Paper Menu >>
Journal Menu >>
 Vol.3, No.3, 179-185 (2011) Health doi:10.4236/health.2011.33034 Copyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ Exploring the subjective burden of confidentiality among physicians in norway Løvseth Lise Tevik1*, Leiulfsrud Håkon2 1Department of Research and Development, St Olavs University Hospital, Trondheim and Institute of Neuroscience, Norwegian University of Science and Technology, Trondheim, Norway; *Co rreponding Author: lise.lovseth@ntnu.no 2Department of Sociology and Political Science, Norwegian University of Science and Technology, Trondheim, Norway. Received 25 January 2011; revised 7 February 2011; accepted 23 February 2011. ABSTRACT Background: Concern about protecting patient privacy is proposed to be a barrier for physic- cians to talk about emotional distress from their professional experiences. This makes it difficult for many physicians to utilize and fully benefit from different network of social support. The subjective burden of confidentiality is reported to be associated with physician’s health and wellbeing. Aims: To gain knowledge about fac- tors in the in personal and professional sphere that can be associated with the subjective bur- den of confidentialit y. Methods: Qualitative semi- structured interviews with 14 general practi- tioners and hospital physicians in Norway. Ex- amination of transcribed verbatim interviews using qualitative content analysis. Results: The subjective burden of confidentiality is likely linked with factors such as perception of pro- fessional role, social support from colleagues, partners and friends; size of patient population, organizational factors and work environment, and the overlap between personal and profess- sional relationships. Conclusions: Addressing the interaction of emotional demands and pa- tient confidentiality is important to study suc- cessful coping with distress from physician’s professional experiences. Keywords: Professional secrecy; doctors; ethics; work stress; social support; work en vir onment 1. INTRODUCTION Although physicians are educated and trained to be capable and mentally prepared to handle patient’s mis- fortune, it is inevitable that they can be emotionally af- fected by their patients. Situations that can cause emo- tional distress can range from one major traumatic event to several critical incidents over a short period of time [1,2], including everyday routine situations [3-5]. As exposure to emotional job stressors usually cannot be reduced, the physician’s ability to cope with emotional demands is i m po rt ant in orde r to prevent stress [6,7] . The most common method physicians apply to cope with emotional distress involve turning to others for support [8]. Previous research has confirmed that support from others is a critical resource to foster adjustment to dis- tressing events, and of considerable significance for people’s health and wellbeing [9]. A key assumption in research on stress and coping is that people centralize their own needs. However , in m any situations people must prioritize other people’s needs or other important personal and professional values and goals. Competing priorities in coping, such as concerns about own confidentiality [10,11] or the need to maintain or protect ones own or their in-group professional integ- rity [12,13], can act as a barrier to seek support from others. In addition, the concern about protecting other people’s privacy in terms of discretion and client confi- dentiality is also an important barrier for supp ort seeking in emergency- and human service professionals [14]. A recent cross-cultural study showed that about 30% of hospital physicians regarded patient confidentiality as a considerable barrier to seeking emotional support from their professio nal and person al network [1 5]. In this st udy, the interaction between emotional demands, patient con- fidentiality and coping was clearly associated with phy- sician’s health and wellbeing [15]. As concerns about patient’s privacy seem to be relevant for physicians coping with emotional distress from their professional experiences, it is interesting to gain knowl- edge how confidentiality mediates coping with emotional distress, and factors in their personal and professional sphere, which can be associated