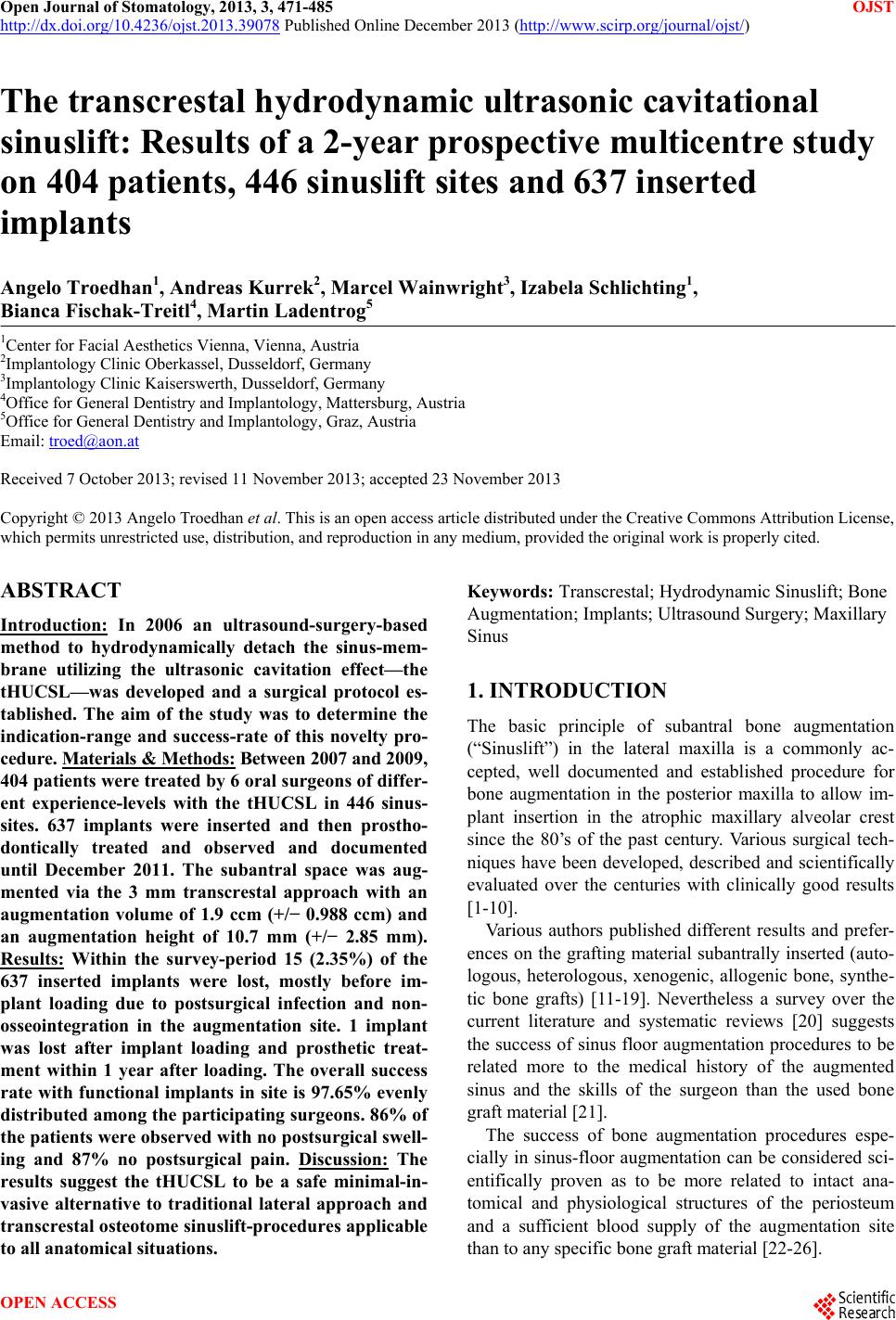
 Open Journal of Stomatology, 2013, 3, 471-485 OJST http://dx.doi.org/10.4236/ojst.2013.39078 Published Online December 2013 (http://www.scirp.org/journal/ojst/) The transcrestal hydrodynamic ultrasonic cavitational sinuslift: Results of a 2-year prospective multicentre study on 404 patients, 446 sinuslift sites and 637 inserted implants Angelo Troedhan1, Andreas Kurrek2, Marcel Wainwright3, Izabela Schlichting1, Bianca Fischak-Treitl4, Martin Ladentrog5 1Center for Facial Aesthetics Vienna, Vienna, Austria 2Implantology Clinic Oberkassel, Dusseldorf, Germany 3Implantology Clinic Kaiserswerth, Dusseldorf, Germany 4Office for General Dentistry and Implan tology, Mattersburg, Austria 5Office for General Dentistry and Implantology, Graz, Austria Email: troed@aon.at Received 7 October 2013; revised 11 November 2013; accepted 23 November 2013 Copyright © 2013 Angelo Troedhan et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Introduction: In 2006 an ultrasound-surgery-based method to hydrodynamically detach the sinus-mem- brane utilizing the ultrasonic cavitation effect—the tHUCSL—was developed and a surgical protocol es- tablished. The aim of the study was to determine the indication-range and success-rate of this novelty pro- cedure. Materials & Methods: Between 2007 and 2009, 404 patients were treated by 6 oral surgeons of differ- ent experience-levels with the tHUCSL in 446 sinus- sites. 637 implants were inserted and then prostho- dontically treated and observed and documented until December 2011. The subantral space was aug- mented via the 3 mm transcrestal approach with an augmentation volume of 1.9 ccm (+/− 0.988 ccm) and an augmentation height of 10.7 mm (+/− 2.85 mm). Results: Within the survey-period 15 (2.35%) of the 637 inserted implants were lost, mostly before im- plant loading due to postsurgical infection and non- osseointegration in the augmentation site. 1 implant was lost after implant loading and prosthetic treat- ment within 1 year after loading. The overall success rate with functional implants in site is 97.65% evenly distributed among the participating surgeons. 86% of the patients were observed with no postsurgical swell- ing and 87% no postsurgical pain. Discussion: The results suggest the tHUCSL to be a safe minimal-in- vasive alternative to traditional lateral approach and transcrestal osteotome sinuslift-procedures applicable to all anatomical situations. Keywords: Transcrestal; Hydrodynamic Sinuslift; Bone Augmentation; Implants; Ultrasound Surgery; Maxillary Sinus 1. INTRODUCTION The basic principle of subantral bone augmentation (“Sinuslift”) in the lateral maxilla is a commonly ac- cepted, well documented and established procedure for bone augmentation in the posterior maxilla to allow im- plant insertion in the atrophic maxillary alveolar crest since the 80’s of the past century. Various surgical tech- niques have been developed, described and scientifically evaluated over the centuries with clinically good results [1-10]. Various authors published different results and prefer- ences on the grafting material subantrally inserted (auto- logous, heterologous, xenogenic, allogenic bone, synthe- tic bone grafts) [11-19]. Nevertheless a survey over the current literature and systematic reviews [20] suggests the success of sinus floor augmentation procedures to be related more to the medical history of the augmented sinus and the skills of the surgeon than the used bone graft material [21]. The success of bone augmentation procedures espe- cially in sinus-floor augmentation can be considered sci- entifically proven as to be more related to intact ana- tomical and physiological structures of the periosteum and a sufficient blood supply of the augmentation site than to any specific bone graft material [22-26]. OPEN ACCESS  A. Troedhan et al. / Open Journal of Stomatology 3 (2013) 471-485 472 Diligent presurgical diagnosis, intrasurgical complica- tion management and postsurgical patient and complica- tion management can be considered to play a major role in the overall success of subantral augmentation proce- dures [27-31] as well as the experience of the surgeon as clinical research in other fields of oral surgery suggests [32,33]. The more bone augmentation surgery is per- formed with highly invasive surgical methods, the more postsurgical morbidity can be expected as voluminous edema, pain, uncontrollable bleeding and long term fail- ure of the augmentation. Proper education and training of the oral surgeon are mandatory to develop the necessary skills for traditional sinuslift-procedures with lateral and/or transcrestal ac- cess to prevent the most feared intrasurgical complica- tion of a partial or entire rupture of the sinus-membrane. Therefore, sinuslift procedures also follow the trend from massive invasive surgical protocols with a lateral approach and lateral window preparation [1-3] towards minimal invasive ultrasound surgical techniques [34] based on the idea of the minimal invasive transcrestal approach [4,5]. The limited possible augmentation vol- ume of the classical Summers lift was partly enhanced by the introduction of balloon and hydraulic pressure as- sisted transcrestal sinuslift techniques [35-37]. Still these procedures are challenging the manual dili- gence of the performing, surgeon and proper training and experience have to be achieved by the surgeon to per- form these techniques with an acceptable success rate. Above all—in case of failure—the inconveniences to the patient (edema, pain, costs, long term morbidity) have to be kept as small as possible. To combine the advantages of a lateral approach si- nuslift (scalable augmentation area an d volume) with the atraumaticity of the transcrestal approach and to avoid the need of the surgeon to touch the sinus membrane with instruments or balloons in the detachment-process (and therewith eliminate one of the major risks of intra- surgical membrane perforation) and to utilize the well documented advantages of hydrodynamic pressure sinus- membrane-detachment [36,37] and atraumaticity of ul- trasonic surgery, the transcrestal hydrodynamic ultra- sonic cavitational sinuslift (tHUCSL-INTRALIFT) was developed i n 200 6 [ 38 -4 0]. The significant application safety of the tHUCSL- INTRALIFT compared to traditional transcrestal Sum- mers- and balloon-assisted sinuslift-procedures can be considered as verified in animal cadaver experiments [41]. The aims of the current prospective multicentre study performed in six implantologist’s offices were: 1) The evaluation if success-rates of the tHUCSL- INTRALIFT depend on the experience-level of the per- forming oral surgeon, the type and/or brand of suban- trally inserted bone graft material and type and/or brand of inserted dental implants. 