J. J. TONG ET AL.
Copyright © 2013 SciRes. ENG
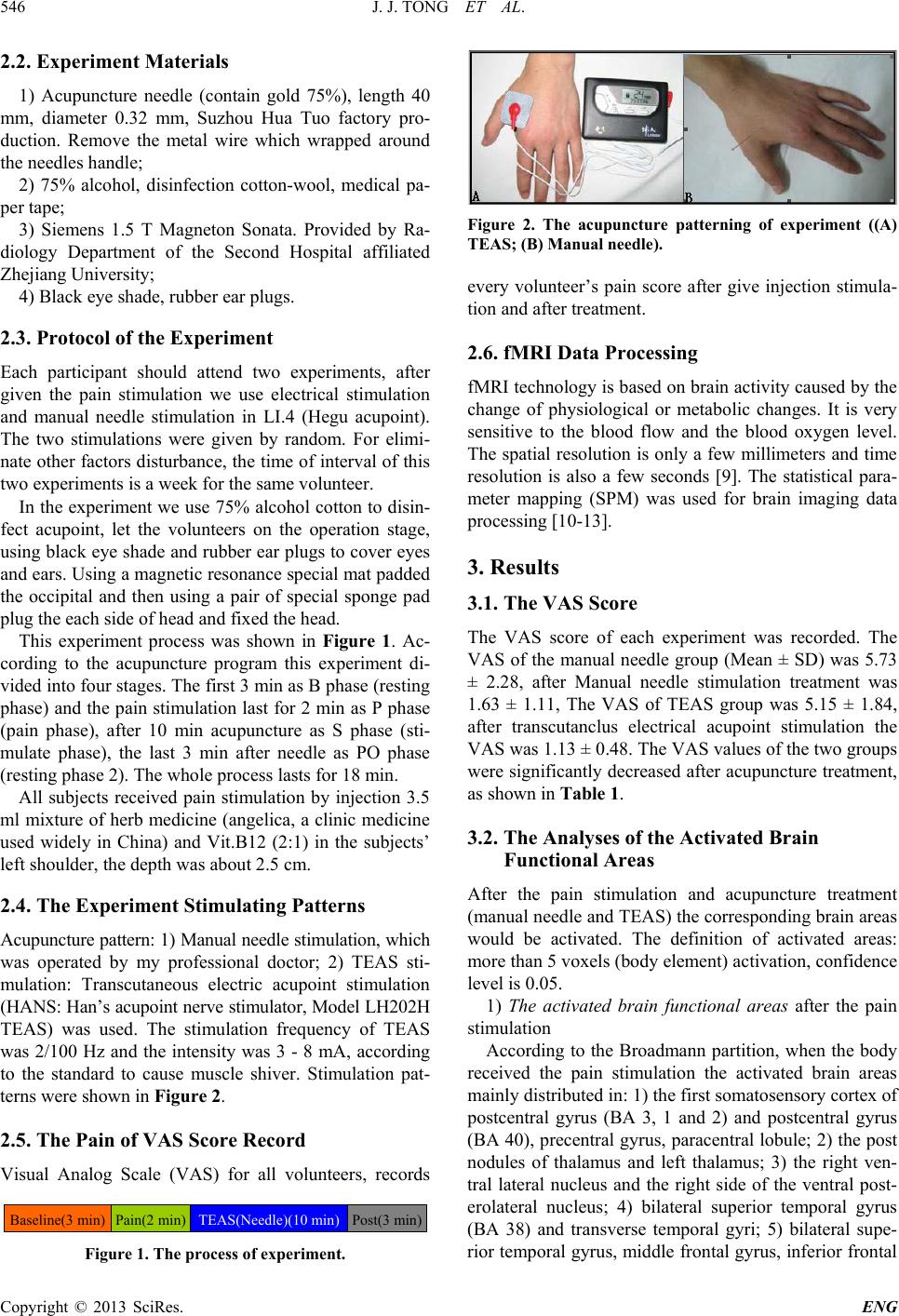
campus, the left of superior temporal gyrus, middle tem-
poral gyrus, supramarginal gyrus, angular gyrus, left of
the superior parietal lobule and inferior parietal lobule.