with the subjective bur- den of confidentiality. This includes an explicit focus upon physician’s coping with emotional distress from their professional experiences, and how they resolve  L. L. Tevik et al. / Health 3 (2011) 179-185 Copyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 180 these possible challenges in light of the norms and rules of patient confidentiality. We are here primary interested to reveal examples an d patterns in how patient confid en- tiality is practiced, which explain the current research design based upon in depth interviews of Norwegian physicians, rather than a quantitative approach. The quail- tative study supplements and supports more quantitative driven research on the role of patient confidentiality for professionals in emergency and human services [14,15]. 2. METHODS In-depth interviews were carried out in a sample of 14 practicing physicians working in two Norwegian health regions. Nine were general practitioners (GP), four were oncologist from a hospital with patients from the whole country, and one senior consultant was specialized in treatment of physicians with health problems. Partici- pants were recruited based on recommendations from their colleagues and superiors. Our concern was to ex- plore contrasting experiences among the ones inter- viewed. In order to do so it was important to have a mixed sample in terms of experience and ty p e o f me d i ca l p r a c- tice (Table 1). The interviews were conducted as semi structured in- dividual interviews with open-ended questions, and held in the physician’s office. The interviews lasted from 45 minutes to 3 hours, on aver age taking 1 – 1.5 hours. Par- ticipants were asked open-ended questions. Core con- cepts were pursued flexibly in the individual interviews, according to the topics that appeared most adequate during the conversation. The participants were asked to give a short summary o f their curren t position, edu cation and career as physician. The interview covered topics of emotional distress from their professional experiences, coping with distress and the ways in which confidentiality affected them in various situations at work and outside work. Phys icians were encouraged to speak freely and raise issues concerning confidentiality that were important to them, and to support their responses with examples. We avoided a focus on judgments of individual decisions as right or wrong practice of confidentiality [16]. The interviews were taped and transcribed, and then the interviewer and co-workers verified the transcriptions. In the analysis and coding of data, this study followed Miles and Huberman’s [17] qualitative research method. Two researchers separately coded the data, and the codes were later compared in order to reconcile discrepancies and reach consensus to ensure the validity of the inter- pretations made. Qualitative conten t analysis of text was conducted on several levels. Initially, we looked in detail at the transcript of each interview, starting with particular Table 1. Characteristics of int e rviewees. No. Gender Age Hospital Position* Location Patient population (N**) Head of dept/ med. office Partner’s occupation 1 M 50 No CMMO District 1’- 10’ Yes Psychologist 2 M 44 No CMMO District 1’- 10’ Yes Unknown 3 M 54 No GP City 10’- 200’ No Teacher 4 F 29 No GP City 1’- 10’ No Unknown 5 F 49 No GP City 1’- 10’ No Physician 6 M 48 No CMMO District 1’- 10’ Yes Physician 7 M 40 No GP District 10’- 200’ No Housewife 8 M 44 Yes SSC District 10’- 200’ Yes Nurse 9 M 52 No GP City 1’- 10’ No Nurse 10 M 50 Yes SSC City >4 500’ Yes Not physician 11 M 48 Yes SC City >4 500’ No Physician 12 M 54 Yes SC City >4 500’ Yes Physiotherapist 13 F 45 Yes SC City >4 500’ No Physician 14 M 40 No CMMO District < 1000 Yes Single *GP = General practiti oner/(S)SC = (Se ction) senior consultant/CMMO = Chief Munici pal medical officer. **numbers in thousand. 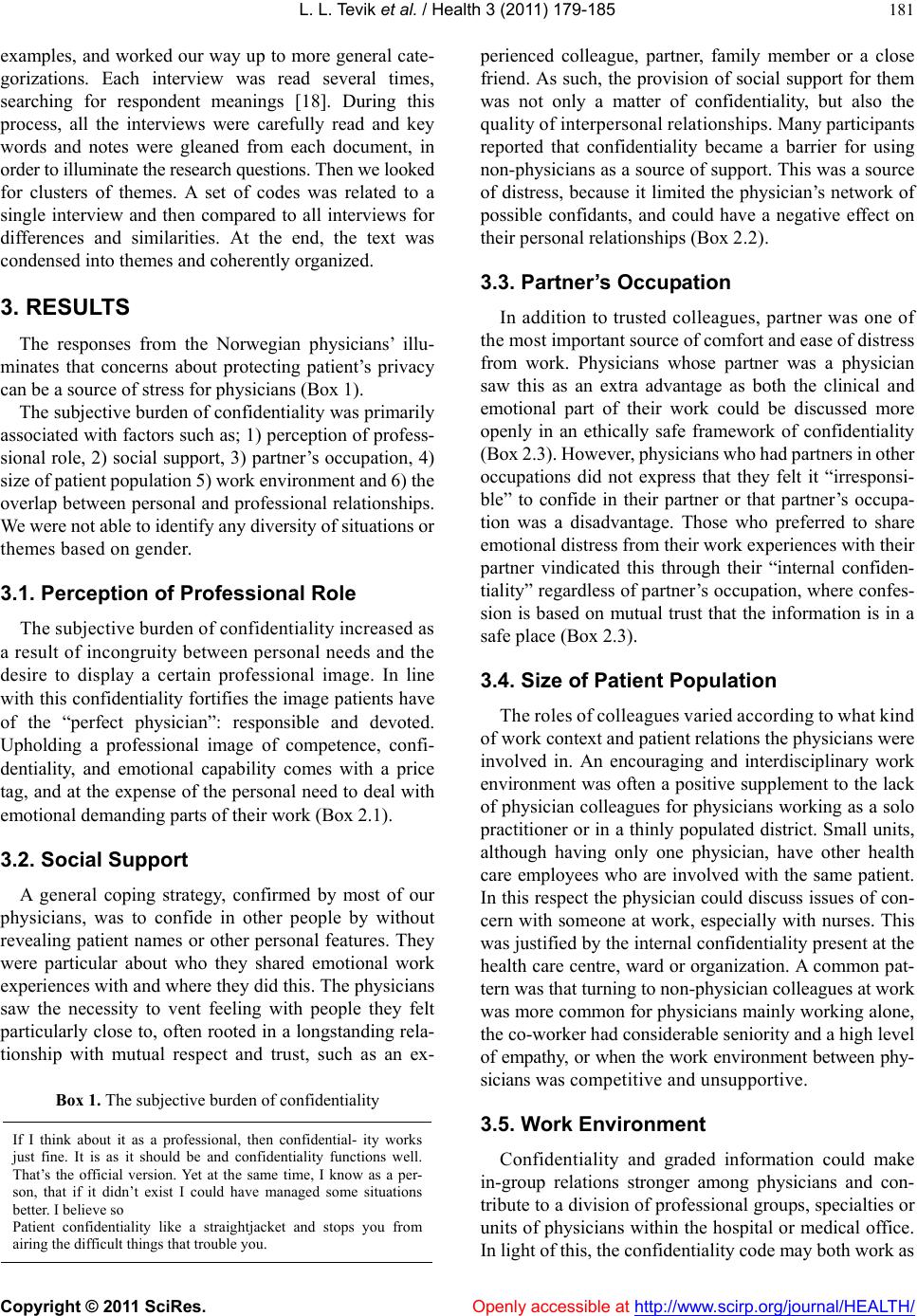 L. L. Tevik et al. / Health 3 (2011) 179-185 Copyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 181 examples, and worked our way up to more general cate- gorizations. Each interview was read several times, searching for respondent meanings [18]. During this process, all the interviews were carefully read and key words and notes were gleaned from each document, in order to illuminate the research questions. Then we looked for clusters of themes. A set of codes was related to a single interview and then compared to all interviews for differences and similarities. At the end, the text was condensed into themes and coherently organized. 