2) The verification of the unrestricted applicability of the tHUCSL-INTRALIFT to every subantral anatomical surgical site from very narrow single tooth-gaps up to bilateral endentolous upper jaws and the vastly varying anatomy of the human maxillary sinus as suggested by the experimental results [38]. 3) The evaluation of clin ical application safety as sug- gested by comparative animal cadaver studies [41] when long term experienced implantologists are compared to average experienced ones. 4) The evaluation of the procedural burdening of pa- tients such as postsurgical pain and swelling and overall success-rate of the tHUC-sinuslift-technique. 2. MATERIAL & METHODS 2.1. Experience Level of Participating Surgeons To be as close as possible to working conditions of most oral surgeons, 6 dentists in 5 offices were participating in the prospective study treating 412 patients in 457 maxil- lary sinus sites with a subantral alveolar crest height of 1 - 10 mm with the tHUCSL-INTRALIFT procedure be- tween February 2007 and December 2009. (Although subantral crest heights of 8 - 10 mm might be treated with short implants nowadays the authors decided the inclusion when the protocol was setup in 2006 due to lack of documented long-term success rates of short im- plants in the molar region of the maxilla at that time.) One participating dentist is also specialized in oro- maxillofacial surgery for 20 years, three dentists have long term experience in implantology and sinus lifting for 5 - 10 years, one participating dentist short time experi- ence in implantology for 4 years and one dentist was at the beginner level in implantology with 2 years of prac- tical experience, the latest two without experience in sinuslifting. 2.2. Patients Inclusion Criteria To be eligib le for tHUC-sinuslift surgery all patients had to fulfil the common criteria for any type of sinuslift- procedure (no prior Caldwell-Luc-Sinus-surgery, no chronic or acute maxillary sinusitis, no acute cold, no mucocele visible in panoramic X-ray, permission by General Practitioner/Internist/ENT). Smokers were con- sidered as eligible since percentage of smokers in the European populatio n is still high with an average of 30%. All patients requesting a sinuslift in all 5 participating clinics/offices within the study period and fulfilling the common eligibility-criteria for any sinuslift procedure were exclusively treated with the tHUCSL-Intralift pro- cedure. Copyright © 2013 SciRes. OPEN ACCESS 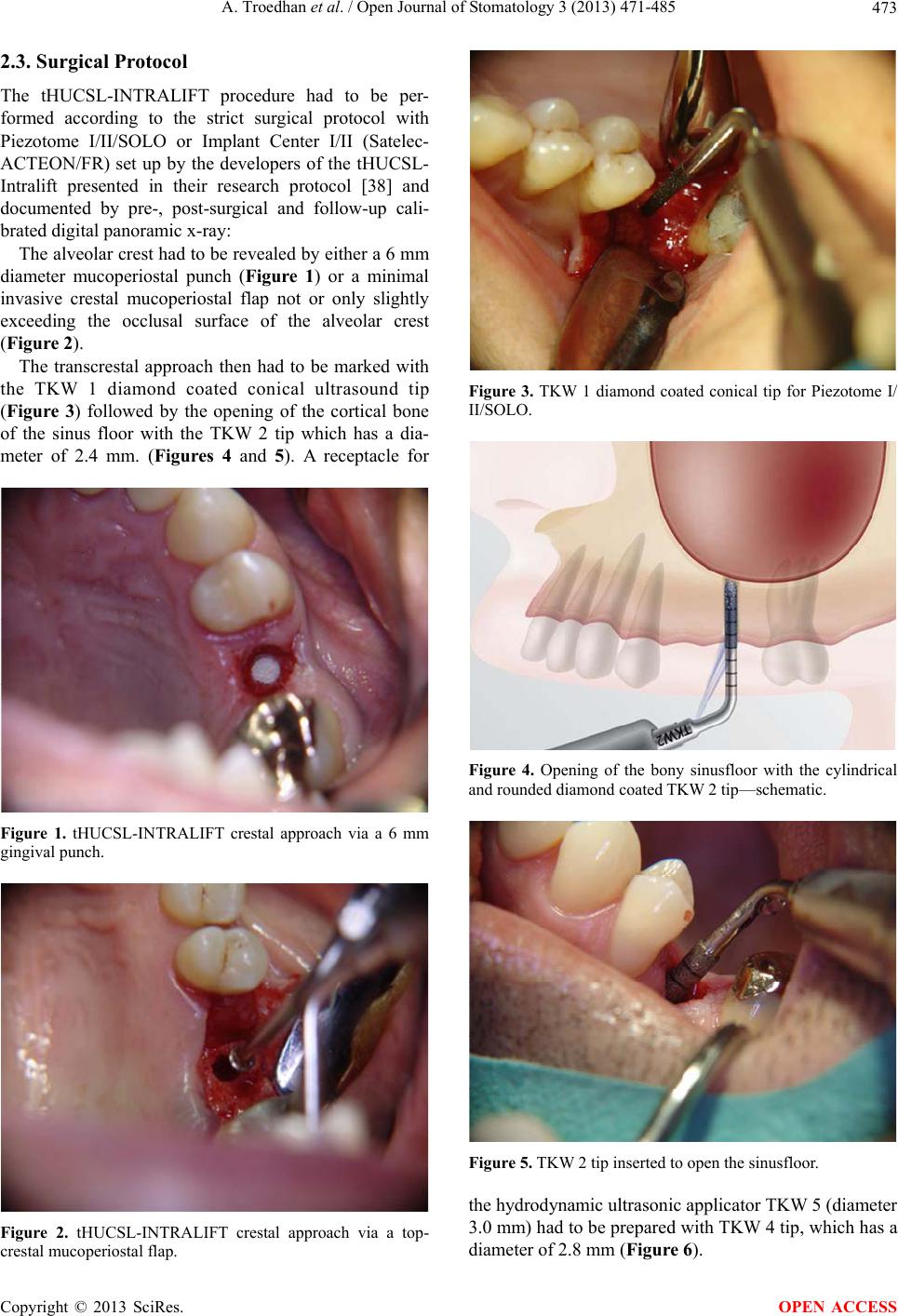 A. Troedhan et al. / Open Journal of Stomatology 3 (2013) 471-485 473 2.3. Surgical Protocol The tHUCSL-INTRALIFT procedure had to be per- formed according to the strict surgical protocol with Piezotome I/II/SOLO or Implant Center I/II (Satelec- ACTEON/FR) set up by the developers of the tHUCSL- Intralift presented in their research protocol [38] and documented by pre-, post-surgical and follow-up cali- brated digital panoramic x-ray: The alveolar crest had to be revealed by either a 6 mm diameter mucoperiostal punch (Figure 1) or a minimal invasive crestal mucoperiostal flap not or only slightly exceeding the occlusal surface of the alveolar crest (Figure 2). The transcrestal approach then had to be marked with the TKW 1 diamond coated conical ultrasound tip (Figure 3) followed by the opening of the cortical bone of the sinus floor with the TKW 2 tip which has a dia- meter of 2.4 mm. (Figures 4 and 5). A receptacle for Figure 1. tHUCSL-INTRALIFT crestal approach via a 6 mm gingival punch. Figure 2. tHUCSL-INTRALIFT crestal approach via a top- crestal mucoperiostal flap. Figure 3. TKW 1 diamond coated conical tip for Piezotome I/ II/SOLO. Figure 4. Opening of the bony sinusfloor with the cylindrical and rounded diamond coated TKW 2 tip—schematic. Figure 5. TKW 2 tip inserted to open the sinusfloor. the hydrodynamic ultrasonic applicator TKW 5 (diameter 3.0 mm) had to be prepared with TKW 4 tip, which has a diameter of 2.8 mm (Figure 6). Copyright © 2013 SciRes. OPEN ACCESS  A. Troedhan et al. / Open Journal of Stomatology 3 (2013) 471-485 474 Figure 6. Preparation of the 2.8 mm receptacle with the cylin- drical diamond coated TKW 4-tip—schematic. After checking the snug fit of the TKW 5-applicato r in the receptacle the hydrodynamic ultrasonic cavitational detachment of the sinus membrane had to be performed at a power setting of the Piezotome at mode D3 with a flow rate of 30 ml/min for 5 seconds. At these settings the sinus membrane will be completely detached from the entire sinus floor and provides a possible augmen- tation volume of 2.5 ccm. (Figures 7 and 8) The integrity of the sinus-membrane had to be check- ed visually and/or by Valsalva-test. In case of a perfora- tion of the sinus-membrane the surgeon had to decide wether to proceed or interr upt surgery for wound clo sure depending on the size of the pe rf orat i o n w he n vi si bl e. After widening of the transcrestal trepanation with TKW 3 (Figure 9) and TKW 4 diamond coated ultra- sound tips (Figure 10) synthetic, xenogenic and/or auto- logous