 Advances in Infectious Diseases, 2013, 3, 300-305 Published Online December 2013 (http://www.scirp.org/journal/aid) http://dx.doi.org/10.4236/aid.2013.34046 Open Access AID Healthcare Associated Infection in the Neonatal Intensive Care Unit of King Abdl Aziz Specialist Hospital, Taif, KSA A. K. Al-Zahrani1, E. M. Eed2, A. A. Alsulaimani3, S. H. Abbadi4* 1Department Pediatrics, College of Medicine Taif University, Neonatal Intensive Care Unit King Abdulaziz Specialist Hospital, Taif, KSA; 2Department of Medical Microbiology and Immunology, Faculty of Medicine Menoufia University, Egypt and College of Ap- plied Medical Sciences Taif University, Taif, KSA; 3Associate Prof. Medical College, Consultant Pediatrician & Neonatologist, Taif University, Taif, KSA; 4Department of Medical Microbiology and Immunology, Faculty of Medicine Suez Canal University, Egypt and College of Medicine, Taif University, KSA. Email: *saidabbadi@tu.edu.sa Received October 13th, 2013; revised November 13th, 2013; accepted November 20th, 2013 Copyright © 2013 A. K. Al-Zahrani et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Healthcare-associated infection is a common problem of newborn in neonatal intensive care units. It results in high mortality rate and serious complications. The Aim: to assess the incidence, etiology and the mortality of healthcare- associated infections of patients in neonatal intensive care unit at King Abdl Aziz Specialist Hospital (KAASH), Taif, Kingdom of Saudi Arabia. Material and Methods: This is a retrospective study including 8033 neonates admitted to neonatal intensive care unit during period between April, 2006 and December, 2012. The health-care associated infec- tion rate, mortality rate, causative organism and risk factors were studied. Results: The prevalence of health-care asso- ciated infection was found to be 6.03%; the mortality rate was 27.1%. The highest prevalence was among children with the birth weight below 1000 g. The most frequent causative pathogen was klebseilla spp, followed by other gram nega- tive bacilli. Conclusion: The rate of healthcare-associated infections in neonatal intensive care unit at KAASH was relatively high. In addition, the mortality rate was observed to be high (27.1%) owing to the high virulence of the causa- tive organisms. Keywords: Healthcare-Associated Infection; Newborn; Neonatal Intensive Care Unit 1. Introduction Health-care associated infections (HAIs) continue to be a major public health problem throughout the world, espe- cially in the neonatal intensive care unit (NICU). Neo- nates in the NICU are a very vulnerable group due to de- fective immunity and the increasing number of technol- ogy dependant infants [1,2]. Deficiencies of both innate and adaptive immunity contribute to the impaired neona- tal host defense [3]. A domination of naive immune cells, functional impairments and lower leukocyte subset num- bers contribute further to an increased susceptibility [4,5]. The mode of infection transmission is mainly through the care-giver staff specially if the proper antiseptic meas- ures are not considered [4]. Infection control for prevent- ing nosocomial infections may play an important role in reducing medical costs, period of hospital stay, and mor- tality in hospitalized patients [6]. Sepsis in the newborn is classified into early-onset form (EONS), within the first 72 hours of life, and late- onset form (LONS), which takes place afterwards (3). HAI in the NICU takes many forms, and the most frequent forms are the blood stream infection (septicemia) (28%), ventilator associated pneumonia (21%). Meningitis, gas- tro-enteritis, skin and eye infections are also common infections [7]. Many risk factors of HAI in the NICU are involved. The most important is excessive invasive pro- cedures such as peripheral cannulation, central venous catheter placement, tracheal incubation and ventilation [6]. Furthermore, the duration of hospital stay, plays an important role; that is, the longer the stay, the higher the incidence of HAI [7]. Premature infants, with a birth weight less than 1000 g (ELBW: extremely low birth weight infants), are particularly predisposed to sepsis, as there is an inverse correlation between gestational age, birth weight, and sepsis [8,9]. Furthermore, the age of the neonate has a role in the incidence of HAI. Previous stu- *Corresponding author.  Healthcare Associated Infection in the Neonatal Intensive Care Unit of King Abdl Aziz Specialist Hospital, Taif, KSA 301 dies have shown that the peak incidence of infection oc- curred between the age of 10th and 20th day [2]. Many organisms are involved in neonatal HAI, and the commonest are E. coli (36.6%), Staphylococcusaureus (29.5%), Pseudomonas spp (22.4%), Klebsiella spp (7.6%) and Proteus spp (3.8%). St pneumoniae, entero- cocci and Serratia are also involved [10,11]. In spite of the high prevalence and severity of neonatal HAI, the ho- spital represents a well established reservoir for resistant organisms that makes the problem difficult to control, and neonatal HAI is still a preventable problem, as risk factors can potentially be employed to develop local strategy for prevention [12]. This could be achieved through strict antiseptic measures for environment, staff, equipment, and minimizing invasive procedures [13]. These perfect control measures require proper epidemi- ological studies and tracing of infection [14]. The princi- pal method of diagnosing sepsis is the isolation of causa- tive organisms from blood cultures and antimicrobial sus- ceptibility testing [15,16]. Results are usually available between 48 - 72 hours after specimen collection and therefore, initial antimicrobial treatment has been usually empirical with the aim that the most likely pathogens would be susceptible to the chosen drugs [15]. Therefore, this study was conducted in order to investigate the epi- demiological characteristics of HAI in the aspects of in- fection rate, common pathogens and risk factors in our NICU in order to guide empirical therapy and improve bet- ter preventive measures. 2. Subjects and Methods 2.1. Clinical Setting and Patients Population This is a retrospective, hospital-based study. It was car- ried out in the neonatal intensive care unit (NICU) at King Abdul Aziz Specialist Hospital (KAASH), Taif, Kingdom of Saudi Arabia during the period April 2006 - December, 2012. KAASH is a 500-bed tertiary-level hos- pital. The NICU is a level III nursery with 60 bed ca- pacity, dealing with all cases delivered in the hospital that ranges between 12,000 to 14,000 deliveries each year. Data were collected from the medical records in stan- dardized collection sheets and included demographic data, birth weight, gestational age, gender, outcome, and delivery data (mode of delivery, maturity). The preva- lence of sepsis was calculated by dividing the number of newborns with sepsis by the total number of newborns admitted to the NICU. 2.2. Case Definition Health care associated sepsis, defined as a positive blood culture taken after 48 hours of admission to NICU with presence of clinical signs that are suggestive of neonatal septicemia [12]. 2.3. Culture and Susceptibility Each neonate showing manifestation of sepsis was sub- jected to sampling for blood culture, cerebrospinal fluid (CSF) culture, or other samples according the clinical presentation. Blood culture was done for all neonates who were suspected to have sepsis. All blood samples were collected from the peripheral vein under strict asep- tic precautions, before starting antibiotic therapy. Blood culture samples were incubated in the BacT/ALERT 3D (bioMerieux, France), sub-cultures were done on blood agar, chocolate agar, Mannitol salt agar and Mac Con- key’s agar plates (Oxoid) and incubated at 37˚C for 24 - 48 hours. The bacterial isolates were identified by stan- dard laboratory techniques, using standard culture media and biochemical reactions according to the Clinical La- boratory Standard Institute (CLSI) criteria. Thereafter, antibiotic susceptibility testing was performed on Muller Hinton agar (Oxoid) by Kirby-Bauer disk diffusion me- thod and interpreted according to CLSI criteria [17]. Data were analyzed using SPSS software (Version 10.0; SPSS Inc., Chicago). 