Towards Developing Communication Strategies for HIV/AIDS Control among the Scheduled Tribes
and Scheduled Castes Women in Three Northeastern States of India
376
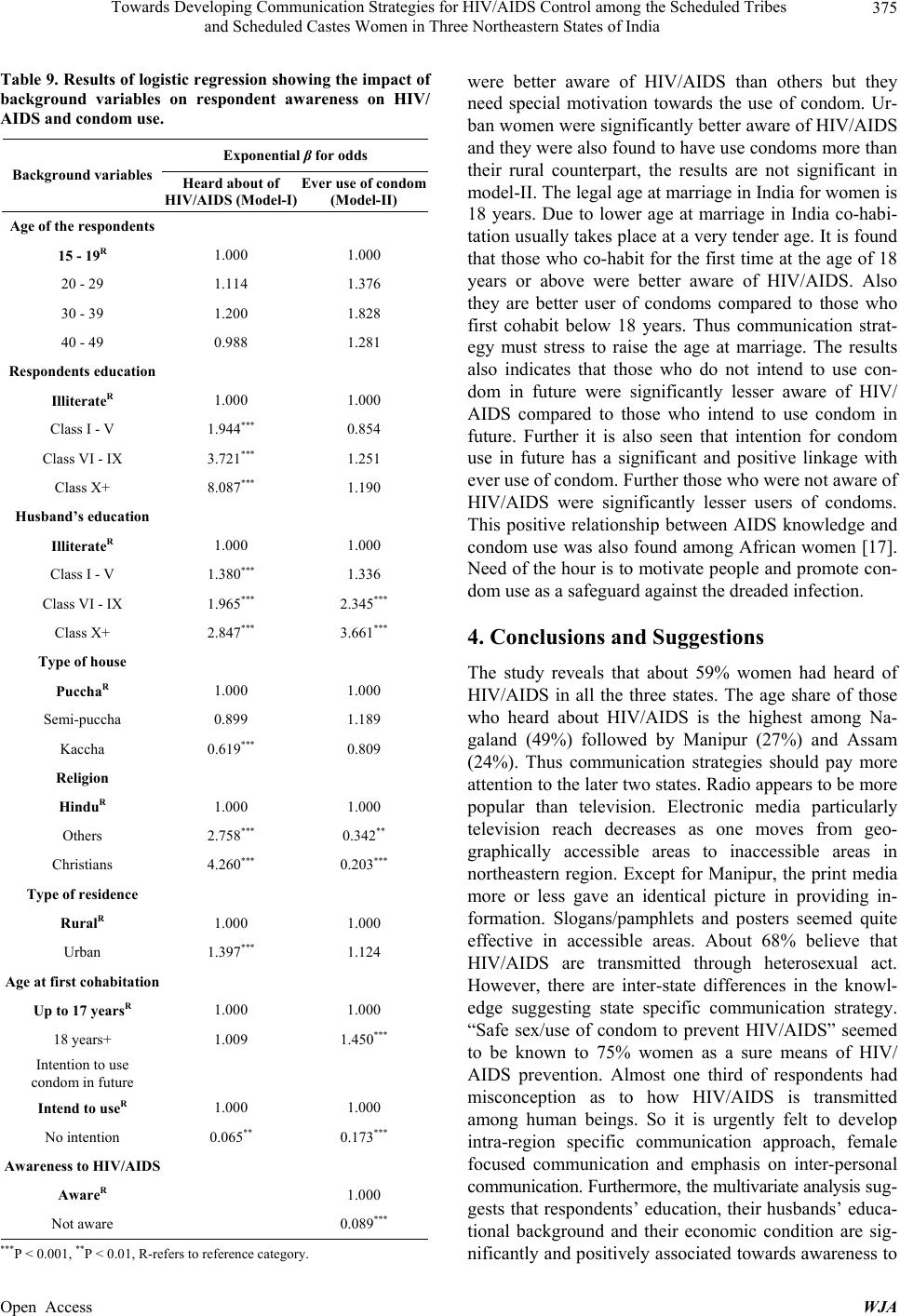
HIV/AIDS. The multivariate model also suggests that
husbands’ education of respondents plays a pivotal role
in determining the use of condom—a strong preventive
measure against HIV/AIDS and thus it demands to in-
crease men’s participation in reproductive health matters.