3. RESULTS The responses from the Norwegian physicians’ illu- minates that concerns about protecting patient’s privacy can be a source of stress for physicians (Box 1) . The subjective burden of confidentiality was primarily associated with factors such as; 1) perception of profess- sional role, 2) social support, 3) partner’s occupation, 4) size of patient po pulat ion 5) work envi ronm ent a nd 6 ) the overlap between personal and professional relationships. We were not able to identify any diversity of situations or themes based on gender. 3.1. Perception of Professional Role The subjective burden of confidentiality increased as a result of incongruity between personal needs and the desire to display a certain professional image. In line with this confidentiality fortifies th e image patients have of the “perfect physician”: responsible and devoted. Upholding a professional image of competence, confi- dentiality, and emotional capability comes with a price tag, and at the expense of the personal need to deal with emotional demanding part s of their work (Box 2.1). 3.2. Social Support A general coping strategy, confirmed by most of our physicians, was to confide in other people by without revealing patient names or other personal features. They were particular about who they shared emotional work experiences with and where they did this. The physicians saw the necessity to vent feeling with people they felt particularly close to, often rooted in a longstanding rela- tionship with mutual respect and trust, such as an ex- Box 1. The subjective burden of confide ntiality If I think about it as a professional, then confidential- ity works just fine. It is as it should be and confidentiality functions well. That’s the official version. Yet at the same time, I know as a per- son, that if it didn’t exist I could have managed some situations better. I b e l ie v e s o Patient confidentiality like a straightjacket and stops you from airing the difficult t hi ngs th at trouble you. perienced colleague, partner, family member or a close friend. As such, the provision of social support for them was not only a matter of confidentiality, but also the quality of interpersonal relationships. Man y par t i c i pa n t s reported that confidentiality became a barrier for using non-physicians as a source of su pport. This was a sour ce of distress, because it limited the physician’s network of possible confidants, and could have a negative effect on their personal rel at i onships (Box 2.2). 3.3. Partner’s Occupation In addition to trusted colleagues, partner was one of the most important s ource of comfort and eas e o f dist re ss from work. Physicians whose partner was a physician saw this as an extra advantage as both the clinical and emotional part of their work could be discussed more openly in an ethically safe framework of confidentiality (Box 2.3 ). Howeve r , p hysicians who ha d partner s in othe r occupations did not express that they felt it “irresponsi- ble” to confide in their partner or that partner’s occupa- tion was a disadvantage. Those who preferred to share emotional distress from their work experiences with their partner vindicated this through their “internal confiden- tiality” regardless of partner’s occupation, where confes- sion is based on mutual trust that the information is in a safe place (Box 2.3). 3.4. Size of Patient Population The roles of colleagues varied according to what kind of work context and pat i ent relations the physicians were involved in. An encouraging and interdisciplinary work environment was often a positive supplement to the lack of physician colleagu es for physicians working as a solo practitioner or in a thinly populated district. Small un its, although having only one physician, have other health care employees who are involved with the same patient. In this respect the physician could discuss issues of con- cern with someone at work, especially with nurses. This was justified by the internal confid entiality presen t at the health care centre, ward or organization. A common pat- tern was that turning to non-physician colleagues at work was more common for physicians mainly working alone, the co-worker had co nsiderable senio rit y an d a hi g h level of empathy, or when the work environment between phy- sicians was competitive and unsupportive. 