3. Results Tab le 1 shows that during the study period (April, 2006- December, 2012) the total number of the patients admit- ted to the neonatal intensive care unit were 8033 neo- nates. The total HAI rate in our ICU was 6.03%. Being highest in year 2006 followed by year 2007. While was lowest in year 2008. There were a total 484 health care associated infections, of them 258 infant were males and 226 were females. The studied newborn were categorized acceding to the birth weight into four groups group I (less than 1000 g), group II (1000 - 1500 g), group III (1501 - 2500 g) and group IV (more than 2500 g). The results showed different HAI rate among four birth weight groups. The highest rate (29.54%) was found in patients with weight below 1000 g, and was 26.65% in group II, 28.7% in group III while, the HAI rate among the fourth group was only 14% (Table 2). Also, the studied newborn were categorized acceding to the gestational age in weeks into four groups group I (less than 28 w), group II (28 - 31 w + 6 days), group III (32 - 36 w + 6 days) and group IV (equal or more than 37 w) (Table 2). During the study period, the most com- mon recovered organism was klebseilla spp (128 isolates) followed by Enterobacter spp species, E. coli and Acine- tobacterspp (79, 78 and 72 isolates respectively. Whereas gram positive cocci as CoNS, Staphylococcus aureus and Enterococcus were less frequent (31, 9, and 7 isolates re- spectively) (Table 3). Open Access AID 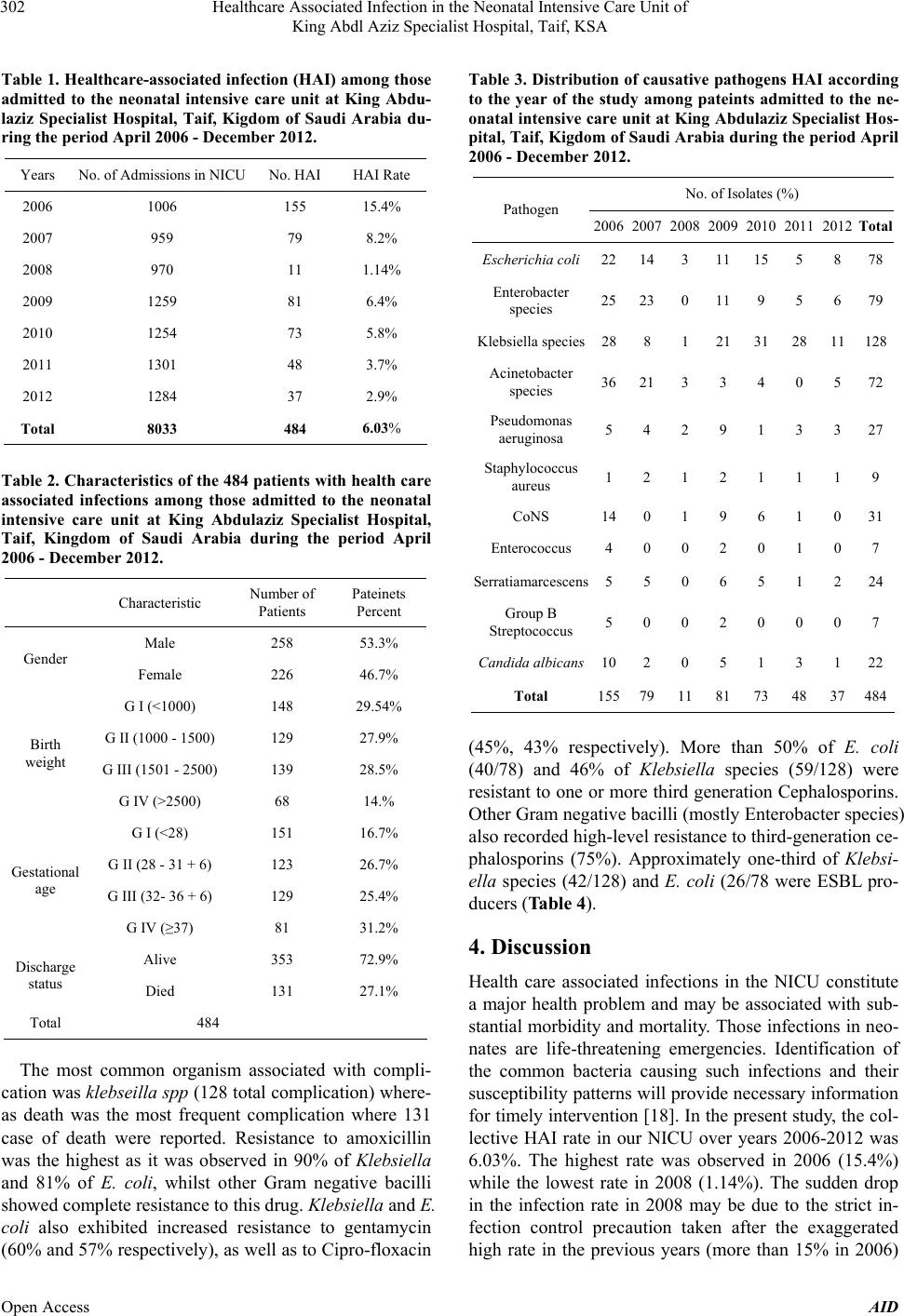 Healthcare Associated Infection in the Neonatal Intensive Care Unit of King Abdl Aziz Specialist Hospital, Taif, KSA 302 Table 1. Healthcare-associated infection (HAI) among those admitted to the neonatal intensive care unit at King Abdu- laziz Specialist Hospital, Taif, Kigdom of Saudi Arabia du- ring the period April 2006 - December 2012. Years No. of Admissions in NICU No. HAI HAI Rate 2006 1006 155 15.4% 2007 959 79 8.2% 2008 970 11 1.14% 2009 1259 81 6.4% 2010 1254 73 5.8% 2011 1301 48 3.7% 2012 1284 37 2.9% Total 8033 484 6.03% Table 2. Characteristics of the 484 patients with health care associated infections among those admitted to the neonatal intensive care unit at King Abdulaziz Specialist Hospital, Taif, Kingdom of Saudi Arabia during the period April 2006 - December 2012. Characteristic Number of Patients Pateinets Percent Male 258 53.3% Gender Female 226 46.7% G I (<1000) 148 29.54% G II (1000 - 1500) 129 27.9% G III (1501 - 2500) 139 28.5% Birth weight G IV (>2500) 68 14.% G I (<28) 151 16.7% G II (28 - 31 + 6) 123 26.7% G III (32- 36 + 6) 129 25.4% Gestational age G IV (≥37) 81 31.2% Alive 353 72.9% Discharge status Died 131 27.1% Total 484 The most common organism associated with compli- cation was klebseilla spp (128 total complication) where- as death was the most frequent complication where 131 case of death were reported. Resistance to amoxicillin was the highest as it was observed in 90% of Klebsiella and 81% of E. coli, whilst