Open Journal of Nephrology, 2013, 3, 220-222
Published Online December 2013 (http://www.scirp.org/journal/ojneph)
http://dx.doi.org/10.4236/ojneph.2013.34038
Open Access OJNeph
Atypical Presentation of Classical Ba rtter Syndro m e as a
Case of Chronic Diarrhea and Failure to Thrive*
Anil Kumar Mohanty, Deepti Damayanty Pradhan, Bijay Kumar Meher, Pradeep Sivraj
Department of Paediatrics, Sardar Vallavbhai Patel Post Graduate Institute of Paediatrics (SCB Medical College), Cuttack, India
Email: bkmeher187@yahoo.co.in
Received November 20, 2013; revised December 10, 2013; accepted December 20, 2013
Copyright © 2013 Anil Kumar Mohanty et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
The classical Bartter syndrome is an uncommon tubular disorder of autosomal recessive inheritance, characterized by
early childhood onset of polyuria, polydipsia, vomiting, dehydration, constipation and salt craving habit. The long-term
outlook for patients with Bartter syndrome is not certain. If not properly treated, it may lead to failure to thrive and
growth retardation. We herein report a case of 18-month-old girl child who presented chronic diarrhea and failure to
thrive and then was diagnosed as a case of classical Bartter syndrome. She was successfully treated with potassium sup-
plementation and ibuprofen therapy.
Keywords: Bartter Syndrome; Chronic Diarrhea; Ibuprofen Therapy
1. Introduction
Bartter Syndrome first described in 1960 but, over the
years several phenotypic and genotypic variants of
original description of Bartter syndrome have been iden-
tified [1,2]. The classical Bartter syndrome (BS) is char-
acterized by early childhood onset with polyuria, poly-
dipsia, vomiting, constipation, salt craving, severe dehy-
dration, failure to thrive and growth retardation [3]. It is
an uncommon tubular disorder, characterized by meta-
bolic alkalosis, hyponatremia, hypokalemia, hypochlo-
remia, with hyper-reninemia and hyperaldosteronemia,
and normal or low blood pressure associated with in-
creased loss of sodium, potassium, calcium and chloride
in the urine [4].
2. Case Report
An 18-month-old female child born out of non-consan-
guineous marriage presented with history of vomiting,
poor feeding, on and off low grade fever, loose motion
and weight loss for 3 months. Vomiting was projectile,
non-bilious, and 6 - 8 times per day. The loose motion
was watery sometimes mucoid 6 - 8 times daily and was
continuing for last 3 months and was hospitalized in local
hospital twice for dehydration but loose motion did not
relieved by treatment. There was no history of decrease
in urination. This child was 4th order, term normal vagi-
nal delivery, birth weight being 2800 gm with uneventful
perinatal period. Baby was on exclusive breast fed up to
6 months of age and thereafter was on home based cereal
diet. Developmental milestones were normal till about 15
months of age then unable to stand and walk and started
crawling. In the sibling history, 1st male child died at 4
months and 2nd female child died at 6 months due to un-
known reasons, 3rd female child was 5 years old and do-
ing well.