3.5. Work Environment Confidentiality and graded information could make in-group relations stronger among physicians and con- tribute to a divisio n of pro fession al groups, sp ecialties or units of physicians within the ho spital or medical office. In light of this, the confidentiality code may both work as  L. L. Tevik et al. / Health 3 (2011) 179-185 Copyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 182 a factor to maintain professional integrity, as well as a stressor and barrier for seeking social support with non-physicians. This was particularly evident among the physicians work ing in hospitals. Even though the climate between physician co-workers was not good (Box 2.4), many felt they could not go beyond professional “bor- ders” and talk to non-physician c o-workers. The realization that graded information might create a hierarchy and different in-group relations at the work place was compensated by creating alternative and less hierarchical modes of collaboration between physicians and non-physicians (Box 2.4). The extended network of possible confidants appears to have made it easier to share demanding work experiences with co-workers they valued and relied on regardless of the co-workers pro- fession. An important issue related to coping with emo- tional distress and confidentiality was the absence or presence of forums debriefing at the workplace. Such forums were according to those interviewed important for managing stressful situation s in an eth ically safe manner. These forums, informal and formal, were typically a result of the combination of work environment, organ- izational structure and personal initiative from seniors at the ward or health care centre. Although a formal forum existed in the quality system of the organization, most often physicians or co-workers used informal forums, such as Monday morning coffee breaks, staff meetings and lunch or private conversations between two physic- cians. These forums were not regarded as loose talk about patients, b ut describe d as an adv ice seeki ng sit uation held with respect for patients and confidentiality (Box 2.4). 3.6. The Overlap between Personal and Professional Relationships Privacy may be compromised when professional rel- tionships are interwoven with personal ones (Box 2.5). Physicians that worked and live within a small commu- nity faced situations where they had to be aware of con- fidentiality in interpersonal relationships. The GP’ s in the small rural practice said that having friends and col- leagues as patients was almost a weekly occurrence. Though, also physicians working in larger communities and hospitals faced these situations when treating col- leagues or members of a social group they belonged to. Younger physicians had not yet worked up a pool of patients that made confidentiality as challenging in in- terpersonal relationships in this regard. As a “newcomer” they did not know many people in their community. This was perceived as an advantage in order to avoid emo- tional connection with patients or distress by identifica- tion with patient’s life status. The need to keep profess- sional and personal relationships separate was also the reason why many physicians preferred to live in their neighbor municipal or district than the one they worked in. The amount of personal information the physician found comfortable and appropriate to know about people they knew set the premise for these kinds of consultations and encounters. Some physicians pre- ferred to completely separa ting the roles by refusing to treat people they knew well. Others did not have this strict division between the private and professional. However, the extent in which they treated people was limited. Some chose to only write out prescriptions, treat minor illness, perform superficial examinations and refer people to proper treatment/skilled clinicians. Some physicians drew the line between physical and psychological/psychiatric issues, and did