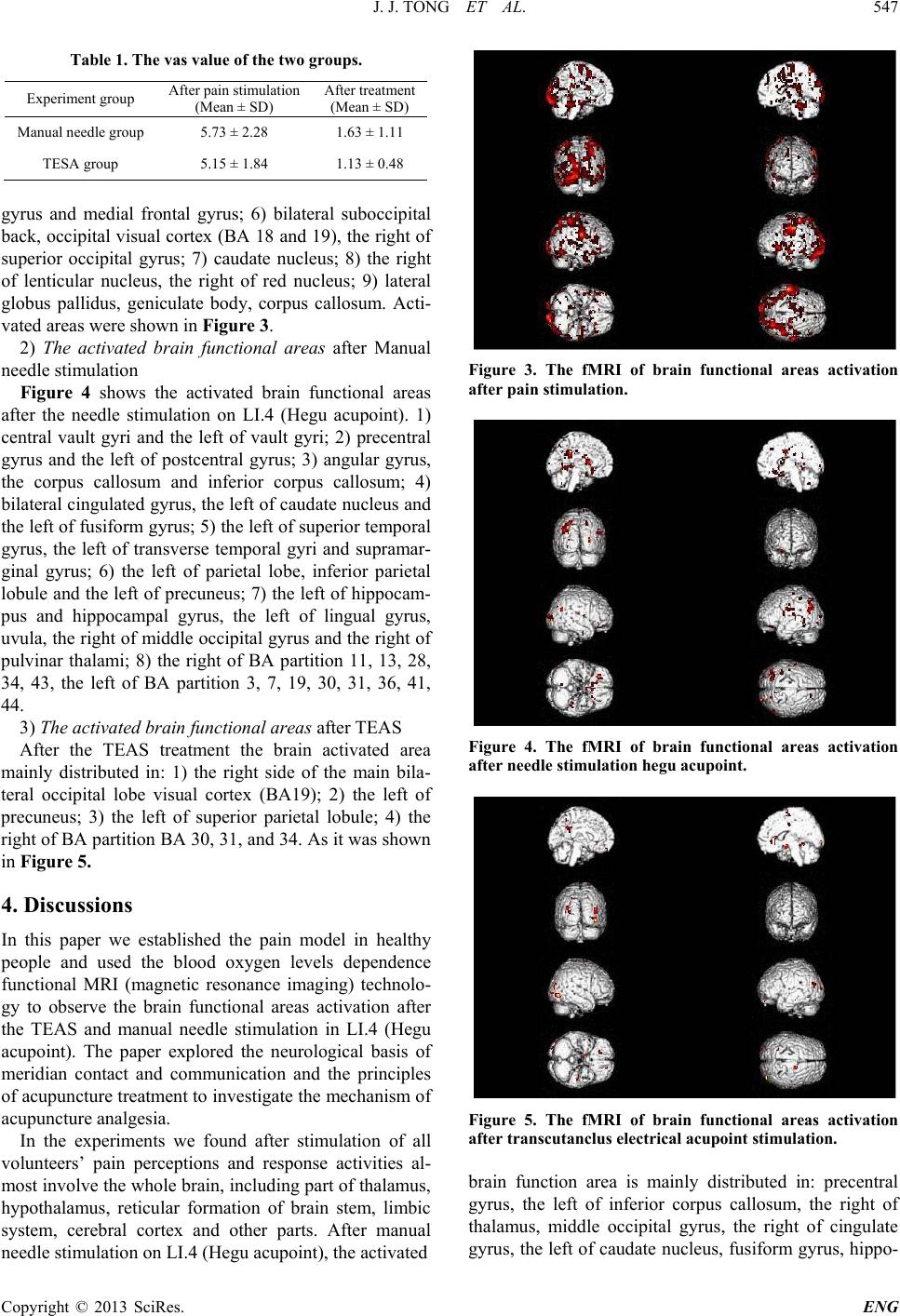
But after the TEAS on LI.4 (Hegu acupoint), the acti-
vated brain functional area is mainly distributed in: the
right side of the main bilateral occipital lobe visual cor-
tex (BA19), anterior cingulated, hippocampal gyrus, left
of the precuneus and the BA partition of 30, 31, 34. Ma-
nual needle stimulation and transcutaneous electrical sti-
mulation of acupuncture analgesia through activate the
multiple brain areas related pain modulation and then to
realize, but manual needle stimulation activation area is
wider than TEAS, and the degree of activate is stronger.