The analysis also shows that though Christians are better
aware of HIV/AIDS, the use of condom among them is
lower than Hindus.
Manipur and Nagaland have predominantly Christian
population, whereas Assam has Hindu population. A
comparison of the responses of Christian and Hindu re-
spondents has been made for evolving broad communi-
cation strategy in northeastern region of India. The sug-
gested communication strategies are mentioned below.
4.1. Need for Region Specific Communication
Approach
Inter-state and rural-urban differences were observed
about HIV/AIDS awareness, prevention methods, media
contribution and related misconceptions about HIV/
AIDS among three states. Hence, communication ap-
proach must take these findings and findings of similar
surveys in other northeastern states into consideration
while designing any communication strategy. Education
seems to be the single most important determinant in
creating awareness of HIV/AIDS. Communication of
HIV/AIDS message should aim at reducing the existing
knowledge gap and bring about desired behavioural
changes among the persons considered in “high risk”
group with special reference to female population of
Scheduled caste and Scheduled tribes in northeastern
region. Two specific communication approaches have
been suggested to develop state and community specific
communication strategy.
4.2. Female Focused Communication
Keeping in view that women by and large in northeast-
ern region play a prominent role in domestic and commu-
nity activities, a “female focused” communication will
have positive effects in controlling HIV/AIDS in the re-
gion. The women should be “educated” to remove the
misconception, and to persuade their men folks to adopt
methods of safe sex. The “safe sex” concept must be in-
corporated in the family planning programme and media
message must highlight concept of safe sex. Since
women encounter sexual experiences early in their lives,
existing means of communication including educational
institutions must form a part of an “advocacy group” to
promote safe sex targeted to young and adolescent fe-
males women who should be encouraged to persuade
their men folks to use condom for safe sex and sex denial
to men without condom use should be advocated. A
study suggested the promotion of condom use particu-
larly in the context of casual sexual relations to reduce
the potential for the spread of STD/HIV in Bangladeshi
population [18]. At the same time, communication should
also stress to raise the age at marriage in the region.
4.3. Emphasis on Interpersonal Communication
In all three states’ interpersonal communication, husbands
and other relatives seem to provide a great deal of
information to women. Due to limited reach of mass
media in inaccessible areas, interpersonal communication
keeps a prime mode of sharing and exchanging views of
ideas. Also community meetings are found to be
effective in these areas. Hence, it is suggested that apart
from electronic and print media, interpersonal communi-
cation, community meetings and use of posters, hoarding
and other existing locally popular means must form an
integral part of communication strategy. Efforts should
be made to utilize health workers including doctors in
creating awareness of HIV/AIDS who are currently least
involved in promoting health care.
5. Acknowledgements
The authors sincerely acknowledge the support extended
by Dr. Neeru Singh, Director, Regional Medical Re-
search Centre for Tribals (ICMR), Jabalpur and Indian
Council of Medical Research, New Delhi, India for pro-
viding the facilities. Further the authors also place on
record and thank Ministry of Health and Family Welfare,
Government of India and International Institute for Popu-
lation Sciences, Mumbai, India for allowing using RCH
data set for the study.
REFERENCES
[1] J. Shreedhar and A. Colaco, “Broadening the Front: NGO
Response to HIV and AIDS in India,” ACTIONAID, The
British Council, New Delhi, 1996.
[2] UNAIDS/NACO/WHO, “2.5 Million People Living in
India with HIV, According to New Estimates,” Statistics
on HIV/AIDS Cases India 2005-2006, 2007.
[3] NACO, “Monthly Updates on AIDS, NACO, India, 31st
August,” Statistics on HIV/AIDS Cases India 2005-2006,
2006.
[4] G. Thomas, “AIDS in India,” Rawat Publication, Jaipur,
1994.
[5] H. C. Srivastava, K. B. Saha and K. I. Sahay, “Under-
standing Awareness and Knowledge about AIDS in the
Selected States of India,” XXI Annual Conference of In-
dian Association for Studies in Population, Banaras Hindu
University, 1998, Unpublished.
[6] J. Moore, “AIDS: Prevention and Control. Invited Presen-
tations and Papers from the World Summit of Ministers
Open Access WJA