not assist people with issues that had great emotional impact such as sexual issues, family crisis, suicide attempts and such. Still others had no separation between someone they knew a nd a ny oth er pat ie nt; they treated them equally regardless of the patient’s problem. When communication in social situations became a clinical encounter or addressed medical concerns, the physicians often used confidentiality as a tool to ac- tively force the encounter into a professional rela- tionship or setting. In these situations, confidentiality became a buffer of potential relationship stress; it regulated how the professional role came forward in a private setting in a manner that protected the integrity of both parties an d their relationship in the future. They always ensured that the consultation was conducted in their medical office. Or they explicitly specified that they are in the role of physician during the consul tation (Box 2.5). This study may extend our understanding on the relationship between protection of patient’s privacy and physicians coping with work related emotional distress. The results from the interviews with physic- cians suggest that organizational, professional and personal factors, which reinforce one another, may contribute to the subjective burden of confidentiality. For example, a hospital ward with a hierarchic struc- ture and unsupportive climate might have a different impact on this matter than a supportive work envi- ronment with a network of consistent boundaries re- garding the psychosocial work climate. This is in line with previous research where physicians are shown to have different attitudes to and practice of confidenti- ality [19,20], their professional rol e [21,22] and c oping strategies used to deal with ethical [23,24] and emo- tional [25] discomfort in their work. Based on the current results, these factors are likely to be associated with how physician manages emotionally-char ged work situations and confi de nt iality.  L. L. Tevik et al. / Health 3 (2011) 179-185 Copyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 183 Box 2. Factors associated with the subjective burden of patient confidentiality. 2.1 Professional role Confidentiality causes one to become an individualist. One must give the impression of being present and complete secrecy of all information- and because of this, it is important to maintain an im pression that information is not easily exchange between us doctors [No.1] Confidentiality is the problem; it is so strong and important that it hinders debriefing because of fear of showing weakness in a profession that is supposed to be “elite” [No. 6] One also has professional pride in that information should be kept to oneself [No. 8] 2.2 Social support Because of confidentiality, I primarily rely on my colleagues, perhaps more so than my partner [No. 5]. I don’t usually discuss concrete situations from work at home. One main reason for this is confidentialit y. My partner has said that it puts distance between us. But there is something about confidentiality…it happens quite fast that you’ve suddenly said a little something. It’s much easier to say nothing at all about your professional experiences [No. 10]. Most often you have a few people you feel particularly close to. And I have mine. It does not have to be a physician. It is more personal, and is a ma tte r of trust and personal chemistry [No. 10] 2.3 Partners occupation My wife is a nurse, and I do not believe that I violate confidentiality when I talk to her [No 9]. Confidentiality limits the kind of issues you bring at home. However, my partner works in the health care system. This makes it easier [No. 9] Though I can speak with my colleagues, I be lieve it is common to speak with your part ner. At least if yo ur par tner is a physician. We have an internal confidentiality, were I can share confidential information about patients, and know that it is in a safe place. It is probably not legal at all [No.11] 2.4 Work e nvironment It is a bit problematic to use other co-workers as confidants. We have some of the traditional separation between physicians and nurses. I feel that to a certain extent I have to maintain loyalty to the physicians and not take the nurses into confidence in regard to how much information I