M. Millogo et al. / Open Journal of Stomatology 3 (2013) 465-470 469
the pleomorphic adenoma among non malignant tumors
of salivary glands could be explained by the cellular di-
versity of salivary glandular tissue. The pleomorphic
adenoma is indeed a mixed tumor. Its microscopy shows
epithelial and myoepithelial cells in an abundant stroma
with some chondroma or myxoid areas [2,5,16,17]. Ma-
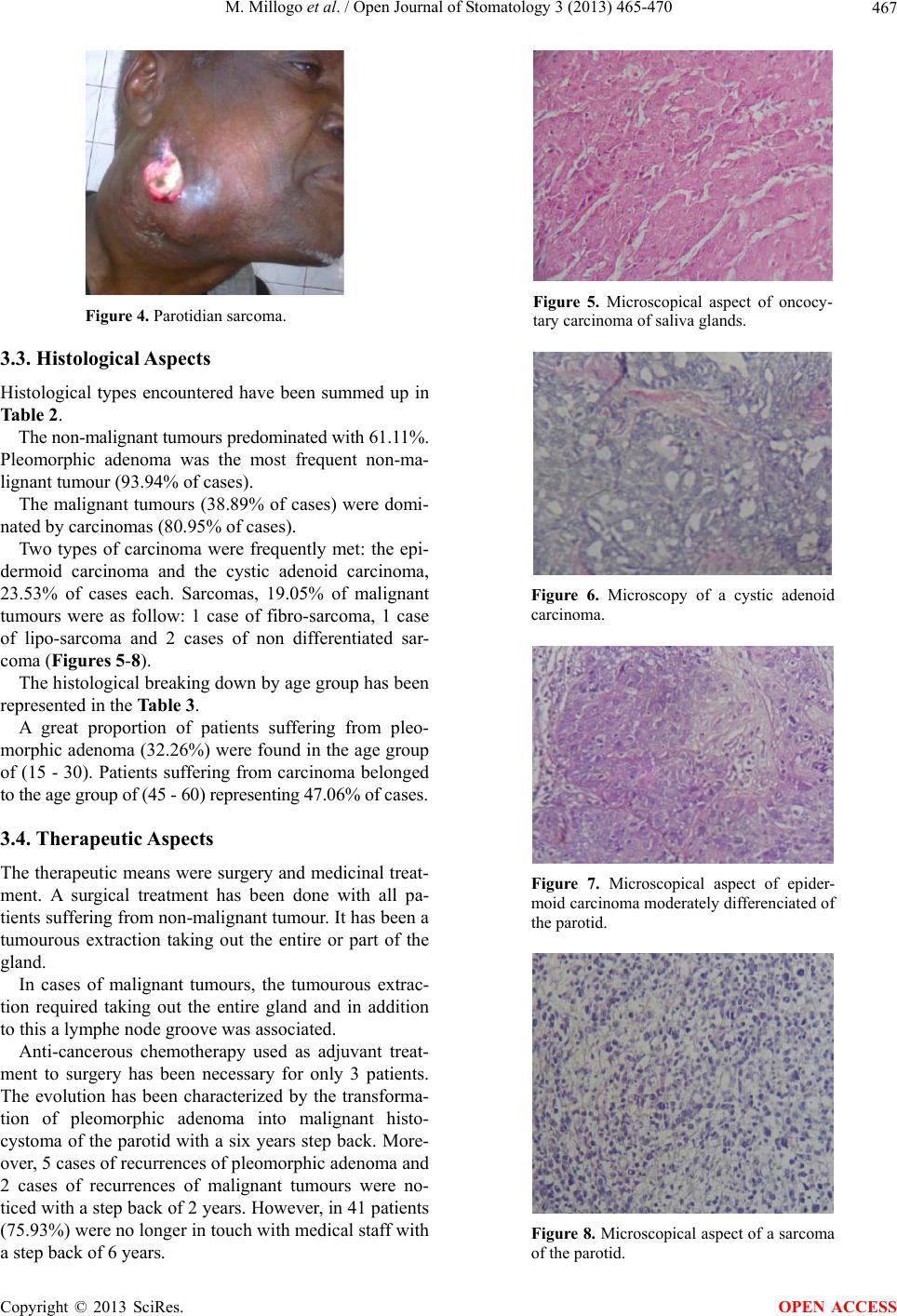
lignant tumours represented 38.89% of all the tumours
(80.95% of carcinomas and 19.05% of sarcomas). The
epithelial nature predominating in salivary glands cells
could explain the predominance of carcinoma [18,19].