bone graft of the surgeon’s choice was inserted under the sinus membrane with a common bone applica- tor (Figure 11). When available the surgeons were advised to check the augmentation area and height intraoperatively step by step with digital X-ray to determine the case-sufficient extension of the augmentation. (Figures 12-14) It was also the surgeon’s decision to insert one or more implants simultaneously depending on the height and quality of the subantral alveolar crest to achieve primary stability with the surgeon’s co mmon implant system. The only prerequisite towards the choice of the implant was an implant—diameter wider than 3 mm since the diame- ter of the TKW 5 tip is 3 mm. 2.4. Study Data Documented and Follow Up Data as follows then had to be documented by the par- ticipating dentists in a web-based Excel-Sheet accessible via password: Date of surgery, name of the surgeon coded by a number, patient’s name, age, sex, smoker y/n, diabetes Figure 7. Insertion of the hollow 3.0 mm TKW 5-tip and de- tachment of the sinus-membrane by injection of ultrasonic os- cillating saline solution creating a cavitation effect—schematic. Figure 8. TKW 5-tip inserted into the receptacle: this tip seals the approach canal like a sealing ventile and enables by it’s oscillations the cavitation effect. Figure 9. After detachment of the sinus-membrane from the bony floor the approach canal is widened with the cylindrical diamond coated TKW 3-tip. Copyright © 2013 SciRes. OPEN ACCESS 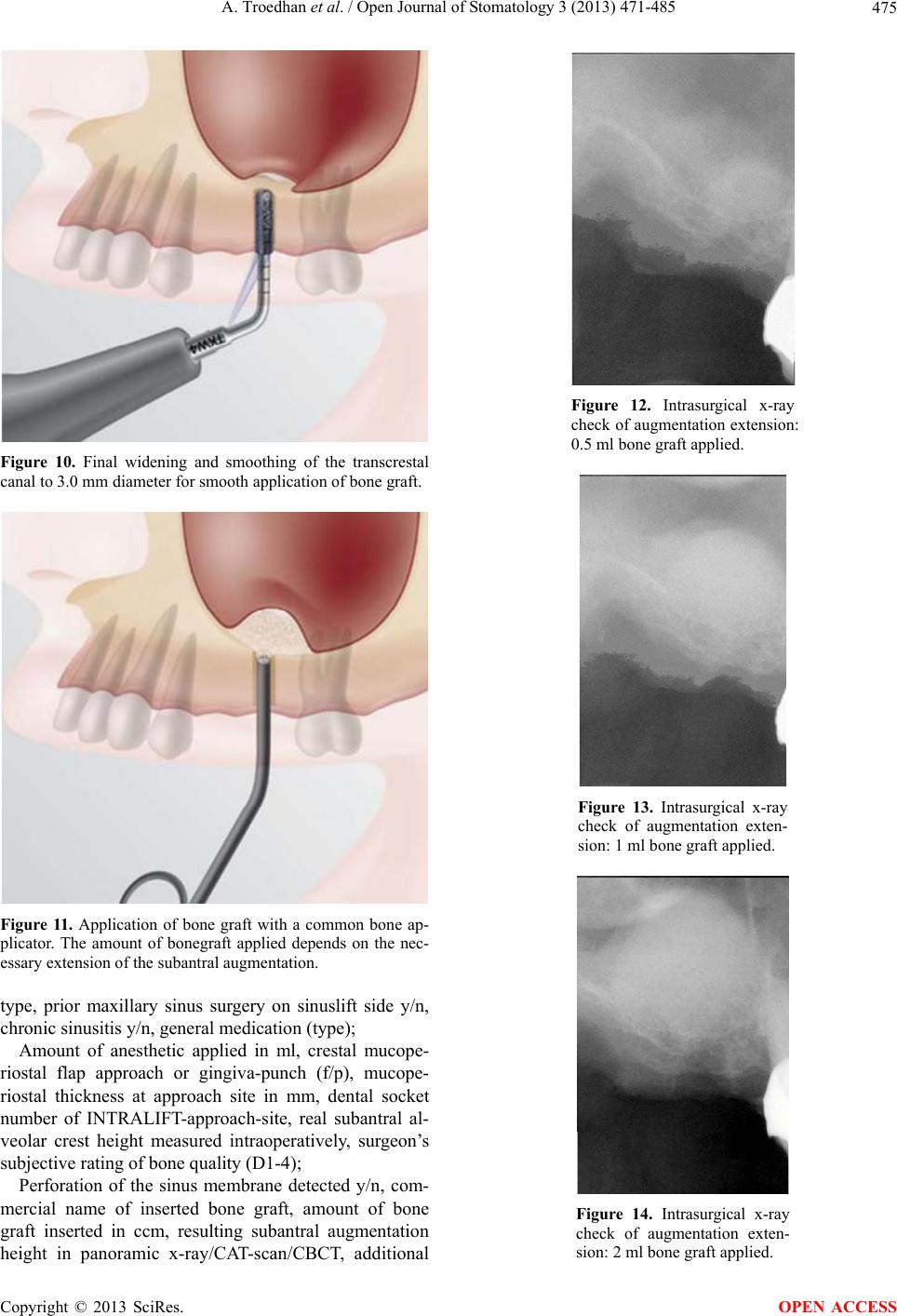 A. Troedhan et al. / Open Journal of Stomatology 3 (2013) 471-485 475 Figure 10. Final widening and smoothing of the transcrestal canal to 3.0 mm diameter for smooth application of bone graft. Figure 11. Application of bone graft with a common bone ap- plicator. The amount of bonegraft applied depends on the nec- essary extension of the subantral augmentation. type, prior maxillary sinus surgery on sinuslift side y/n, chronic sinusitis y/n, general medication (type); Amount of anesthetic applied in ml, crestal mucope- riostal flap approach or gingiva-punch (f/p), mucope- riostal thickness at approach site in mm, dental socket number of INTRALIFT-approach-site, real subantral al- veolar crest height measured intraoperatively, surgeon’s subjective rating of bone qu a lity (D1-4 ); Perforation of the sinus membrane detected y/n, com- mercial name of inserted bone graft, amount of bone graft inserted in ccm, resulting subantral augmentation height in panoramic x-ray/CAT-scan/CBCT, additional Figure 12. Intrasurgical x-ray check of augmentation extension: 0.5 ml bone graft applied. Figure 13. Intrasurgical x-ray check of augmentation exten- sion: 1 ml bone graft applied. Figure 14. Intrasurgical x-ray check of augmentation exten- sion: 2 ml bone graft applied. Copyright © 2013 SciRes. OPEN ACCESS 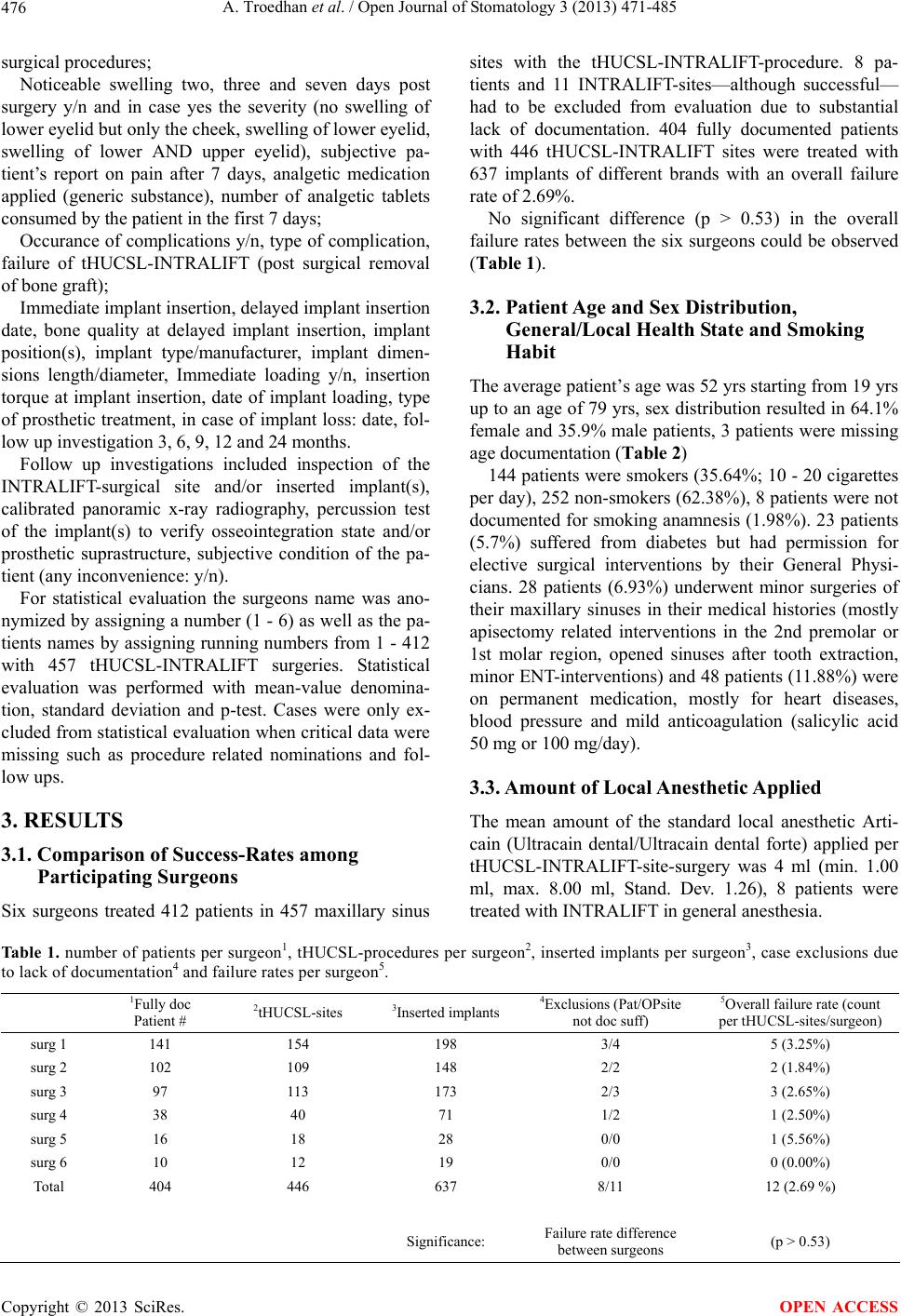 A. Troedhan et al. / Open Journal of Stomatology 3 (2013) 471-485 Copyright © 2013 SciRes. 476 OPEN ACCESS surgical procedures; Noticeable swelling two, three and seven days post surgery y/n and in case yes the severity (no swelling of lower eyelid but only th e cheek, swelling of lower eyelid , swelling of lower AND upper eyelid), subjective pa- tient’s report on pain after 7 days, analgetic medication applied (generic substance), number of analgetic tablets consumed by the patient in the first 7 days; Occurance of complications y/n, type of complication, failure of tHUCSL-INTRALIFT (post surgical removal of bone graft); Immediate implant insertion, delayed impla nt in sertion date, bone quality at delayed implant insertion, implant position(s), implant type/manufacturer, implant dimen- sions length/diameter, Immediate loading y/n, insertion torque at implant insertion, date of implant loading, type of prosthetic treatment, in case of implant lo ss: date, fol- low up investigat i on 3, 6, 9, 12 and 2 4 m on t hs. Follow up investigations included inspection of the INTRALIFT-surgical site and/or inserted implant(s), calibrated panoramic x-ray radiography, percussion test of the implant(s) to verify osseointegration state and/or prosthetic suprastructure, subjective condition of the pa- tient (any inconvenience: y/n). For statistical evaluation the surgeons name was ano- nymized by assigning a number (1 - 6) as well as the pa- tients names by assigning running numbers from 1 - 412 with 457 tHUCSL-INTRALIFT surgeries. Statistical evaluation was performed with mean-value denomina- tion, standard deviation and p-test. Cases were only ex- cluded from statistical evaluation when critical data were missing such as procedure related nominations and fol- low ups. 3. RESULTS 3.1. Comparison of Success-Rates among Participating Surgeons Six surgeons treated 412 patients in 457 maxillary sinus sites with the tHUCSL-INTRALIFT-procedure. 8 pa- tients and 11 INTRALIFT-sites—although successful— had to be excluded from evaluation due to substantial lack of documentation. 404 fully documented patients with 446 tHUCSL-INTRALIFT sites were treated with 637 implants of different brands with an overall failure rate of 2.69%. No significant difference (p > 0.53) in the overall failure rates between the six surgeons could be observed (Table 1). 3.2. Patient Age and Sex Distribution, General/Local Health State and Smoking Habit The av erag e patien t’s age w as 52 yr s sta rting fr om 19 yr s up to an age of 79 yrs, sex distribution resulted in 64.1% female and 35.9% male patients, 3 patients were missing age documentati o n ( Table 2) 144 patients were smokers (35.64%; 10 - 20 cigarettes per day), 252 n on-smokers (62.38%) , 8 patients were no t documented for smoking anamnesis (1.98%). 23 patients (5.7%) suffered from diabetes but had permission for elective surgical interventions by their General Physi- cians. 