give. That’ s the way it is, it’ s like an unwritten rule her e [No. 10] Of course the medical meetings between doctors are important. However , because the house staff is a l arge part of the medical centre, it should not be a difference between us. They perform many clinical functions and have much knowledge about the patients. Often it is th e same patients that are challenging for us doctor s, as it is for them [No.5] It is more important to emphasize the ward and that those who work here is a unit. Particularly because we are exposed to the type of cases we have here. I mean, it becomes wrong if I constantl y emphasize [a hierar chy] that I am a senior consultant, and you a resident, next a poor intern, after that a nurse and then an enrolled nurse. Of course I have the main responsibility, but it is not necessary to demonstrate a visible power in the ward through confidentiality and rank. Everyone know their tasks, and all serve the same pur pose; working together with in the best interest for the patient. And the enjo yment and challenges we experience are som ething that we are going to share [No. 12] I think it’s important to have a place where you can be together and laugh about the frustration you have about patients. I don’t feel that confidentiality is a barrier to that. When I go to a colleague and talk about little things that happen, it’s between us. That is a freedom we take [No.6] 2.5 Personal and professional relationships Confidentiality complicates my life. In social situations it complicates my life. In professional situations I think it is easier to handle [No.3] As we have a more personal relationship with patients as general practitioners we place a major importance to ensure confidentiality [No. 1] In contrast to hospital physicians who focus more on “cases” that lays along the hospital beds. I think this personal relationship facilitates increased awareness on confidentiality among general practitioners than hospital physicians [No.1] Confidentiality regarding family and friends is difficult - incredibly difficult. Close friends who have problems. There I sit at a party with them and maybe before I sat and spoke with them about their worst life trauma [No. 3] When they [friends] come to my office, they see me more as a physician. If they visit my home and we are chatting at the kitchen table, then in this situation I am talking with them as a friend. I think this makes them feel safe as well. There is something to learning how to separate the private and the professional realms, you know. You will come into some problems regarding confidentiality if everything gets mixed together [No.5] There isn’t as much leeway for how to build a friendship. Because I have information that I don’t want to have between us, but it is there anyway [No.1] 4. DISCUSSION The present results indicate that a positive work environment alleviated the subjective burden of con- fidentiality. In addition, multidisciplinary teams with good, open c omm unicat ion provide a f orum for shared experience as well as shared knowledge and informa- tion. Interestingly, participation in meetings to discuss stressful work situations seemed to be helping to vent feelings both in a personal, and ethical, suitable man- ner. To b u il d a c om m o n ex pe r ie nc e b as e m ay el im i na te the need for detailed information in daily communica- tion with fellow workers as the emotional reaction be- comes readily recognizable without it [26]. This might  L. L. Tevik et al. / Health 3 (2011) 179-185 Copyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 184 counteract the subjective burden of confidentiality. Confidentiality was also perceived as a tool that pro- tects the physicians from possible relationship distress. Interweave bet ween personal and professiona l spheres for physicians have received increased attention the last decade [27,28]. Rourke and his associates have focused on boundary issues that may evolve due to treating own family members and friends [29]. All physicians, re- gardless of specialization, face such situations from time to time; though being a physician in a small community pose more frequent and proximal interpersonal chal- lenges in this regard. Miedema, Easley, Fortin, Hamilton and Tatemichi’s [30] study on how the trespassing