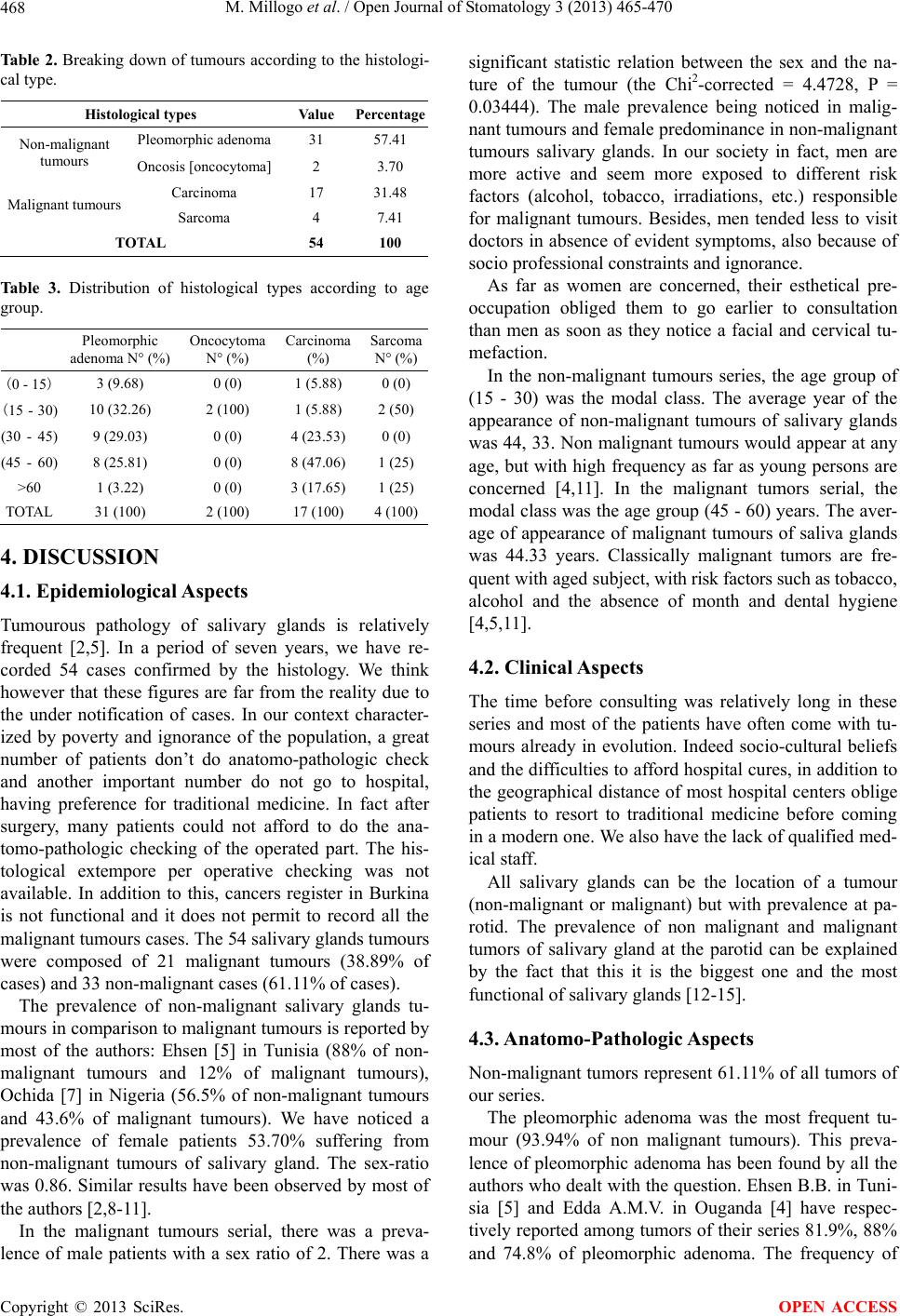
We have noticed in our series 9 different types of car-
cinomas dominated by the epidermoid carcinoma (23%,
53%) and adenoid cystic carcinoma (23.53%).
