saku, K. (2008) Venous thrombosis associated with a large uter- ine myoma. Internal Medicine, 47, 809. [17] Barsam, S., Bagot, C., Patel, R., et al. (2006) Extrinsic Venous Compression: A Sufficient Explanation for Venous Thromboembolism Due to Massive Fibroids? Thrombosis and Haemostasis, 96, 694-696. [18] Ippolito, E., Buora, A., Belcaro, G., Alari, G., Arpaia, G. and Ciammaichella, G. (2012) Deep Vein Thrombosis and Pulmonary Embolism in a Patient Affected by Uterine Fibroids: Clinical Case. Panminerva Medica, 54, 97-99. [19] Nawaz, R., Haque, S. and S haha, K. (2008) Deep Vein Thrombosis and Pulmonary Embolism in a Woman with Uter- ine Myoma Bangladesh. Journal of Obstetrics & Gynaecology, 23, 78-81. [20] Falcome, M. and Serra, P. (2005) Massive Pulmonary Embolism in a Woman with Leiomyomatous Uterus Causing Pelvic Deep Venous Thrombosis. Annali Italiani di Medicina Interna, 20, 104-107. [21] Tanaka, H., Umekawa, T., Kikuka wa, T., Nakamura, M. and Toyoda, N. (2002) Venous Thromboembolic Disease Associated with Uterine Myomas Diagnosed before Hysterectomy: A Report of Two Cases. Journal of Obstetrics and Gynaecology R esearch, 28, 300-303. http://dx.doi.org/10.1046/j.1341-8076.2002.00059.x [22] Ogawa, N., Hayashi, Y., Maehara, T., Sato, S., Tobe, M., Ozaki, T., Hameda, T. and Uchida, K. (1992) A Surgically Treated Case of Acu te Pulmonary Embolism Owing to Deep Vein Thrombosis of the Leg Mainl y Caused by Uterine Myoma. Kyobu Geka, 45, 631-634. [23] Nishikawa, H., Ideishi, M., Nishimura, T., et al. (2000) Deep Venous Thrombosis and Pulmonary Thromboembolism Associated with a Huge Uterine Myoma—A Case Report. Angiology, 51, 161-166. http://dx.doi.org/10.1177/000331970005100210 [24] Huffman-Dracht, H.B. and Coates, W.C. (2010) Uterine Leiomyomata-Related Thromboembolic Disease: A Case Re- port. Journal of Emergency Medicine, 39, e101-e104. http://dx.doi.org/10.1016/j.jemermed.2008.08.020 [25] Rosenfeld, H. and By ard, R.W. (2012) Lower Extremity Deep Venous Thrombosis with Fatal Pulmonary Thromboem- bolism Caused by Benign Pelvic Space-Occupying Lesions—An Overview. Journal of Forensic Sciences, 57, 665-668. http://dx.doi.org/10.1111/j.1556-4029.2011.02047.x [26] Kurakazu, M., Ueda, T., Matsuo, K., Ishikura, H., Kumagai, N., Yoshizato, T. and Miyamoto, S. (2012) Percutaneous Cardiopulmonary Support for Pulmonary Thromboembolism Caused by Large Uterine Leiomyomata. Taiwanese Journal of Obstetrics and Gynecology, 51, 639-642. http://dx.doi.org/10.1016/j.tjog.2012.09.023 [27] Kobayashi, Z., Tanaka, H., Tao, O., Shiraishi, A., Yokota, T., Kanda , T., Mizusawa, H., Yamaguchi, H. and Hirota, N.  P. Devabhaktuni et al. (2003) Multiple Cerebral Embolism Caused by a Patent Foramen Ovale and a Uterine Myoma. No To Shinkei, 55, 705-708. [28] Ohtani, T., Tanita, M. and Tagami, H. (2003) Resolution of a Chronic Non Healing Leg Ulcer after Hysterectomy. Dermatol, 7, 530-532. [29] Sheikh, H.H. (1998) Uterine Leiomyoma as a Rare Cause of Acu te Abdomen and Intestinal Gangrene. American Journal of Obstetrics & Gynecology, 179, 830-831. [30] Zinn, H.L., Abulafia, O., Sherer, D.M. and Sclafani, S.J. (2010) Lower Extremity Claudication Resulting from Uterine Leiomyoma-Associated Common Iliac Artery Compression. Obstetri cs & Gynecology, 115, 468-470. http://dx.doi.org/10.1097/AOG.0b013e3181cb8f6c [31] Liu, W., Liu, M. and Xue, J. (2013) Detection of Intravenous Lejomymatosis with Intracardiac Extension by Ultra- sonography: A Case Report. Oncology Letters, 6, 336-338. http://dx.doi.org/10.3892/ol.2013.1387 [32] Xu, Z.-F., Yong, F., Chen, Y.-Y. and Pan, A.-Z. (2013) Uterine Intravenous Leiomyomatosis with Cardiac Extension: Imaging Characteristics and Literature Review. World Journal of Clinical Oncology, 4, 25-28. http://dx.doi.org/10.5306/wjco.v4.i1.25 [33] Liu, B., Liu, C.W., Guan, H., Li, Y.J., Song, X.J., Shen, K. and Miao, Q. (2009) Intravenous Leiomyomatosis with In- ferior Ven a Cava and Heart Extension. Journal of Vascular Surgery, 50, 897-902. [34] Jame, A.H. (2009) Venous thromboembolism: Mechanisms, Treatment, and Public Awareness Venous Thromboem- bolism in Pregnancy. Arteriosclerosis and Vascular Biology, 29, 326-331. http://dx.doi.org/10.1161/ATVBAHA.109.184127 [35] Riat, R., Chowdary, P., Mavrides, E., Magos, A. and Gatt, A. (2013) Is There an Association between Thrombosis and Fibroids? A Single Centre Experience and Literature Review. International Journal of Laboratory Hematology, 35, e13-e16. [36] Gherman, R.B., Goodwin, T.M., Leung, B., Byrne, J.D., Het humumi, R. and Montoro, M. (1999) Incidence, Clinical Characteristics, and Timing of Objectively Diagnosed Venous Thromboembolism during Pregnancy. Obstetrics and Gynecology, 94, 730-734. [37] Chan, W.S., Spencer, F.A. and Ginsbergm, J.S. (2012) Anatomic Distribution of Depp Vein Thrombosis in Pre g nancy. Canadian Medical Association Journal, 182, 657-660. http://dx.doi.org/10.1503/cmaj.091692 [38] van Hylckama Vlieg, A., Helmerhorst, F.M., Vandenbroucke, J.P., Doggen, C.J.M. and Rosendaal, F.R. (2009) The Venous Thrombotic Risk of Oral Contraceptives, Effects of Oestrogen Dose and Progestogen Type: Result of the MEGA Case-Control Study. British Medical Journal, 339, b2921. [39] Kemmeren, J.M., Algra, A. and Grobbee, D.E. (2001) Third Generation Oral Contraceptives and Risk of Venous Thrombosis: Meta-Analysi s. B ritish Medical Journal, 323, 131. [40] Simioni, P., Sanson, B.J., Prandoni, P., Tormene, D., Friederich, P.W., Girolami, B., Gavasso, S., Huisman, M.V., Buller, H.R., Wouter ten Cate, J., Girolami, A. and Prins, M.H. (1999) Department of Medical and Surgical Sciences, University Hospital of Padua, ltaly. Incidence of Venous Thromboembolism in Families with Inherited Thrombophilia. Thrombosis and Haemostasis, 81, 198-202. [41] Stegeman, B.H., de Bastos, M., Rosendaal, F.R., van Hylckama Vlieg, A., Helmerhorst, F.M., Stijnen, T. and Dekkers, O.M. (2013) Different Combined Ora l Contraceptives and the Risk of Venous Thrombosis: Systematic Revie w and Network Meta-Analysis. British Medical Journal, 347, f5298. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3771677/ http://dx.doi.org/10.1136/bmj.f5298 [42] Lidegaard, J., Nielsen, L.H., Skovlund, C.W., Skjeldestad, F.E. and Løkkegaard, E. (2011) Ri sk of Venous Thrombo- embolism from Use of Oral Contraceptives Containing Different Progestogens and Oestrogen Doses: Danish Cohort Study, 2001-9. British Medical Journal, 343, d6423. http://dx.doi.org/10.1136/bmj.d6423 [43] Roberts, L.N., Patel, R.K., Chitongo, P., Bonner, L. and Arya, R. (2013) African-Caribbean Ethnicity Is Associated with a Hypercoagulable State as Measured by Thrombin Generation. Blood Coagulation & Fibrinolysis, 24, 40-49. http://dx.doi.org/10.1097/MBC.0b013e32835a07fa [44] Pai, N., Ghosh, K. and Shetty, S. (2012) Cause of Deep Venous Thrombosis and Pulmonary Embolism in Young Pa- tients from India as Compared with Other Ethnic Groups. Blood Coagulation & Fibrinolysis, 23, 257-261. http://dx.doi.org/10.1097/MBC.0b013e3283502961 [45] Mishra, M.N. and Bedi, V.S. (2010) Prevalence of Common Thrombophilia Markers and Risk Factors in Indian Pa- tients with Prima ry Venous Thrombosis. Sao Paulo Medical Journal, 128, 263-267. mnmishra2005@yahoo.co [46] Chatterjee, T., Gupta, N., Choudhry, V.P., Behari, M., Saxena, R. and Ashraf, M.Z. (2013) Prediction of Ischemic Stroke in Young Indians: Is Thrombophilia Profiling a Way Ou t? Blood Coagulation & Fibrinolysis, 24, 449-453. http://dx.doi.org/10.1097/MBC.0b013e32835bfe21  P. Devabhaktuni et al. [47] James, A.H., Konkle, B.A. and Bauer, K.A. (2013) Prevention and Treatment of Venous Thromboembolism in Preg- nancy in Patients with Hereditary Antithrombin Deficiency. International Journal of Women’s Health, 5, 233-241. http://dx.doi.org/10.2147/IJWH.S43190 [48] Barsoum, M.K., Heit, J.A., Ashrani, A.A., Leibson, C.L., Petterson, T.M. and Bailey, K.R. (2010) Is Progestin an In- dependent Risk Factor for Incident Venous Throboembolism? A Population-Based Case-Control Study. Thrombosis Research, 126, 373-378. http://dx.doi.org/10.1016/j.thromres.2010.08.010 [49] WHO (2009) Medical Eligibility Criteria for Contraception. 4th Edition. http://whqlibdoc.who.int/publications/2010/9789241563888_eng.pdf [50] Dal, C.P., Quade, B.J., Neskey, D.M., Kleinman, M.S., Weremowicz, S. and Morton, C.C. (2003) Intravenou s Leiomyo- matosis Is Characterized by a Der (14)t(12;14)(q15;q24). Genes, Chromosomes and Cancer, 36, 205-206. http://dx.doi.org/10.1002/gcc.10159
|