Experience of Patients Undergoing Mini-Arthroscopy Compared to MRI in the Earliest Phases of Arthritis
Open Access IJCM
2
permeability, and has been shown to be a sensitive too l to
detect changes after treatment [6-11].
At international scientific meeting s, when results from
studies using synovial biopsy sampling by mini-arthro-
scopy are presented by researchers of our Department of
Clinical Immunology and Rheumatology of the Acade mic
Medical Center (AMC) Amsterdam, questions are raised
concerning patient’s experience of synovial biopsy sam-
pling by mini-arthroscopy, especially in individuals with-
out arthritis. It seems that there is a general idea that
mini-arthroscopy is an invasive procedure and a burden
for patients, which seems to hamper the use of mini-ar-
throscopic synovial biopsy sampling in some research
centres. Patient expectations and experience of mini-ar-
throscopy have never been studied. Therefore, we inves-
tigated patient’s expectations before and experience after
mini-arthroscopic synovial biopsy sampling and com-
pared those with expectations before and experience after
undergoing dynamic contrast-enhanced MRI, which is
generally seen as a non -invasive procedure.
2. Methods
2.1. Study Subjects
Group A consisted of early arthritis patients (arthritis
duration less than 1 year) with an inflamed knee, ankle or
wrist, who were disease modifying antirheumatic drug
naive (AMC’s “Synoviomics” program) [12]. Group B
consisted of individuals at risk for developing RA, de-
fined by the presence of IgM-rheumatoid factor and/or
anti-citrullinated protein antibodies, but no evidence of
arthritis upon physical examination [13] (AMC’s “Pre-
Synoviomics” program) [14]. The study was performed
according to the principles of the Declaration of Helsinki,
approved by the medical ethical committee of the AMC,
and all study subjects gave written in formed consent.
2.2. MRI
All study subjects underwent DCE-MRI as previously
described [6]. In Group A, a clinically inflamed (swo llen
and painful) wrist, knee or ankle joint was examined and
in Group B an arbitrarily chosen knee joint was exam-
ined in all cases. Briefly, images were acquired on either
a closed (1.5 Tesla GE Signa Horizon Echospeed, LX9.0,
General Electric Medical Systems, Milwaukee, Wiscon-
sin, USA) or open (Panorama 1 Tesla Open, Philips, Best,
the Netherlands) MRI scanner, depending on the avail-
ability of the machine. Three scans were performed after
which a contrast agent gadolinium (Magnevist, Schering,
Berlin, Germany) was injected intravenously and 2 addi-
tional scans were performed. Total duration of the pro-
cedure was 60 minutes.
2.3. Synovial Biopsy Sampling by
Mini-Arthroscopy
Within one week after the MRI, synovial biopsy sam-
pling was performed at the outpatient clinic by means of
mini-arthroscopy under local anaesthetics, as previously
described [2,15]. The same joint was chosen for both
procedures. For each study group 24 up to 32 synovial
tissue biopsies were obtained during one procedure. The
duration of the t ota l proce du re was 45 to 60 minut es.
2.4. Questionnaires
Before and after both procedures, subjects filled in ques-
tionnaires with items about expectations and the experi-
ence they had with regard to the procedures. Questions
asked were 1) Do you have preference for MRI or mini-
arthroscopy or do you have “no preference”? 2) Please
mark how well you think you are prepared for (a) MRI
and (b) mini-arthroscopy 3) Please mark the level of fear
you experience of (a) MRI and (b) mini-arthroscopy? 4)
Please mark if you are reluctant to undergo (a) MRI and
(b) mini-arthroscopy. The first question was multiple
choice; the latter three questions were depicted on a vis-
ual analogue scale (VAS) of 0 - 100 mm. In addition,
study subjects could comment their choice of preference
for one of the procedures. The first questionnaire was
completed and handed in before and the second ques-
tionnaire was filled in after both procedures.
2.5. Statistical Analysis
We describe preference for either of the procedures be-
fore and after the procedures or compared preference in
Group A with Group B using Chi-square test. In addition,
differences in baseline emotional aspects with respect to
both procedures and differences in preference after pro-
cedures compared to baseline were analysed using Wil-
coxon signed rank test for related samples. P-value <
0.05 was considered statistically significant. Statistical
analysis was performed using PASW Statistics 18 (SPSS
Inc., Chicago, IL).