28 patients (6.93%) underwent minor surgeries of their maxillary sinuses in their medical histories (mostly apisectomy related interventions in the 2nd premolar or 1st molar region, opened sinuses after tooth extraction, minor ENT-interventions) and 48 patients (11.88%) were on permanent medication, mostly for heart diseases, blood pressure and mild anticoagulation (salicylic acid 50 mg or 100 mg/day). 3.3. Amount of Local Anesthetic Applied The mean amount of the standard local anesthetic Arti- cain (Ultracain dental/Ultracain dental forte) applied per tHUCSL-INTRALIFT-site-surgery was 4 ml (min. 1.00 ml, max. 8.00 ml, Stand. Dev. 1.26), 8 patients were treated with INTRALIFT in general anesthesia. Table 1. number of patients per surgeon1, tHUCSL-procedures per surgeon2, inserted implants per surgeon3, case exclusions due to lack of documentation4 and failure rates per surgeon5. 1Fully doc Patient # 2tHUCSL-sites 3Inserted implants 4Exclusions (Pat/OPsite not doc suff) 5Overall failure rate (count per tHUCSL-si tes/surgeon ) surg 1 141 154 198 3/4 5 (3.25%) surg 2 102 109 148 2/2 2 (1.84%) surg 3 97 113 173 2/3 3 (2.65%) surg 4 38 40 71 1/2 1 (2.50%) surg 5 16 18 28 0/0 1 (5.56%) surg 6 10 12 19 0/0 0 (0.00%) Total 404 446 637 8/11 12 (2.69 %) Significance: Failure rate difference between surgeons (p > 0.53) 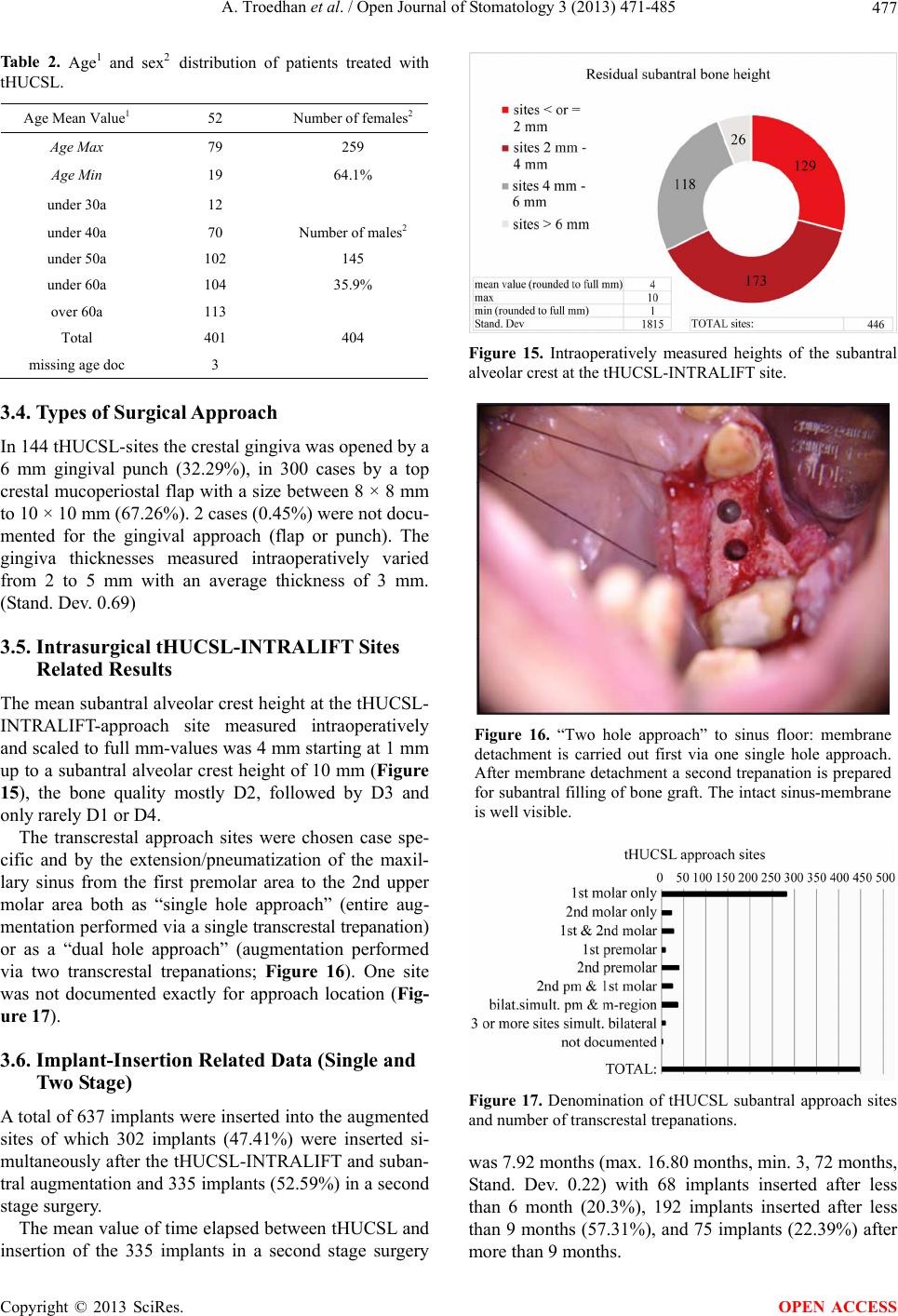 A. Troedhan et al. / Open Journal of Stomatology 3 (2013) 471-485 477 Table 2. Age1 and sex2 distribution of patients treated with tHUCSL. Age Mean Value1 52 Number of females2 Age Max 79 259 Age Min 19 64.1% under 30a 12 under 40a 70 Number of m ales2 under 50a 102 145 under 60a 104 35.9% over 60a 113 Total 401 404 missing age doc 3 3.4. Types of Surgical Approach In 144 tHUCSL-sites the crestal gingiva was opened by a 6 mm gingival punch (32.29%), in 300 cases by a top crestal mucoperiostal flap with a size between 8 × 8 mm to 10 × 10 mm (67.26%). 2 cases (0.45%) were not docu- mented for the gingival approach (flap or punch). The gingiva thicknesses measured intraoperatively varied from 2 to 5 mm with an average thickness of 3 mm. (Stand. Dev. 0.69) 3.5. Intrasurgical tHUCSL-INTRALIFT Sites Related Results The mean subantral alveolar crest height at the tHUCSL- INTRALIFT-approach site measured intraoperatively and scaled to full mm-values was 4 mm starting at 1 mm up to a subantral alveolar crest height of 10 mm (Figure 15), the bone quality mostly D2, followed by D3 and only rarely D1 or D4. The transcrestal approach sites were chosen case spe- cific and by the extension/pneumatization of the maxil- lary sinus from the first premolar area to the 2nd upper molar area both as “single hole approach” (entire aug- mentation performed via a single transcrestal trepanation) or as a “dual hole approach” (augmentation performed via two transcrestal trepanations; Figure 16). One site was not documented exactly for approach location (Fig- ure 17). 3.6. Implant-Insertion Related Data (Single and Two Stage) A total of 637 implants were inserted into the augmented sites of which 302 implants (47.41%) were inserted si- multaneously after the tHUCSL-INTRALIFT and suban- tral augmentation and 335 implants (52.59%) in a second stage surgery. The mean value of time elapsed between tHUCSL and insertion of the 335 implants in a second stage surgery Figure 15. Intraoperatively measured heights of the subantral alveolar crest at t he tHUCSL-IN TRALIFT site. Figure 16. “Two hole approach” to sinus floor: membrane detachment is carried out first via one single hole approach. After membrane detachment a second trepanation is prepared for subantral filling of bone graft. The intact sinus-membrane is well visible. Figure 17. Denomination of tHUCSL subantral approach sites and number of transcrestal trepanations. was 7.92 months (max. 16.80 months, min. 3, 72 months, Stand. Dev. 0.22) with 68 implants inserted after less than 6 month (20.3%), 192 implants inserted after less than 9 months (57.31%), and 75 implants (22.39%) after more than 9 months. Copyright © 2013 SciRes. OPEN ACCESS 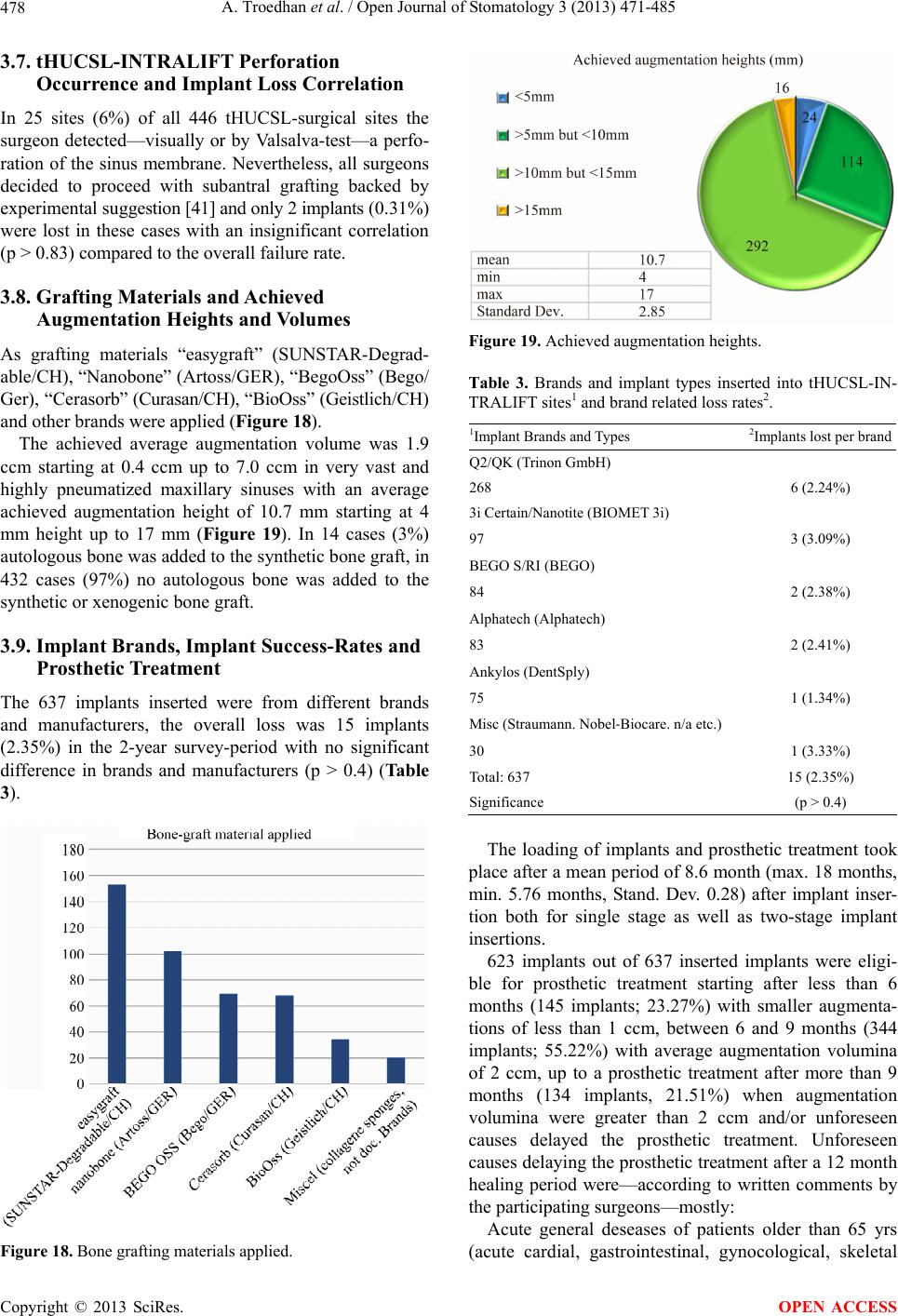 A. Troedhan et al. / Open Journal of Stomatology 3 (2013) 471-485 478 3.7. tHUCSL-INTRALIFT Perforation Occurrence and Implant Loss Correlation In 25 sites (6%) of all 446 tHUCSL-surgical sites the surgeon detected—visually or by Valsalva-test—a perfo- ration of the sinus membrane. Nevertheless, all surgeons decided to proceed with subantral grafting backed by experimental suggestion [41] and only 2 im plants (0.31%) were lost in these cases with an insignificant correlation (p > 0.83) compared to the overall failure rate. 3.8. Grafting Materials and Achieved Augmentation Heights and Volumes As grafting materials “easygraft” (SUNSTAR-Degrad- able/CH), “Nanobone” (Artoss/GER), “BegoOss” (Bego/ Ge r), “Ce ra sorb” (Curasan/CH), “BioOss” (Geistlic h/C H) and other brands were applied (Figure 18). The achieved average augmentation volume was 1.9 ccm starting at 0.4 ccm up to 7.0 ccm in very vast and highly pneumatized maxillary sinuses with an average achieved augmentation height of 10.7 mm starting at 4 mm height up to 17 mm (Figure 19). In 14 cases (3%) autologous bone was added to the synthetic bone graft, in 432 cases (97%) no autologous bone was added to the synthetic or xenogenic bone graft. 3.9. Implant Brands, Implant Success-Rates and Prosthetic Treatment The 637 implants inserted were from different brands and manufacturers, the overall loss was 15 implants (2.35%) in the 2-year survey-period with no significant difference in brands and manufacturers (p > 0.4) (Table 3). Figure 18. Bone grafting materials applied. Figure 19. Achieved augmentation heights. Table 3. Brands and implant types inserted into tHUCSL-IN- TRALIFT sites1 and brand related loss rates2. 