G. W. LIU ET AL.
Copyright © 2011 SciRes. SS
71
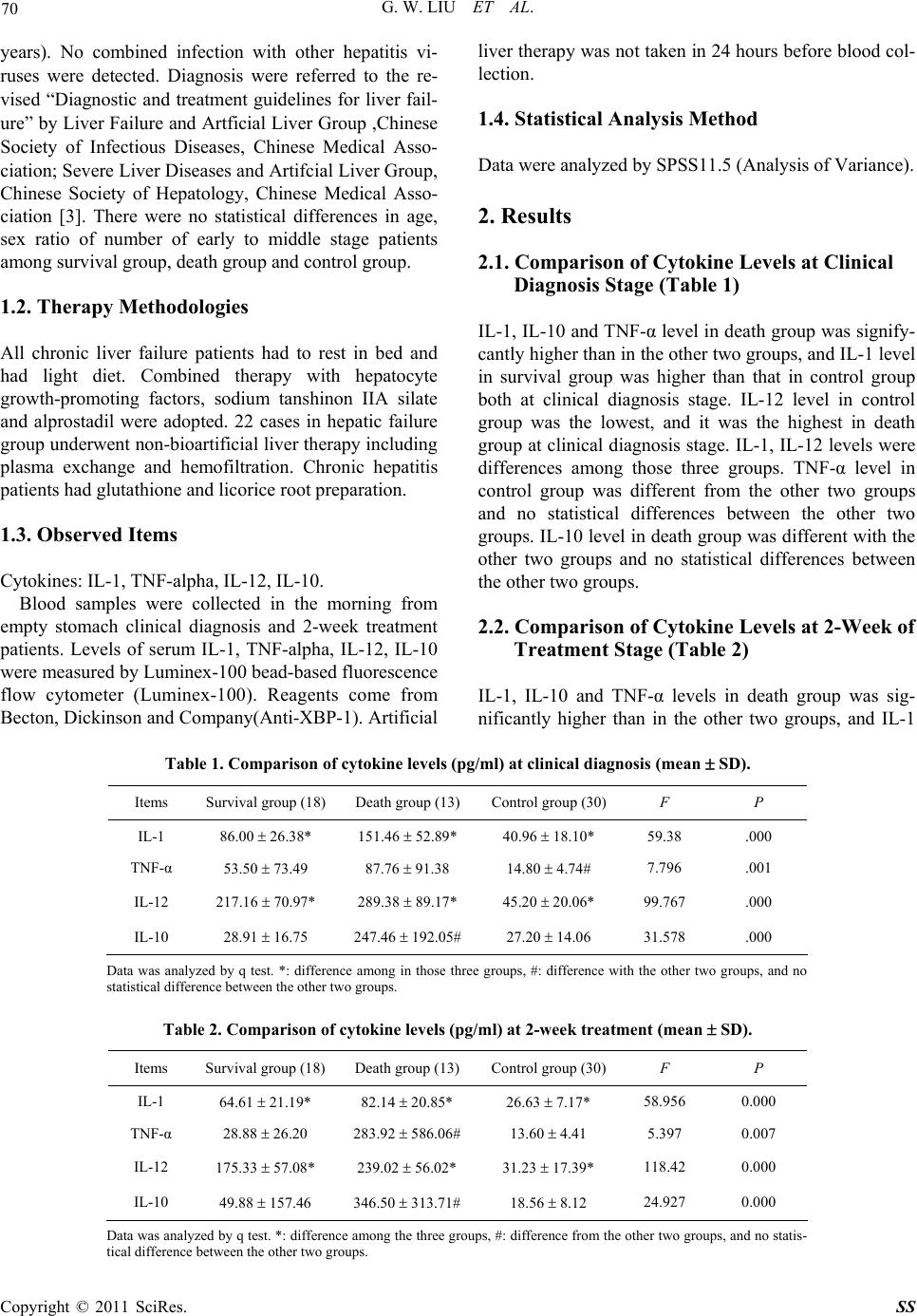
level in survival group was higher than in control group.
IL-12 level in control group was the lowest, and it was
the highest in death group after 2-week treatment. IL-1,
IL-12 level are difference among those three groups.
TNF-α and IL-10 level in death group were different from
the other two groups and no statistical difference be-
tween the other two groups. IL-1 level at clinical diagnosis
stage was higher than after 2-week treatment, both in
death group and survival group.
3. Discussion
IL-1 helps body to fight against pathogenic microorgan-
isms and it is also one of non-specific defensive factors.