3. Results
Of 38 subjects baseline and follow-up questionnaires were
available: 17 from Grou p A and 21 fro m Group B. Table
1 shows the disposition of study subjects with regard to
type of joint examined and MRI machine used.
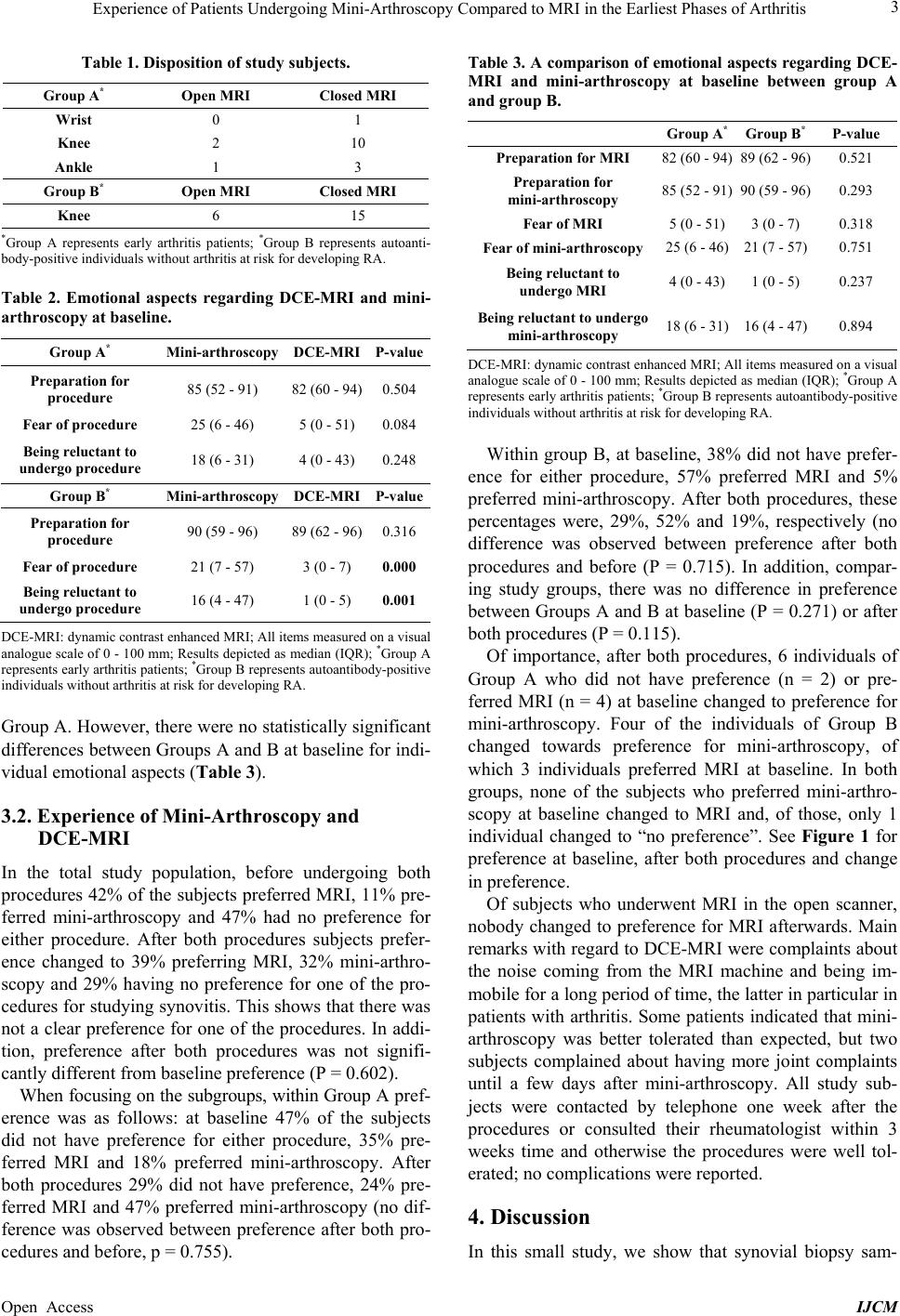
3.1. Emotional Aspects
With respect to emotional aspects subjects generally felt
well prepared fo r both procedures. In Group B scores for
fear and reluctance were higher for mini-arthroscopy
compared to MRI, see Table 2. This was not the case for