1Implant Brands and Types 2Implants lost per brand Q2/QK (Trinon GmbH) 268 6 (2.24%) 3i Certain/Nanotite (BIOMET 3i ) 97 3 (3.09%) BEGO S/RI (BEGO) 84 2 (2.38%) Alphatech (Alphatech) 83 2 (2.41%) Ankylos (DentS ply) 75 1 (1.34%) Misc (Straumann. Nobel‐Biocare. n/a etc.) 30 1 (3.33%) Total: 637 15 (2.35%) Significance (p > 0.4) The loading of implants and prosthetic treatment took place after a mean period of 8.6 month (max. 18 months, min. 5.76 months, Stand. Dev. 0.28) after implant inser- tion both for single stage as well as two-stage implant insertions. 623 implants out of 637 inserted implants were eligi- ble for prosthetic treatment starting after less than 6 months (145 implants; 23.27%) with smaller augmenta- tions of less than 1 ccm, between 6 and 9 months (344 implants; 55.22%) with average augmentation volumina of 2 ccm, up to a prosthetic treatment after more than 9 months (134 implants, 21.51%) when augmentation volumina were greater than 2 ccm and/or unforeseen causes delayed the prosthetic treatment. Unforeseen causes delaying the prosthetic treatment after a 12 month healing period were—according to written comments by the participating surgeons—mostly: Acute general deseases of patients older than 65 yrs (acute cardial, gastrointestinal, gynocological, skeletal Copyright © 2013 SciRes. OPEN ACCESS 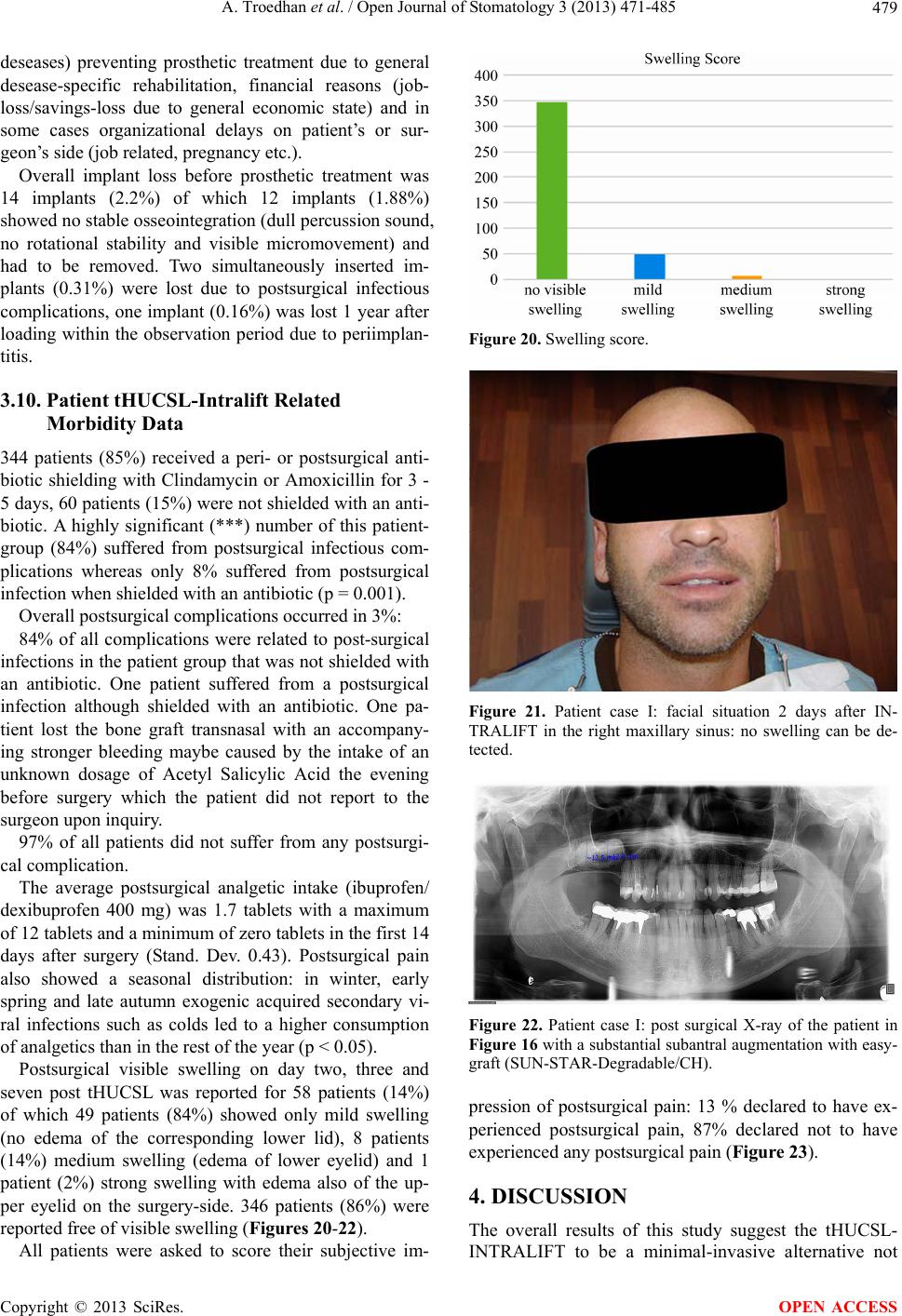 A. Troedhan et al. / Open Journal of Stomatology 3 (2013) 471-485 479 deseases) preventing prosthetic treatment due to general desease-specific rehabilitation, financial reasons (job- loss/savings-loss due to general economic state) and in some cases organizational delays on patient’s or sur- geon’s side (job relate d, pr eg nancy etc.). Overall implant loss before prosthetic treatment was 14 implants (2.2%) of which 12 implants (1.88%) showed no stable osseointegration (dull percussion sound, no rotational stability and visible micromovement) and had to be removed. Two simultaneously inserted im- plants (0.31%) were lost due to postsurgical infectious complications, one implant (0.1 6%) was lost 1 year after loading within the observation period due to periimplan- titis. 3.10. Patient tHUCSL-Intralift Related Morbidity Data 344 patients (85%) received a peri- or postsurgical anti- biotic shielding with Clindamycin or Amoxicillin for 3 - 5 days, 60 patients (15%) were not shielded with an anti- biotic. A highly significant (***) number of this patient- group (84%) suffered from postsurgical infectious com- plications whereas only 8% suffered from postsurgical infection when shielded with an antibiotic (p = 0.001). Overall postsurgical complications occurred in 3%: 84% of all complications were related to post-surgical infections in the p atient group that was not shielded with an antibiotic. One patient suffered from a postsurgical infection although shielded with an antibiotic. One pa- tient lost the bone graft transnasal with an accompany- ing stronger bleeding maybe caused by the intake of an unknown dosage of Acetyl Salicylic Acid the evening before surgery which the patient did not report to the surgeon upon inquiry. 97% of all patients did not suffer from any postsurgi- cal complication. The average postsurgical analgetic intake (ibuprofen/ dexibuprofen 400 mg) was 1.7 tablets with a maximum of 12 tablets and a minimum of zero tablets in the first 14 days after surgery (Stand. Dev. 0.43). Postsurgical pain also showed a seasonal distribution: in winter, early spring and late autumn exogenic acquired secondary vi- ral infections such as colds led to a higher consumption of analgetics than in the rest of the year (p < 0.05). Postsurgical visible swelling on day two, three and seven post tHUCSL was reported for 58 patients (14%) of which 49 patients (84%) showed only mild swelling (no edema of the corresponding lower lid), 8 patients (14%) medium swelling (edema of lower eyelid) and 1 patient (2%) strong swelling with edema also of the up- per eyelid on the surgery-side. 346 patients (86%) were reported free of visible swelling (Figures 20-22). All patients were asked to score their subjective im- Figure 20. Swelling score. Figure 21. Patient case I: facial situation 2 days after IN- TRALIFT in the right maxillary sinus: no swelling can be de- tected. Figure 22. Patient case I: post surgical X-ray of the patient in Figure 16 with a substantial subantral augmentation with easy- graft (SUN-STAR-Degradable/CH). pression of postsurgical pain: 13 % declared to have ex- perienced postsurgical pain, 87% declared not to have experienced any postsurgical pain (Figure 23). 4. DISCUSSION The overall results of this study suggest the tHUCSL- INTRALIFT to be a minimal-invasive alternative not Copyright © 2013 SciRes. OPEN ACCESS 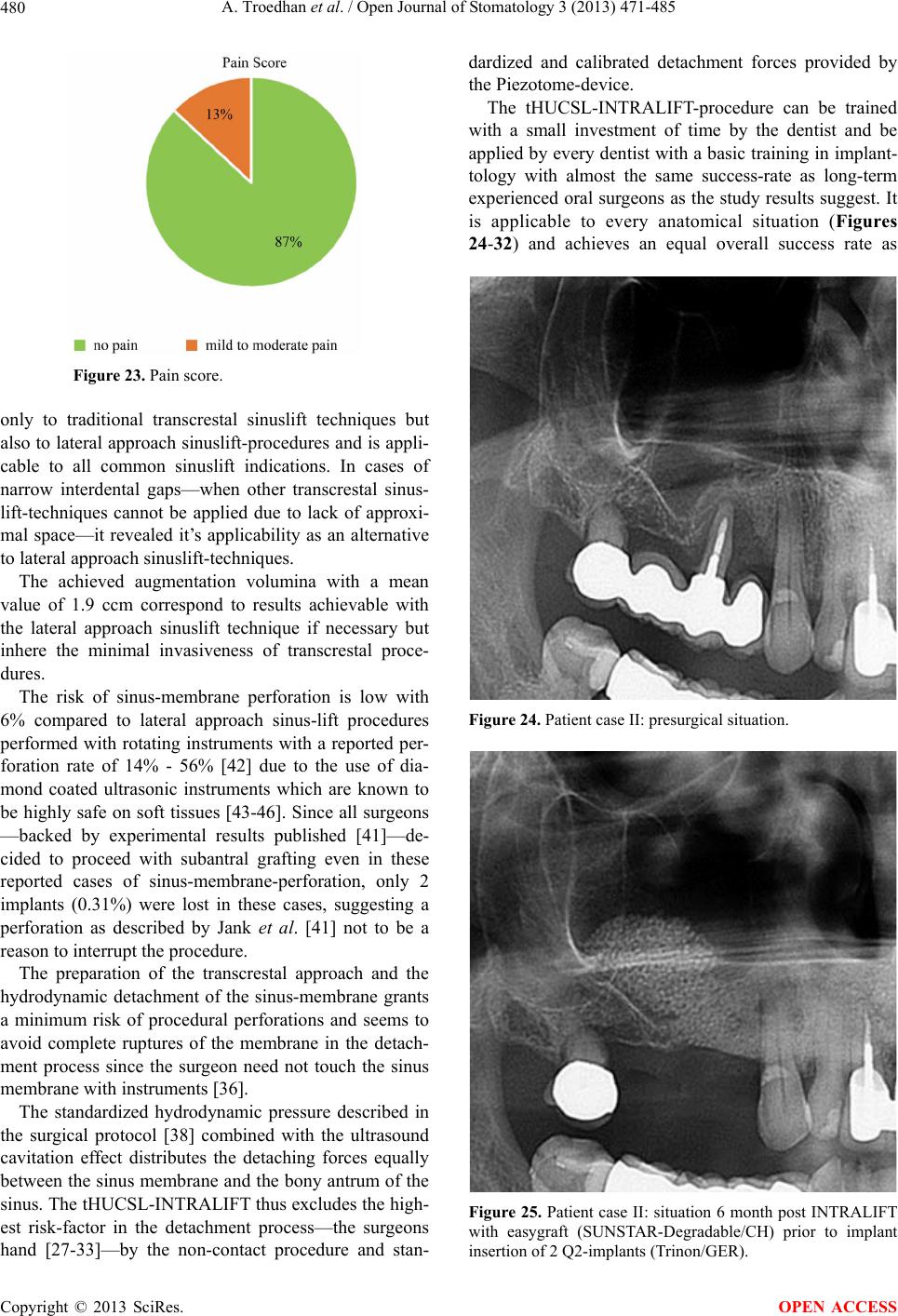 A. Troedhan et al. / Open Journal of Stomatology 3 (2013) 471-485 480 Figure 23. Pain score. only to traditional transcrestal sinuslift techniques but also to lateral approach sinuslift-procedures and is appli- cable to all common sinuslift indications. In cases of narrow interdental gaps—when other transcrestal sinus- lift-techniques cannot be applied due to lack of approxi- mal space—it revealed it’s applicability as an alternative to lateral approach sinuslift-techniques. The achieved augmentation volumina with a mean value of 1.9 ccm correspond to results achievable with the lateral approach sinuslift technique if necessary but inhere the minimal invasiveness of transcrestal proce- dures. The risk of sinus-membrane perforation is low with 6% compared to lateral approach sinus-lift procedures performed with rotating instruments with a reported per- foration rate of 14% - 56% [42] due to the use of dia- mond coated ultrasonic instruments which are known to be highly safe on soft tissues [43-46]. Since all surgeons —backed by experimental results published [41]—de- cided to proceed with subantral grafting even in these reported cases of sinus-membrane-perforation, only 2 implants (0.31%) were lost in these cases, suggesting a perforation as described by Jank et al. [41] not to be a reason to interrupt the procedure. The preparation of the transcrestal approach and the hydrodynamic detachment of the sinus-membrane