A. D. LEVA ET AL.
Copyright © 2011 SciRes. IIM
61
It must be pointed out that the resource utilization ap-
plies to the particular care process we have studied and
not to the whole activity executed in the OPDept. Indeed
if we insert in the process any other kind of chemother-
apy, all resources turn out to be heavily used.
In analyzing simulation results it must be pointed out
that the main problem is related to the long waiting times
to obtain drugs from the Pharmacy and exams results of
analysis from the Laboratory. Let us analyze these prob-
lems separately.
3.1.1. Laboratory
Waiting time to receive results from the Laboratory de-
pends on three factors:
• Test-tube labeling.
• Test-tube transport from OPDept to Laboratory.
• Test result availability notification.
Test-tube labeling is a process that influ ences the wait-
ing time to obtain exam results. Indeed, bad printing of
the label or its wrong positioning on test-tube results in
the arrest of the analysis automated line. This requires
intervention by a technician to resume the line. In order
to prevent this event, robots have been developed to pro-
duce test-tubes in which the labels are correctly printed
and positioned.
Test-tubes are currently transported from OPDept to
Laboratory by auxiliary staff. This process is time con-
suming (it requires about 30 minutes) and this is a rele-
vant part of the total waiting time. A good solution to
this problem would be the employment of a Pneumatic
Mail tube system in substitution of the auxiliary staff;
this would result in a considerable save in transport time.
Regarding test result no tification, at presen t doctors, in
order to know test results, have to repeatedly check the
result availability with queries to a software application.
A possible solution would be the use of acoustic and
visual signals to let the doctors know as soon as test re-
sults are ready. This way, waiting time would be reduced
from the current 26-35 minutes to about 4-5 minutes.
3.1.2. Pharmacy
Waiting time to receive drugs depends on two factors:
• Transmission of therapy requests.
• Drug preparation and transport.
At present, doctors have to insert a therapy request
into the local Information System, print it and then send
it by fax to the Pharmacy. It might h app en th at th e doctor
decides to make some changes to a therapy on the base
of the patient’s condition. Some times the doctor intro-
duces these changes by sending on paper and not using
the information system. Since the paper form is the only
request form officially accepted in the Pharmacy, the
pharmacist has to add further effort to his job, and intro-
duces new manual activities in the procedure. This also
introduces in the process an element of risk! A possible
solution would be the use of a new certified computer-
ized procedure in place of the fax procedure.
The second factor which influences the waiting time
depends on the time that is necessary to prepare the drug
and to transport it by means of an auxiliary staff. We
have measured it takes about 50 minutes to obtain the
drug. A possible corrective action would be the use of
the same drug, but administered by oral way instead of
intravenous way. Since the OPdept can manage the oral
chemotherapy in a local warehouse, inquiry, preparation
and delivery times can be eliminated.
3.2. “What-If” Analysis and Reorganization
Starting from the current “Oral administration” process
we defined two reo rganizatio n sce narios:
• Scenario A: In this scenario, the oral administra-
tion of the drug has bee n intr od uced.
• Scenario B: In addition to the oral administration,
the corrective actions described above (i.e. the use
of a robot for test-tube labeling, the pneumatic mail
test-tube system and the certified computerized
system to advice doctors) have been introduced in
the model.
In the Scenario A, the oral administration of Navelbina
implies a significant variation of the interactions between
OPDept and Pharmacy. The OPDept has to manage a
local warehouse with the oral chemotherapy (Navelbina)
supplied by the Pharmacy, but all the steps of drug re-
quest, drug preparation and waiting time, and all the
backup procedures necessary in case of faulty delivery
can be removed. The doctor as soon as receives test re-
sults can deliver the oral chemotherapy to the patient.
The oral administration can be conducted according to
the care pathway illustrated in Figure 3. The new activi-
ties, Fix therapy and Oral administration, are illustrated
in Table 4.