of patients onto the physicians’ pe rsonal live in small towns and rural communities, illustrate this issue. Our study shows that the physicians used confidentiality as a tool to force such personal encounters into a professional setting in order to protect both parties integrity. The participants in this study represent a selected sample which might have been more reflective than the average physician and more willing to expose personal demanding situations and/ or situations where confiden- tiality as a norm of behavior has been compromised. The point of situations and themes that came up in the inter- views with the GPs,’ corresponded with the hospital physicians’. We have no reason to believe that the basis for the experiences of those who participated in this study to differ from those of their colleagues. Tough their willingness to make these experiences explicit may be a deviation fr om the general populat ion of physicians. M ost of the interviewed had a long work experience and in depth thoughts about the topics addressed. The disad- vantage of this kind of sample is of course that we might have missed out interesting dilemmas among junior phy- sicians. This said, when the physicians were asked to recall particular matters as inexperienced physicians, none did mention any previous experiences were the role as a subordinate was a problem in this regard. They rather focused on the importance of finding a trusted friend, preferably a fellow colleague to share stressful work experiences with, regardless of position or experience. The sample is over-representative for men. This reflects the proportion of GPs and oncologists in Norway where the majority is male (Statistics, The Norwegian Medical association, 2009). Interestingly we have not been able to track any systematic gender differences in the topic ad- dressed by the participants. Some of the male physician believed that female colleagues would find confidential- ity more c hallengi ng under t he ass umpt ion that wom en i n general prefer to share their emotions and seeks support more than m en. We ha ve not found any s upport f or this i n the current study or in correspondent research [14 ,15]. When the respondents in our study report that inter- professional relationships and confidentiality are crucial factors for inhibition and seeking emotional support, it is important that the organization facilitate a communica- tion atmosphere that address both the technical and emo- tional parts of medicine. In addition, that experienced physicians t ake the lead in promoting pr ofessional cha nge on this matter. An advisory service from skilled seniors might create a competence beyond the medical and tech- nical aspects of the medical profession. 5. ACKNOWLEDGEMENTS We are grateful to the physicians who participated in this study. An extended and special thanks to Olaf Gjerløw Aasland, head of the Research Institute, Norwegian Medical Association for contribution to the conceptual model. We also greatly appreciate constructive com- ments of the manuscripts done by pr ofessor/head of dep artme nt Olav M Linaker and associate professors Ismail Cüneyt Güzey at AFFU and Valentina Cabrol Iversen at St Olavs Hospital. REFERENCES [1] Baverstock A, Finlay F. What can we learn from the experiences of consultants around the time of a child’s death? Child Care Health Dev 2008; 34 (6):732-9. doi:10.1111/j.1365-2214.2008.00875.x [2] Mandell F, Mcclain M, Reece RM. Sudden and Unex- pected Death - the Pediatricians Response. Am J Dis Child 1987; 141 (7):748-50. [3] Vegni E, Mauri E, Moja EA. Stories from doctors of patients with pain. A qualitative research on the physic- cians’ perspective. Support Care Cancer 2005; 13 (1): 18-25. doi:10.1007/s00520-004-0714-2 [4] Shanafelt T, Adjei A, Meyskens FL. When your favorite patient relapses: Physician grief and well-being in the practice of oncology. J Clin Oncol 2003; 21 (13):2616-9. doi:10.1200/JCO.2003.06.075 [5] Elder N, Ricer R, Tobias B. How respected family physic- cians manage difficult patient encounters. J Am Board Fam Med 2006; 19 (6):533-41. doi:10.3122/jabfm.19.6.533 [6] Hobfoll SE. Conservation of Resources - A New Attempt at Conceptualizing Stress. Am Psychol 1989; 44 (3): 513- 24. doi:10.1037/0003-066X.44.3.513 [7] Karasek R, Theorell