grants a minimum risk of procedural perforations and seems to avoid complete ruptures of the membrane in the detach- ment process since the surgeon need not touch the sinus membrane with instruments [36]. The standardized hydrodynamic pressure described in the surgical protocol [38] combined with the ultrasound cavitation effect distributes the detaching forces equally between the sinus membrane and the bony antrum of the sinus. The tHUCSL-INTRALIFT thus excludes the high- est risk-factor in the detachment process—the surgeons hand [27-33]—by the non-contact procedure and stan- dardized and calibrated detachment forces provided by the Piezotome-device. The tHUCSL-INTRALIFT-procedure can be trained with a small investment of time by the dentist and be applied by every den tist with a basic training in implant- tology with almost the same success-rate as long-term experienced oral surgeons as the study results suggest. It is applicable to every anatomical situation (Figures 24-32) and achieves an equal overall success rate as Figure 24. Patient case II: presurgical situation. Figure 25. Patient case II: situation 6 month post INTRALIFT with easygraft (SUNSTAR-Degradable/CH) prior to implant insertion of 2 Q2-implants (Trinon/GER). Copyright © 2013 SciRes. OPEN ACCESS 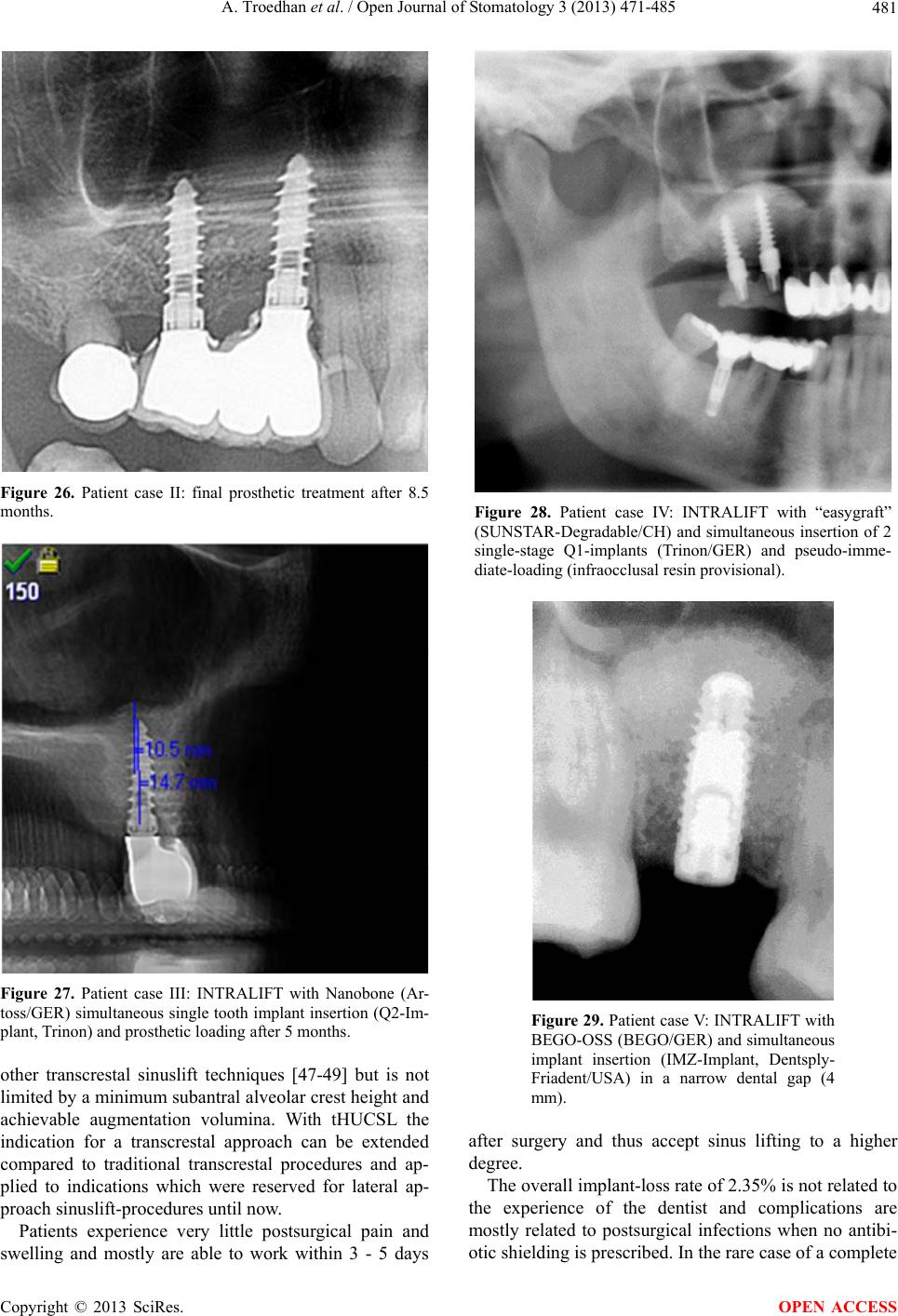 A. Troedhan et al. / Open Journal of Stomatology 3 (2013) 471-485 481 Figure 26. Patient case II: final prosthetic treatment after 8.5 months. Figure 27. Patient case III: INTRALIFT with Nanobone (Ar- toss/GER) simultaneous single tooth implant insertion (Q2-Im- plant, T rinon) and prosthetic loading after 5 months. other transcrestal sinuslift techniques [47-49] but is not limited by a minimum subantral alveolar crest height and achievable augmentation volumina. With tHUCSL the indication for a transcrestal approach can be extended compared to traditional transcrestal procedures and ap- plied to indications which were reserved for lateral ap- proach sinuslift-p rocedures until now. Patients experience very little postsurgical pain and swelling and mostly are able to work within 3 - 5 days Figure 28. Patient case IV: INTRALIFT with “easygraft” (SUNSTAR-Degradable/CH) and simultaneous insertion of 2 single-stage Q1-implants (Trinon/GER) and pseudo-imme- diate-loading (infraocclusal resin provisional). Figure 29. Patient case V: INTRALIFT with BEGO-OSS (BEGO/GER) and simultaneous implant insertion (IMZ-Implant, Dentsply- Friadent/USA) in a narrow dental gap (4 mm). after surgery and thus accept sinus lifting to a higher degree. The overall implant-loss rate of 2.35% is not related to the experience of the dentist and complications are mostly related to postsurgical infections when no antibi- otic shielding is prescribed. In the rare case of a complete Copyright © 2013 SciRes. OPEN ACCESS  A. Troedhan et al. / Open Journal of Stomatology 3 (2013) 471-485 482 Figure 30. Patient case VI: loosened old dental implant has to be removed. Figure 31. Patient case VI: immediately af- ter implant removal INTRALIFT was carried out with Nanobone (Artoss/GER) and simul- taneous implant insertion of 2 Q2-implants (Trinon/GER). rupture of the sinus-membrane or loss of the bone graft the procedure did not cause major inconveniences on the patient’s side and can be repeated after 3 - 5 months. The success-rate of the tHUCSL-INTRALIFT is in- dependent from the type and brand of used bone-graft- material as well as the type and brand of inserted im- plants as already generally described by Del Fabbro et al. for transcrestal sinus-floor elevation in a systematic re- view [47]. Especially in older patients the tHUCSL-INTRALIFT Figure 32. Patient case VI: prosthetic treat- ment after 7 months. enables simultaneous bilateral augmentations of the si- nus-floor without major surgical trauma thus widening the indication spectrum to a wider and older base of pa- tients with remaining subantral alveolar crest heights of 1 mm or less and proves the osteogenic capacity of the atraumatically detached sinus membrane independent from age [50] (Figures 33-36). The indication for a sinuslift procedure might be ques- tionable at subantral crest heights of 8 mm or more since a high reliability of short implants is discussed. Never- theless, the results of this study clearly show that two thirds of patients in need of implants in the lateral max- illa presented equal or less than 4 mm subantral alveolar crest-height thus being not eligible for treatment with short implants (Figure 15). 5. CONCLUSION The tHUCSL-INTRALIFT is compatible to all implant- systems with an implant—diameter of more than 3 mm and—most of all—applicable to all anatomical condi- tions of the alveolar crest and the maxillary sinus which can be considered a major advantage. Compared to other transcrestal instrument sets, balloon- or hydraulic-as- sisted sinuslift systems or “sinuslift”-implants that de- mand a minimum mesio-distal distance of the dentition gap and/or a subantral alveolar crest height of more than 4 mm, the results of this prospective study suggest the tHUCSL-INTRALIFT to be a safe and predictable alter- native also to lateral-approach sinuslift-techniques. It can be applied beginning with maxillary dentition gaps of a Copyright © 2013 SciRes. OPEN ACCESS 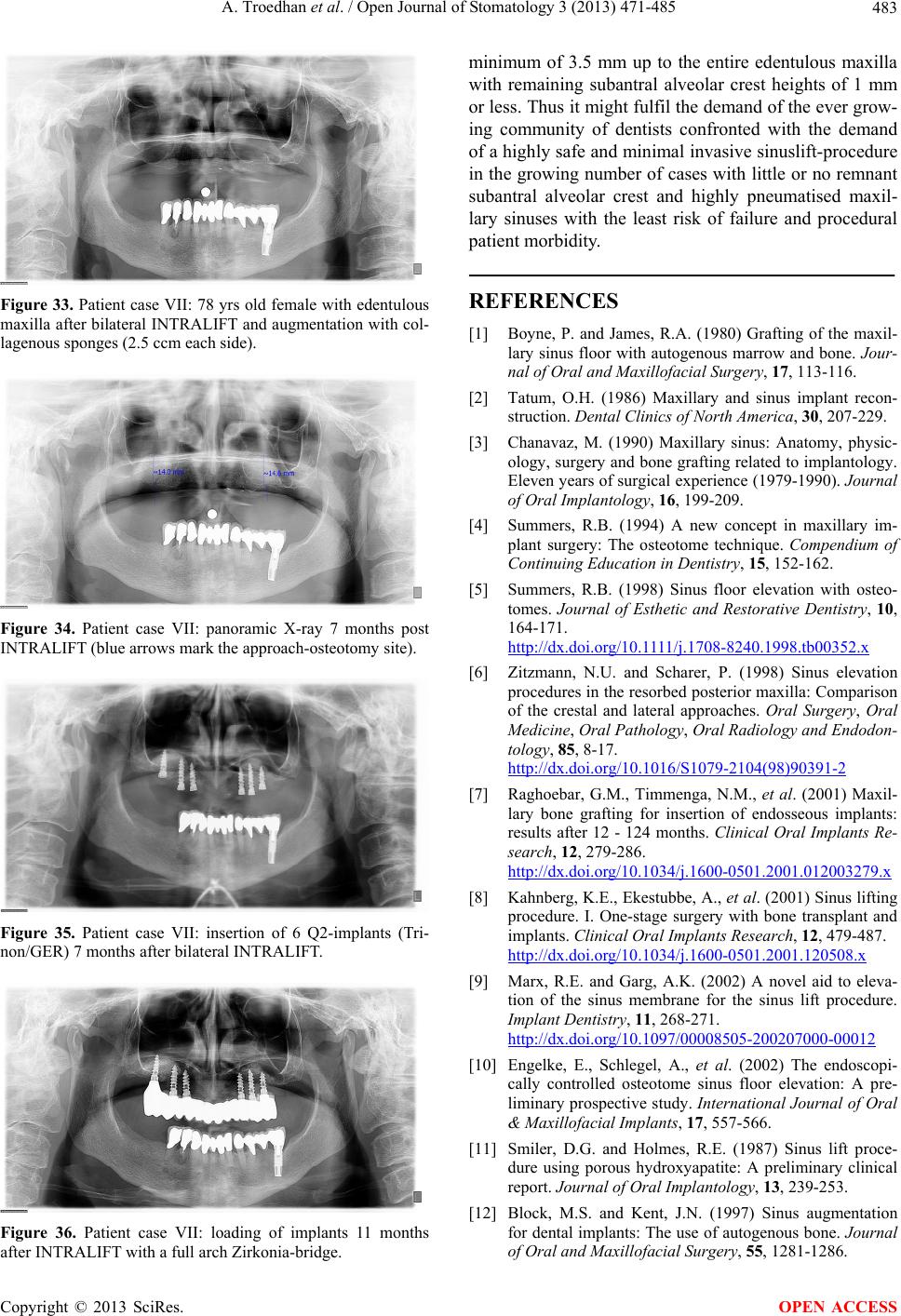 A. Troedhan et al. / Open Journal of Stomatology 3 (2013) 471-485 483 Figure 33. Patient case VII: 78 yrs old female with edentulous maxilla after bilateral INTRALIFT and augmentation with col- lagenous sponges (2.5 ccm each side). Figure 34. Patient case VII: panoramic X-ray 7 months post INTRALIFT (blue arrows mark the approach-osteotomy site). Figure 35. Patient case VII: insertion of 6 Q2-implants (Tri- non/GER) 7 months after bilateral INTRALIFT. Figure 36. Patient case VII: loading of implants 11 months after INTRALIFT with a full arch Zirkonia-bridge. minimum of 3.5 mm up to the entire edentulous maxilla with