The results of at clinical diagnosis and 2-week treatment
stages were shown IL-1 level in death group was signify-
cantly higher than in the other two groups meanwhile, it
was the lowest in control group both at clinical diagnosis
and 2-week treatment stages, which suggested IL-1
might reflect the degree of inflammatory reaction and
serve as important index for prognosis of severe hepatitis.
Nevertheless, with the progression of the disease, IL-1
level at clinical diagnosis stage was higher than after
2-week treatment, both in death group and survival group.
This result implied that IL-1 secretion was decreasing
while the progression of Liver failure, therefore, resultes
in compromising of immunity. Those effectors, the pos-
sible reason, could be generated by a number of immu-
nocytes upon activation in early stage of disease,
whereas those effectors were decreasing indirectly due to
the apoptosis of immunocytes in the last stage.
TNF-α has a variety of biological effects, it is the
important factor in causing liver damage [4]. The level of
TNF-α was not only reflecting the capability of resisting
viral infection, but also associated with the immuno-
pathological to damage hepatocytes. At clinical diagnosis
stage, TNF-α level in severe hepatitis patients was sig-
nificantly higher than in control group, whereas there
was no statistical differences between death group and
survival group. With disease progressing, TNF-α level
was remarkably increasing in death group but decreasing
in survival group. After 2-week treatment, it was obvi-
ously higher in death group than in survival group. It was
suggested that changes of TNF-α could be the index of
the prognostic assessment, and TNF-α also reflected the
inflammation severity. Hepatic necrosis was reflected by
excessively high level of TNF-alpha, it might be one of
the important reasons of death.
IL-10, an important anti-inflammatory cytokine, par-
ticipated in principal negative feedback regulation in-
cluding inhibiting the generation of the inflammatory
factor and the colony stimulating factor in one hand and
suppressed the anti-viral immunity of the body in the
other hand. In this study, it shown anti-inflammatory
cytokines in severe hepatitis patients of death group were
dramatically raise, but not significantly changed in sur-
vival group, which suggested the increasing of anti-in-
flammatory cytokines in severe hepatitis patients espe-
cially at the last stage was an indirect indicator of severe
inflammation. And the raise of cytokine level could be
the result in immunity decreasing. The immunity of pa-
tients who suffered from severe hepatitis might be varied
at different stages of disease. At early stage, the inflame-
matory cytokines were releasing, and there is no in-
creasing in non-inflammatory factors. If the disease had
been well controlled, anti-inflammatory factors would be
no longer increasing. Otherwise, they would be signify-
cantly increasing to prevent the body from excessive
immune attack. Simultaneously, the immunity of patients
was declined.
IL-12 level in death group was higher than in survival
group both at clinical diagnosis and 2-week treatment
stage, and it was the lowest factor in control group,
which suggested there was intensive reaction for elimi-
nating pathogen at beginning of severe hepatitis, espe-
cially in heavy disease patients.
IL-1 could be amplified by the biological effect of
TNF-α, which could aggravate hepatic necrosis. Under
normal physiological condition, TNF-α and IL-1 could
be cleared by the liver. However, in case of liver failure,
endotoxin could activate macrophages, which could im-
pair the liver’s capability of eliminating cytokines. Thus,
TNF-α and IL-1 were the directly factors to develop of
liver failure. In our study, IL-10 raising did not suppress
the IL-12 increasing. In this study, it had shown IL-10
raising might be caused by increasing of IL-12, it might
be a compensatory response, which might prevent body
from excessive immunological damage. In addition, the
results of IL-10 in our study was different from Yumoto
E results [5]. We need more samples for the further
study.
4. References
[1] H. Isoniemi, A. M. Koivusalo, H. Repo and et a1. “The
Effect of Albumin Dialysis on Cytokine Levels in Acute
Liver Failure and Need for Liver Transplantation,”
Transplantation Proceedings, Vol. 37, No. 2, 2005, pp.
1088-1090. doi:10.1016/j.transproceed.2004.11.060
[2] Tao Wen and Hao Wu, “Research Progress of Inter-
leukin-12 and Its Application in Management of HIV In-
fection,” Foreign Medical Sciences (Epidemiology
Lemology Fascicle), Vol. 30, No. 5, 2003, pp. 271-274.
[3] J. Clin Hepatol, “Diagnostic and treatment guidelines for
liver failure,” Vol. 9, No. 6, 2006.
[4] R. F. Schwabe and D. A. Brenner, “Mechanisms of Liver
Injury Tnf-Alpha-Induced Liver Injury: Role of IKK,