This histological diversity among malignant tumours
of salivary glands could be explained by the diversified
characteristic of salivary glands cells (epithelial interme-
diaries, acinous, oncosis, malpighian). There seems to be
a general agreement on the prevalence of carcinomas
among malignant tumours of salivary glands and on the
histological diversity of carcinomas. However, no histo-
logical form among carcinomas of salivary glands has
been considered as leading type of the file [5,7,18 - 20].
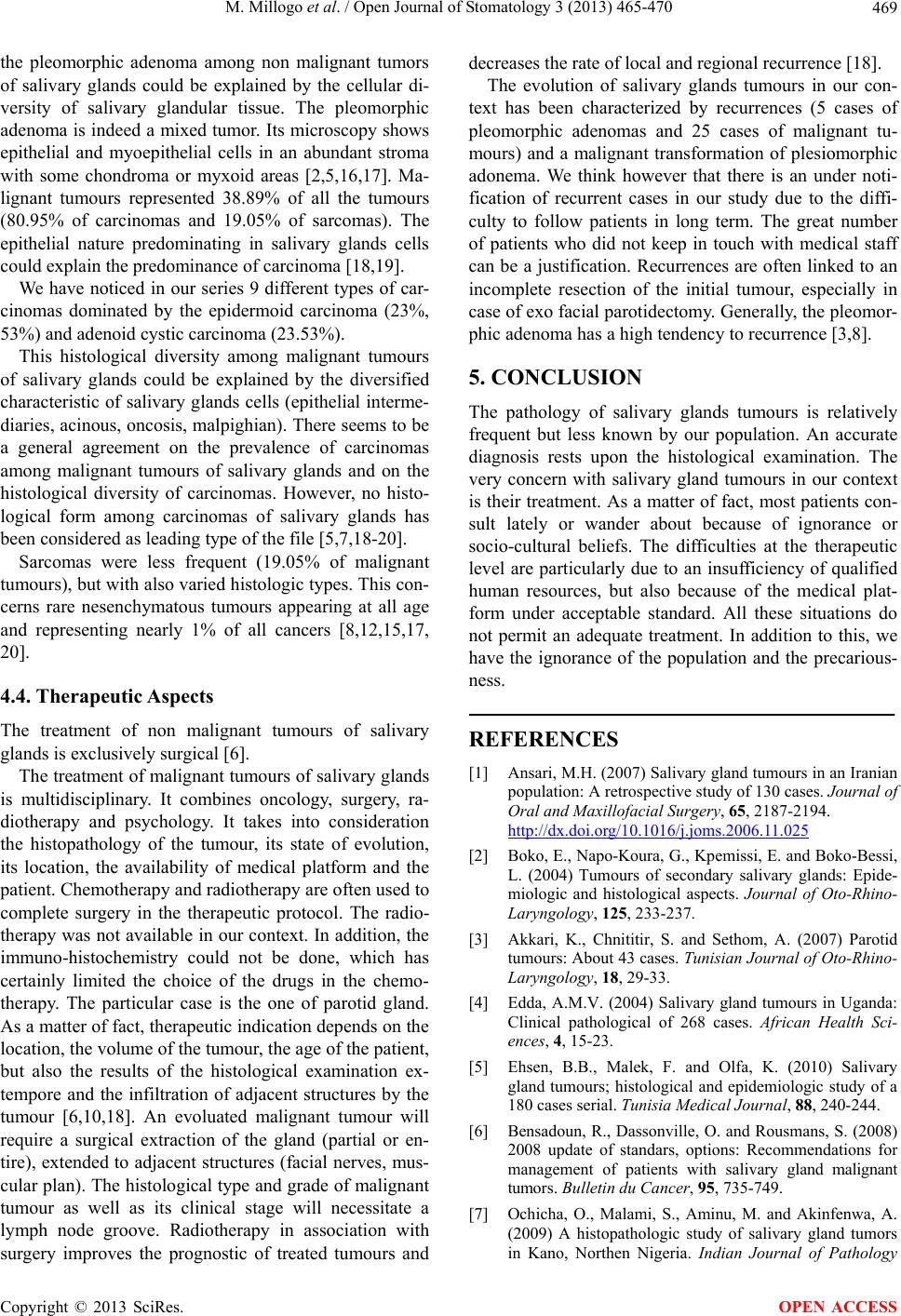
Sarcomas were less frequent (19.05% of malignant
tumours), but with also varied histolog ic types. This con-
cerns rare nesenchymatous tumours appearing at all age
and representing nearly 1% of all cancers [8,12,15,17,
20].