remaining subantral alveolar crest heights of 1 mm or less. Thus it might fulfil the demand of the ever grow- ing community of dentists confronted with the demand of a highly safe and minimal invasive sinuslift-procedure in the growing number of cases with little or no remnant subantral alveolar crest and highly pneumatised maxil- lary sinuses with the least risk of failure and procedural patient morbidity. REFERENCES [1] Boyne, P. and James, R.A. (1980) Grafting of the maxil- lary sinus floor with autogenous marrow and bone. Jour- nal of Oral and Maxillofacial Surgery, 17, 113-116. [2] Tatum, O.H. (1986) Maxillary and sinus implant recon- struction. Dental Clinics of North America, 30, 207-229. [3] Chanavaz, M. (1990) Maxillary sinus: Anatomy, physic- ology, surgery and bone grafting related to implantology. Eleven years of surgical experience (1979-1990). Journal of Oral Implantology, 16, 199-209. [4] Summers, R.B. (1994) A new concept in maxillary im- plant surgery: The osteotome technique. Compendium of Continuing Education in Dentistry, 15, 152-162. [5] Summers, R.B. (1998) Sinus floor elevation with osteo- tomes. Journal of Esthetic and Restorative Dentistry, 10, 164-171. http://dx.doi.org /10.1111/j.1708-8240.1998.tb00352.x [6] Zitzmann, N.U. and Scharer, P. (1998) Sinus elevation procedures in the resorbed posterior maxilla: Comparison of the crestal and lateral approaches. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodon- tology, 85, 8-17. http://dx.doi.org/10.1016/S1079-2104(98)90391-2 [7] Raghoebar, G.M., Timmenga, N.M., et al. (2001) Maxil- lary bone grafting for insertion of endosseous implants: results after 12 - 124 months. Clinical Oral Implants Re- search, 12, 279-286. http://dx.doi.org/10.1034/j.1600-0501.2001.012003279.x [8] Kahnberg, K.E., Ekestubbe, A., et al. (2001) Sinus lifting procedure. I. One-stage surgery with bone transplant and implants. Clinical Oral Implants Research, 12, 479-487. http://dx.doi.org/10.1034/j.1600-0501.2001.120508.x [9] Marx, R.E. and Garg, A.K. (2002) A novel aid to eleva- tion of the sinus membrane for the sinus lift procedure. Implant Dentistry, 11, 268-271. http://dx.doi.org/10.1097/00008505-200207000-00012 [10] Engelke, E., Schlegel, A., et al. (2002) The endoscopi- cally controlled osteotome sinus floor elevation: A pre- liminary prospective study. International Journal of Oral & Maxillofacial Implants, 17, 557-566. [11] Smiler, D.G. and Holmes, R.E. (1987) Sinus lift proce- dure using porous hydroxyapatite: A preliminary clinical report. Journal of Oral Implantology, 13, 239-253. [12] Block, M.S. and Kent, J.N. (1997) Sinus augmentation for dental implants: The use of autogenous bone. Journal of Oral and Maxillofacial Surgery, 55, 1281-1286. Copyright © 2013 SciRes. OPEN ACCESS  A. Troedhan et al. / Open Journal of Stomatology 3 (2013) 471-485 484 http://dx.doi.org/10.1016/S0278-2391(97)90185-3 [13] Van den Bergh, J.P.A., Ten Bruggenkate, C.M., et al. (2000) Anatomical aspects of sinus floor elevations. Cli- nical Oral Implants Research, 11, 256-265. http://dx.doi.org/10.1034/j.1600-0501.2000.011003256.x [14] Cordioli, G., Mazzocco, C., et al. (2001) Maxillary sinus floor augmentation using bioactive glass granules and autogenous bone with simultaneous implant placement. Clinical and histological findings. Clinical Oral Implants Research, 12, 270-278. http://dx.doi.org/10.1034/j.1600-0501.2001.012003270.x [15] Cammack, G., Nevins, M., et al. (2005) Histologic evalu- ation of mineralized and demineralized freeze-dried bone allograft for ridge and sinus augmentations. International Journal of Periodontics and Restorative Dentistry, 25, 231-237. [16] Zijderveld, S.A., Zerbo, I.R., et al. (2005) Maxillary sinus floor augmentation using a beta-tricalcium phosphate (Cerasorb) alone compared to autogenous bone grafts. International Journal of Oral & Maxillofacial Implants, 20, 432-440. [17] Szabo, G., et al. (2005) A prospective multicenter ran- domized clinical trial of autogenous bone versus beta- tricalcium phosphate graft alone for bilateral sinus eleva- tion: Histologic and histomorphometric evaluation. In- ternational Journal of Oral & Maxillofacial Implants, 20, 371-381. [18] Boyne, P.J., Lilly, L.C., et al. (2005) De novo bone in- duction by recombinant human bone morphogenetic pro- tein-2 (rhBMP-2) in maxillary sinus floor augmentation. Journal of Oral and Maxillofacial Surgery, 63, 1693-707. http://dx.doi.org/10.1016/j.joms.2005.08.018 [19] Kim, Y.-K., Yun, P.-Y., et al. (2009) Analysis of the healing process in sinus bone grafting using various graft- ing materials. Oral Surgery , Oral Medicine, Oral Pathol- ogy, Oral Radiology and Endodontology, 107, 204-211. http://dx.doi.org/10.1016/j.tripleo.2008.07.021 [20] Wallace, S.S. and Froum, S.J. (2003) Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Annals of Periodontology, 8, 328-343. http://dx.doi.org/10.1902/annals.2003.8.1.328 [21] Wilk, R.M. (1999) Physiology of the maxillary sinus. Oral & Maxillofacial Surgery Clinics of North America, 11, 15-19. [22] Solar, P., Geyerhofer, U., et al. (1999) Blood supply to the maxillary sinus relevant to sinus floor elevation pro- cedures. Clinical Oral Implants Research, 10, 34-44. http://dx.doi.org/10.1034/j.1600-0501.1999.100105.x [23] Lundgren, S., Anderson, S., et al. (2004) Bone reforma- tion with sinus membrane elevation: A new surgical tech- nique for maxillary sinus floor augmentation. Clinical Implant Dentistry and Related Research, 6, 165-173. [24] Celik D, Turan T, Kabukcuoglu F, et al. (2003) Bone induction capacity of the periosteum and neonatal dura in the setting of the zygomatic arch fracture model. Archives of Facial Plastic Surgery, 5, 301-308. http://dx.doi.org/10.1001/archfaci.5.4.301 [25] Ortak, T.O., et al. (2005) Osteogenic Capacities of periost grafts, periost flaps and prefabricated periosteal flaps: Ex- perimental study. Journal of Craniofacial Surgery, 16, 594-600. http://dx.doi.org/10.1097/01.scs.0000168773.71356.62 [26] Srouji, S., Kizhner, T., et al. (2009) The schneiderian membrane contains osteoprogenitor cells: In vivo and in vitro study. Calcified Tissue International, 84, 138-145. http://dx.doi.org/10.1007/s00223-008-9202-x [27] Hernández-Alfaro, F., Torradeflot, M.M., et al. (2008) Prevalence and management of Schneiderian membrane perforations during sinus-lift procedures. Clinical Oral Implants Research, 19, 91-98. [28] Greenstein, G., Cavallaro, J., et al. (2008) Clinical rec- ommendations for avoiding and managing surgical com- plications associated with implant dentistry: A review. Journal of Periodontology, 79, 1317-1329. http://dx.doi.org/10.1902/jop.2008.070067 [29] Anavi, Y., Allon, D.M., et al. (2008) Complications of maxillary sinus augmentations in a selective series of pa- tients. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology, 106, 34-38. http://dx.doi.org/10.1016/j.tripleo.2007.09.021 [30] Li, J. and Wang, H.L. (2008) Common implant-related advanced bone grafting complications: Classification, eti- ology, and management. Implant Dentistry, 17, 389-401. http://dx.doi.org/10.1097/ID.0b013e31818c4992 [31] Katranji, A., Fotek, P., et al. (2008) Sinus augmentation complications: Etiology and treatment. Implant Dentistry, 17, 339-349. http://dx.doi.org/10.1097/ID.0b013e3181815660 [32] Jerjes, W., Upile, T., et al. (2010) Experience in third molar surgery: An update. British Dental Journal, 209, E1. http://dx.doi.org/10.1038/sj.bdj.2010.581 [33] Waseem, J., Mohammed, E., et al. (2006) Experience versus complication rate in third molar surgery. Head & Face Medicine, 2, 14. http://dx.doi.org/10.1186/1746-160X-2-14 [34] Vercellotti, T., De Paoli, S., et al. (2001) The piezoelec- tric bony window osteotomy and sinus membrane eleva- tion: Introduction of a new technique for simplification of the sinus augmentation procedure. International Journal of Periodontics and Restorative Dentistry, 21, 561-567. [35] Kfir, E., Kfir, V., et al. (2006) Minimally invasive antral membrane balloon elevation followed by maxillary bone augmentation and implant fixation. Journal of Oral Im- plantology, 32, 26-33. http://dx.doi.org/10.1563/782.1 [36] Vitkov, L., Gellrich, N.C., et al. (2005) Sinus floor eleva- tion via hydraulic detachment and elevation of the Sch- neiderian membrane. Clinical Oral Implants Research, 16, 615-621. http://dx.doi.org /10.1111/j.1600-0501.2005.01161.x [37] Sotirakis, E.G. and Gonshor, A. (2005) Elevation of the maxillary sinus floor with hydraulic pressure. Journal of Oral Implantology, 31, 197-204. http://dx.doi.org/10.1563/1548-1336(2005)31[197:EOTM SF]2.0.CO;2 [38] Troedhan, A.C., Kurrek, A., et al. (2010) Hydrodynamic ultrasonic sinus floor elevation—An experimental study Copyright © 2013 SciRes. OPEN ACCESS  A. Troedhan et al. / Open Journal of Stomatology 3 (2013) 471-485 Copyright © 2013 SciRes. 485 OPEN ACCESS in sheep. Journal of Oral and Maxillofacial Surgery, 68, 1125-1130. http://dx.doi.org/10.1016/j.joms.2009.12.014 [39] Velázquez-Cayón, R., Romero-Ruiz, M.M., et al. (2012) Hydrodynamic ultrasonic maxillary sinus lift: Review of a new technique and presentation of a clinical case. Med- icina Oral Patologia Oral y Cirugia Bucal, 17, e271- e275. http://dx.doi.org/10.4317/medoral.17430 [40] Wainwright, M., Troedhan, A., et al. (2007) The IntraLift: A new minimal invasive ultrasonic technique for sinus grafting procedures. Implants, 3, 30-34. [41] Jank, S., Kurrek, A., et al. (2011) Rupture length of the sinus membrane after 1.2 mm puncture and surgical sinus elevation: An experimental animal cadaver study. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology, 112, 568-572. http://dx.doi.org/10.1016/j.tripleo.2010.11.014 [42] Wallace, S.S., Mazor, Z., et al. (2007) Schneiderian membrane perforation rate during sinus elevation using piezosurgery: Clinical results of 100 consecutive cases. International Journal of Periodontics and Restorative Dentistry, 27, 413-419. [43] Schaeren, S., Jaquiery, C., et al. (2008) Assessment of nerve damage using a novel ultrasonic device for bone cutting. Journal of Oral and Maxillofacial Surgery, 66, 593. http://dx.doi.org/10.1016/j.joms.2007.03.025 [44] Pavlíková, G., Foltán, R., et al. (2011) Piezosurgery in oral and maxillofacial surgery. International Journal of Oral and Maxillofacial Surgery, 40, 451-457. http://dx.doi.org/10.1016/j.ijom.2010.11.013 [45] Schlee, M., Steigmann, M., et al. (2006) Piezosurgery: basics and possibilities. Implant Dentistry, 15, 334-340. http://dx.doi.org/10.1097/01.id.0000247859.86693.ef [46] Seshan, H., Konuganti, K. and Zope, S. (2009) Piezosur- gery in periodontology and oral implantology. Journal of Indian Society of Periodontology, 13, 155-156. http://dx.doi.org/10.4103/0972-124X.60229 [47] Del Fabbro, M., Corbella, S., et al. (2012) Implant sur- vival rates after osteotome-mediated maxillary sinus aug- mentation: A systematic review. Clinical Implant Den- tistry and Related Research, 14, e159-e168. http://dx.doi.org /10.1111/j.1708-8208.2011.00399.x [48] Yeong-Wook, K., Yoon-Seon, K., et al. (2010) A retro- spective study of trans-crestal approach to maxillary si- nus floor-elevation and simultaneous implant placement. Journal of the Korean Academy of Implant Dentistry, 29, 1-9. [49] Tan, W.C., Lang, N.P., et al. (2008) A systematic review of the success of sinus floor elevation and survival of im- plants inserted in combination with sinus floor elevation Part II: Transalveolar technique. Journal of Clinical Pe- riodontology, 35, 241-254. [50] Troedhan, A., Kurrek, A., et al. (2012) Biological princi- ples and physiology of bone regeneration under the Sch- neiderian membrane after sinus lift surgery: A radiologi- cal study in 14 patients treated with the transcrestal hy- drodynamic ultrasonic cavitational sinus lift (intralift). In- ternational Journal of Dentistry, 2012, Ar t i c l e I D : 576238.
|