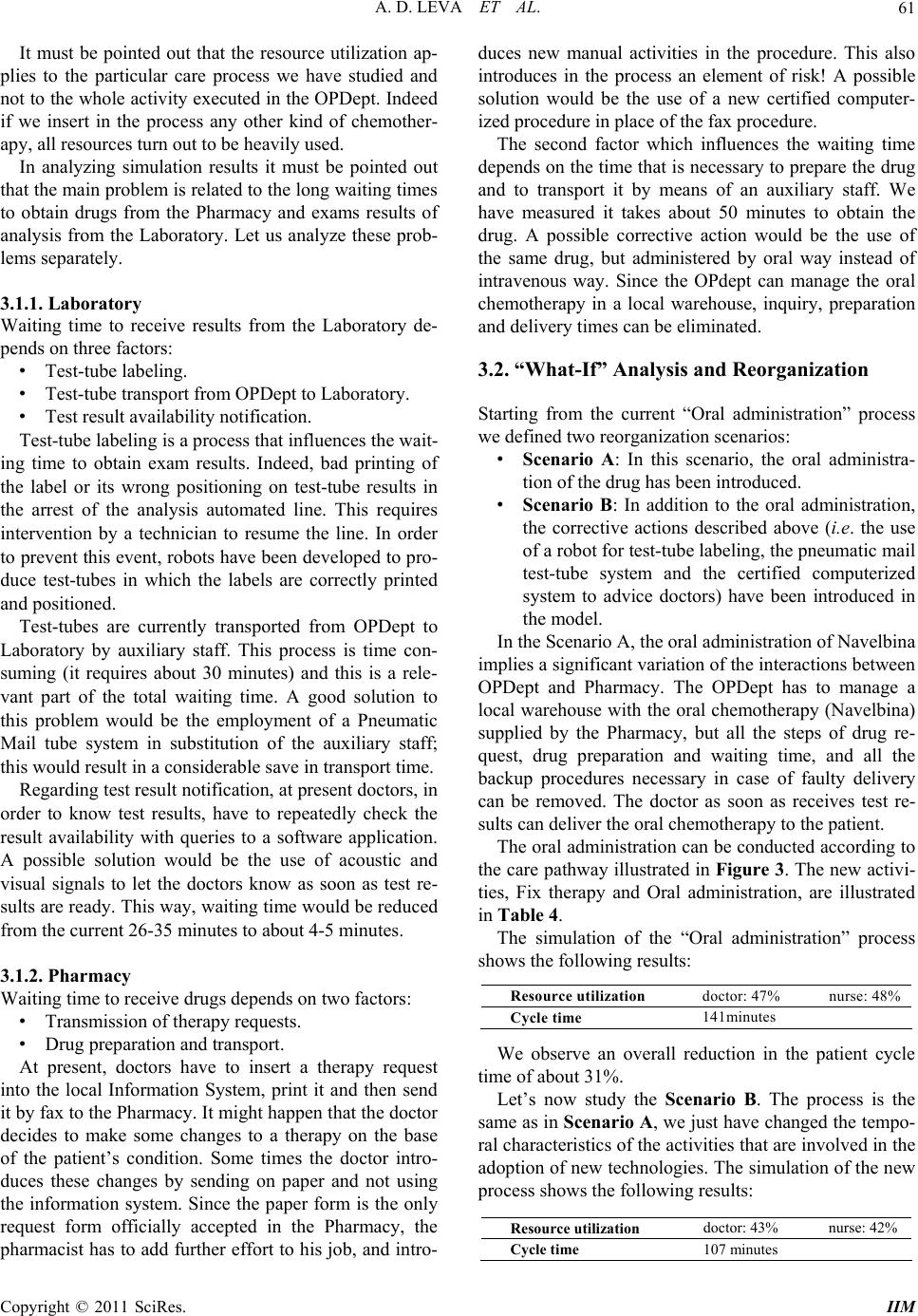
The simulation of the “Oral administration” process
shows the following results:
Resource utilization doctor: 47% nurse: 48%
Cycle time 141minutes
We observe an overall reduction in the patient cycle
time of about 31%.
Let’s now study the Scenario B. The process is the
same as in Scenario A, we just have changed the tempo-
ral characteristics of the activities that are involved in the
adoption of new technologies. The simulation of the new
process shows the following results:
Resource utilization docto r: 43% nurse: 42%
Cycle time 107 minutes