5. Conclusion
Studies have shown that acupuncture (manual needle
stimulation and TEAS) is an effective means in pain re-
lief. Acupuncture analgesia mainly through activating the
multiple brain areas related pain modulation, but the ac-
tivated brain functional area is different between TEAS
and manual needle stimulation. Transcutaneou s electrical
acupoint stimulation mainly activated the right side of
the cerebral cortex-based, while the ordinary manual need-
le stimulation activated the wider areas.
6. Acknowledgements
The research was supported by the Natural Science
Foundation of Zhejiang Province. The authors would like
to appreciate their thanks to them.
REFERENCES
[1] R. Kakigi, et al., “Electrophysiological Study on Human
Pain Perception,” Cli nical Neurophysiology, Vol. 116, No.
4, 2005, pp. 743-763.
http://dx.doi.org/10.1016/j.clinph.2004.11.016
[2] A. C. N. Chen, “New Perspectives in EEG-MEG Brain
Mapping and PET-fMRI Neuroimaging of Human Pain,”
International Journal of Psychophysiology, Vol. 42, No.
2, 2001, pp. 147-159.
http://dx.doi.org/10.1016/S0167-8760(01)00163-5
[3] J. S. Han, “Essentials of Neuroscience,” Joint Publishing
House of Beijing Medical University and Beijing Xiehe
Medical University, Beijing, 1993, p. 535.
[4] L. P. Yan, M. A. Cheng, S. D. LI, et al., “Thinking and
Proposal Concerning Clinical Studies and Application of
Acupuncture Analgesia,” Chinese Acupuncture & Mox-
ibustion, Vol. 24, No. 12, 2004, pp. 869-871.
[5] A. C. N. Chen, “Human Brain Measures of Clinical Pain:
A Review: II. Tomographic Imagings,” Pain, Vol. 54,
No. 2, 1993, pp. 133-144.
http://dx.doi.org/10.1016/0304-3959(93)90201-Y
[6] K. L. Casey, “Forebrain Mechanisms of Nociception and
Pain: Analysis through Imaging,” Proceedings of the Na-
tional Academy of Sciences of the United States of Amer-
ica, Vol. 96, No. 14, 1999, pp. 7668-7674.
http://dx.doi.org/10.1073/pnas.96.14.7668
[7] K. L. Casey, “Concepts of Pain Mechanisms: The Con-
tribution of Functional Imaging of the Human Brain,”
Progress in Brain R e search, Vol. 129, 2000, pp. 277-287.
http://dx.doi.org/10.1016/S0079-6123(00)29020-1
[8] R. P. Pawl, “A Review of Functional Imaging of the
Brain and Pain,” Current Review of Pain, Vol. 3, No. 4,
1999, pp. 249-255.
http://dx.doi.org/10.1007/s11916-999-0042-9
[9] P. Jezzard, P. M. Matthews and S. M. Smith, “Functional
MRI: An Introduction to Methods,” Oxford University
Press, 2003.
[10] H. M. Zhang and S. Z. Cheng, “A New Brain Imaging
Analysis Method—Statistic Parameters Mapping (SPM),”
Chinese Journal of Medical Imaging Technology , Vol. 18,
No. 7, 2002, pp. 711-713.
[11] Y. X. Luo, Y. Y. Tang, L. F. Wu, et al., “Brain Imaging
Analysis Software SPM Introduction,” Chinese Journal
of Medical Imaging Technology, Vol. 19, No. 7, 2003, pp.
926-928.
[12] Y.-G. Wu and K. Li, “Basic Principle of SPM: An Intro-
duction-Part: Review in Basic Mathematic Principle,”
Chinese Journal of Medical Imaging Technol ogy, Vol. 20,
No. 11, 2004, pp. 1768-1771.
[13] Y.-G. Wu and K. Li, “Basic Principle of SPM: An Intro-
duction-Part: Applications to PET and fMRI,” Chinese
Journal of Medical Imaging Technology, Vol. 20, No. 11,
2004, pp. 1772-1773.