T. Healthy work. Stress, productivity, and the reconstruction of working life. New York: Basic Books 1990. [8] Wallace JE, Lemaire J. On physician well being - You’ll get by with a little help from your friends. Soc Sci Med 2007; 64 (12):2565-77. doi:10.1016/j.socscimed.2007.03.016 [9] Cohen S, Syme SL. Social support and health. Orlando, Fla: Academic Press 1985. [10] Kay M, Mitchell G, Clavarino A, et al. Doctors as pa- tients: a systematic review of doctors’ health access and the barriers they experience. Br J Gen Pract 2008; 58 (552): 501-8. doi:10.3399/bjgp08X319486 [11] Davidson SK, Schattner PL. Doctors’ health-seeking be- haviour: a questionnaire survey. Med J Aust 2003; 179  L. L. Tevik et al. / Health 3 (2011) 179-185 Copyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 185 (6):302-5. [12] Engelskjön N. The tradition of the physician’s professional ethics. From Hippocrates to the ethical rules of physic- cians of the Norwegian medical association. In: Olsen BO, Larsen Ø, eds. The Shaping of a profession. Physi- cians in Norway, past and present. Canton, Mass: Sci- ence History Publications 1996:507-18. [13] Øyen E. Trend Report 1. The Social Functions of Confi- dentiality. Current Sociol 1982; 30 (2):1-37. [14] Lövseth LT, Aasland OG. Confidentiality as a Barrier to Social Support: A Cross-Sectional Study of Norwegian Emergency and Human Service Workers. Int J Stress Manage 2010; 17 (3):214-31. doi:10.1037/a0018904 [15] Lövseth LT, Aasland OG, Fridner A, et al. Confidential- ity and Physicians’ Health. A Cross-sectional Study of University Hospital Physicians in Four European Cities (the HOUPE-study). J Occup Health 2010; 52 (5): 263- 71. doi:10.1539/joh.L10014 [16] Kvale S. The Qualitative Research Interview - A Phe- nomenological and A Hermeneutical Mode of Under- standing. J Phenomenol Psychol 1983; 14 (2):171-96. doi:10.1163/156916283X00090 [17] Miles MB, Huberman AM. Qualitative data analysis. An expanded sourcebook. Thousand Oaks, Calif: Sage 1994. [18] Smith JA. Qualitative psychology. A practical guide to research methods. London: Sage 2008. [19] Lako CJ, Lindenthal JJ. The Management of Confidenti- ality in General Medical-Practice - A Comparative-Study in the USA and the Netherlands. Soc Sci Med 1991; 32 (2):153-7. doi:10.1016/0277-9536(91)90055-H [20] Elger BS. Factors influencing attitudes towards medical confidentiality among Swiss physicians. J Med Ethics 2009; 35 (8):517-24. doi:10.1136/jme.2009.029546 [21] Voltmer E, Kieschke U, Spahn C. Work-related behave- iour and experience patterns of physicians compared to other professions. Swiss Medical Weekly 2007; 137 (31-32):448-53. [22] Aase M, Nordrehaug JE, Malterud K. "If you cannot tolerate that risk, you should never become a physician’’: a qualitative study about existential experiences among physicians. J Med Ethics 2008; 34 (11):767-71. doi:10.1136/jme.2007.023275 [23] Duval G, Clarridge B, Gensler G, et al. A nationa l surv ey of US Internists’ experiences with ethical dilemmas and ethics consultation. J Gen Intern Med 2004; 19 (3): 251-8. doi:10.1111/j.1525-1497.2004.21238.x [24] Hurst SA, Perrier A, Pegoraro R, et al. Ethical difficult- ties in clinical practice: experiences of European doctors. J Med Ethics 20 07; 33 (1):51-7. doi:10.1136/jme.2005.014266 [25] Larsson J, Rosenqvist U, Holmstrom I. Enjoying work or burdened by it? How anaesthetists experience and handle difficulties at work: a qualitative study. Br J Anaesth 2007; 99 (4):493-9. doi:10.1093/bja/aem233 [26] Thoits PA. Social support as coping assistance. J Consult Clin Psychol 1986; 54 (4):416-23. doi:10.1037/0022-006X.54.4.416 [27] Farber NJ, Novack DH, Silverstein J, et al. Physicians’ experiences with patients who transgress boundaries. J Gen Intern Med 2000; 15 (11):770-5. doi:10.1046/j.1525-1497.2000.90734.x [28] Spickard WA, Swiggart WH, Manley GT, et al. A con- tinuing medical education approach to improve sexual boundaries of physicians. Bull Menninger Clin 2008; 72 (1):38-53. doi:10.1521/bumc.2008.72.1.38 [29] Rourke JTB, Smith LFP, Brown JB. Patients, Friends, and Relationship Boundaries. Can Fam Physician 1993; 39:2557-64. [30] Miedema B, Easley J, Fortin P, et al. Crossing boundarie s Family physicians’ struggles to protect their private lives. Can Fam Physician 2009; 55 (3):286-7. |