4.4. Therapeutic A spects
The treatment of non malignant tumours of salivary
glands is exclusively surgical [6].
The treatment of malignant tumours of salivary glands
is multidisciplinary. It combines oncology, surgery, ra-
diotherapy and psychology. It takes into consideration
the histopathology of the tumour, its state of evolution,
its location, the availability of medical platform and the
patient. Chemotherapy and radiotherapy are often used to
complete surgery in the therapeutic protocol. The radio-
therapy was not availab le in our context. In addition, th e
immuno-histochemistry could not be done, which has
certainly limited the choice of the drugs in the chemo-
therapy. The particular case is the one of parotid gland.
As a matter of fact, therapeutic indication depends on the
location, the volu me of the tumour, the age of the patient,
but also the results of the histological examination ex-
tempore and the infiltration of adjacent structures by the
tumour [6,10,18]. An evoluated malignant tumour will
require a surgical extraction of the gland (partial or en-
tire), extended to adjacent structures (facial nerves, mus-
cular plan). The histological type and grade of malignant
tumour as well as its clinical stage will necessitate a
lymph node groove. Radiotherapy in association with
surgery improves the prognostic of treated tumours and
decreases the rate of local and regional recurrence [18].
The evolution of salivary glands tumours in our con-
text has been characterized by recurrences (5 cases of
pleomorphic adenomas and 25 cases of malignant tu-
mours) and a malignant transformation of plesiomorphic
adonema. We think however that there is an under noti-
fication of recurrent cases in our study due to the diffi-
culty to follow patients in long term. The great number
of patients who did not keep in touch with medical staff
can be a justification. Recurrences are often linked to an
incomplete resection of the initial tumour, especially in
case of exo facial parotidectomy. Generally, the pleomor-
phic adenoma has a high tendency to recurrence [3,8].
5. CONCLUSION
The pathology of salivary glands tumours is relatively
frequent but less known by our population. An accurate
diagnosis rests upon the histological examination. The
very concern with salivary gland tumours in our context
is their treatment. As a matter of fact, most patients con-
sult lately or wander about because of ignorance or
socio-cultural beliefs. The difficulties at the therapeutic
level are particularly due to an insufficiency of qualified
human resources, but also because of the medical plat-
form under acceptable standard. All these situations do
not permit an adequate treatment. In addition to this, we
have the ignorance of the population and the precarious-
ness.
REFERENCES
[1] Ansari, M.H. (2007) Salivary gland tumours in an Iranian
population: A retrospective study of 130 cases. Journal of
Oral and Maxillofacial Surgery, 65, 2187-2194.
http://dx.doi.org/10.1016/j.joms.2006.11.025
[2] Boko, E., Napo-Koura, G., Kpemissi, E. and Boko-Bessi,
L. (2004) Tumours of secondary salivary glands: Epide-
miologic and histological aspects. Journal of Oto-Rhino-
Laryngology, 125, 233-237.
[3] Akkari, K., Chnititir, S. and Sethom, A. (2007) Parotid
tumours: About 43 cases. Tunisian Journal of Oto-Rhino-
Laryngology, 18, 29-33.
[4] Edda, A.M.V. (2004) Salivary gland tumours in Uganda:
Clinical pathological of 268 cases. African Health Sci-
ences, 4, 15-23.
[5] Ehsen, B.B., Malek, F. and Olfa, K. (2010) Salivary
gland tumours; histological and epidemiologic study of a
180 cases serial. Tunisia Medical Journal, 88, 240-244.
[6] Bensadoun, R., Dassonville, O. and Rousmans, S. (2008)
2008 update of standars, options: Recommendations for
management of patients with salivary gland malignant
tumors. Bulletin du Cancer, 95, 735-749.
[7] Ochicha, O., Malami, S., Aminu, M. and Akinfenwa, A.
(2009) A histopathologic study of salivary gland tumors
in Kano, Northen Nigeria. Indian Journal of Pathology
Copyright © 2013 SciRes. OPEN ACCESS