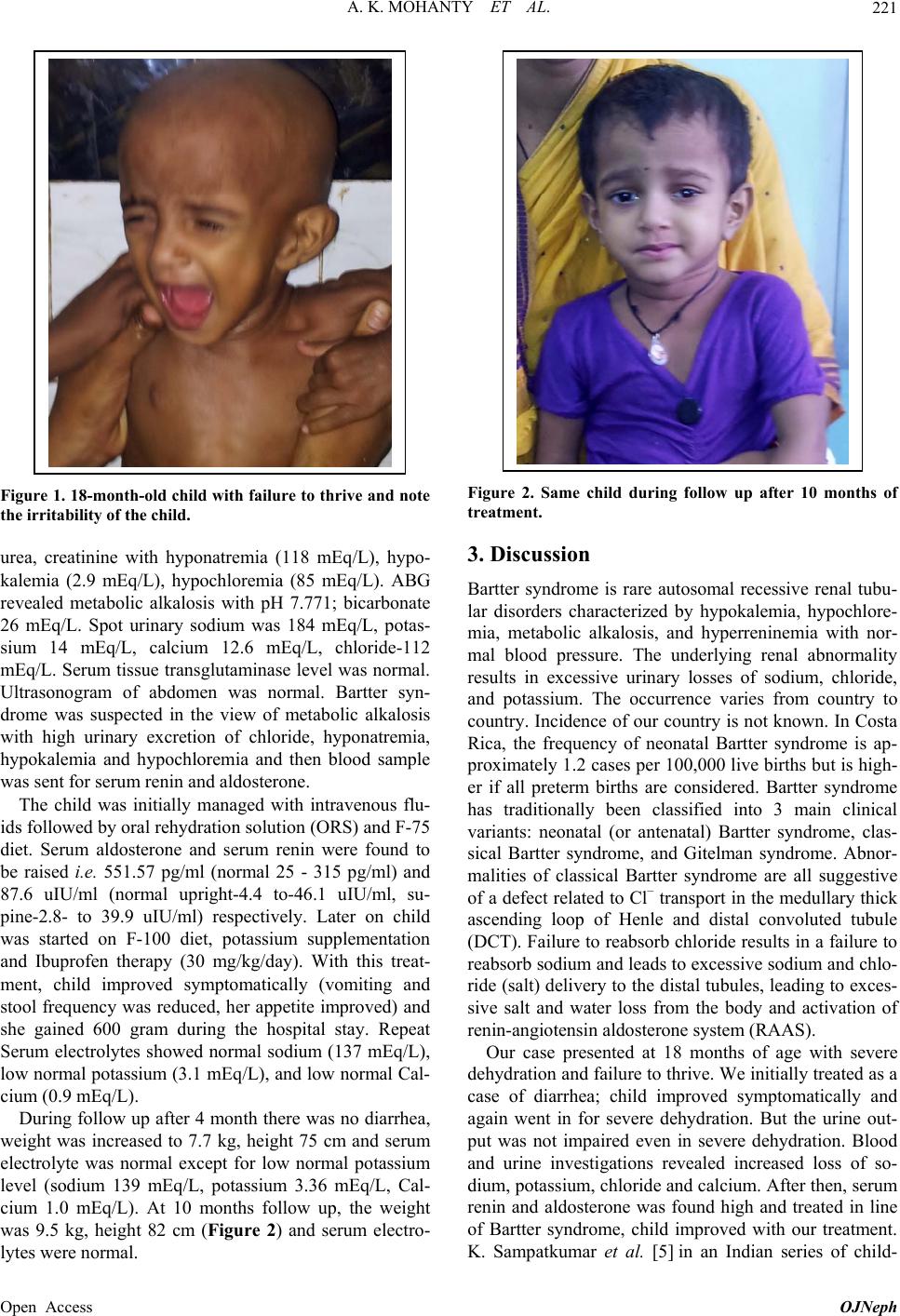
On examination, at admission, the patient was cachec-
tic, afebrile, lethargic, severely dehydrated, having ta-
chycardia, tachypnea, hypotension, weight 5.5 kg, (pre-
vious documented weight at 6 months was 6.5 kg and at
1 year was 8 kg.) without stunting, head circumference
45 cm, MAC-10 cm with US/LS ratio of 1.4. (Figure 1)
She was pale, without having lymphadenopathy, jaundice,
cyanosis, clubbing or edema with systemic examinations
being normal. Clinical diagnosis at admission was chro-
nic diarrhea with failure to thrive.
On investigation, microcytic hypochromic anemia
with normal erythrocyte sedimentation rate (ESR) and
normoglycemia, without any features of infection (total
leucocyte counts, C-reactive protein, urine microscopy
including culture were normal). Stool examination re-
vealed no red blood cells, pus cell, parasites, fat globules
and normal level of reducing sugars. Serum albumin was
3 gm/dL. Renal function test revealed normal serum-
*Funding: none; Conflicting interest: none.