other Gram negative bacilli showed complete resistance to this drug. Klebsiella and E. coli also exhibited increased resistance to gentamycin (60% and 57% respectively), as well as to Cipro-floxacin Table 3. Distribution of causative pathogens HAI according to the year of the study among pateints admitted to the ne- onatal intensive care unit at King Abdulaziz Specialist Hos- pital, Taif, Kigdom of Saudi Arabia during the period April 2006 - December 2012. No. of Isolates (%) Pathogen 2006 2007 2008 2009 2010 2011 2012Total Escherichia coli2214 3 11 15 5 8 78 Enterobacter species 2523 0 11 9 5 6 79 Klebsiella species288 1 21 31 28 11128 Acinetobacter species 36213 3 4 0 5 72 Pseudomonas aeruginosa 5 4 2 9 1 3 3 27 Staphylococcus aureus 1 2 1 2 1 1 1 9 CoNS 140 1 9 6 1 0 31 Enterococcus 4 0 0 2 0 1 0 7 Serratiamarcescens5 5 0 6 5 1 2 24 Group B Streptococcus 5 0 0 2 0 0 0 7 Candida albican s102 0 5 1 3 1 22 Total 15579 11 81 73 48 37484 (45%, 43% respectively). More than 50% of E. coli (40/78) and 46% of Klebsiella species (59/128) were resistant to one or more third generation Cephalosporins. Other Gram negative bacilli (mostly Enterobacter species) also recorded high-level resistance to third-generation ce- phalosporins (75%). Approximately one-third of Klebsi- ella species (42/128) and E. coli (26/78 were ESBL pro- ducers (Table 4). 4. Discussion Health care associated infections in the NICU constitute a major health problem and may be associated with sub- stantial morbidity and mortality. Those infections in neo- nates are life-threatening emergencies. Identification of the common bacteria causing such infections and their susceptibility patterns will provide necessary information for timely intervention [18]. In the present study, the col- lective HAI rate in our NICU over years 2006-2012 was 6.03%. The highest rate was observed in 2006 (15.4%) while the lowest rate in 2008 (1.14%). The sudden drop in the infection rate in 2008 may be due to the strict in- fection control precaution taken after the exaggerated high rate in the previous years (more than 15% in 2006) Open Access AID 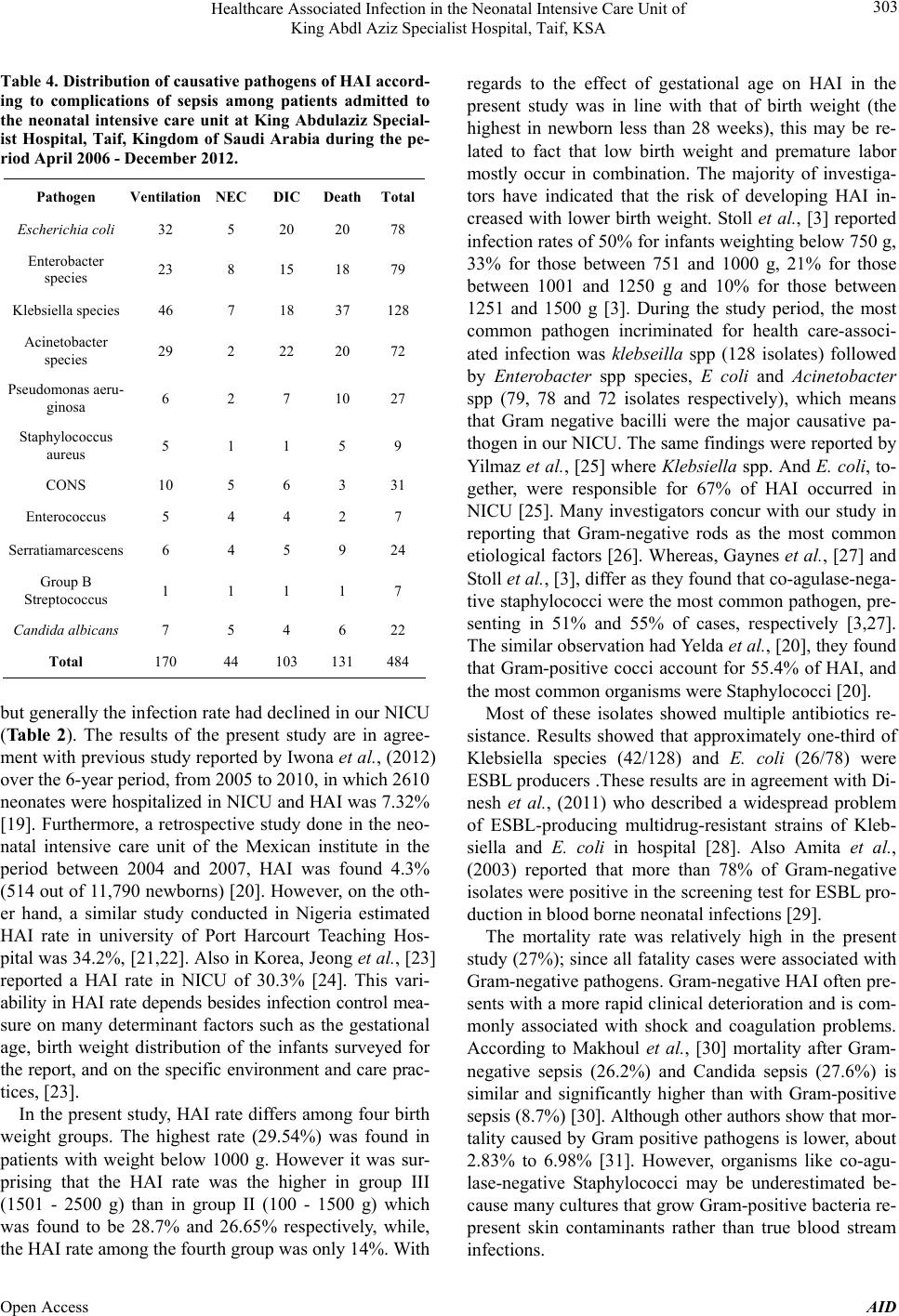 Healthcare Associated Infection in the Neonatal Intensive Care Unit of King Abdl Aziz Specialist Hospital, Taif, KSA 303 Table 4. Distribution of causative pathogens of HAI accord- ing to complications of sepsis among patients admitted to the neonatal intensive care unit at King Abdulaziz Special- ist Hospital, Taif, Kingdom of Saudi Arabia during the pe- riod April 2006 - December 2012. Pathogen Ventilation NEC DIC DeathTotal Escherichia coli 32 5 20 20 78 Enterobacter species 23 8 15 18 79 Klebsiella species 46 7 18 37 128 Acinetobacter species 29 2 22 20 72 Pseudomonas aeru- ginosa 6 2 7 10 27 Staphylococcus aureus 5 1 1 5 9 CONS 10 5 6 3 31 Enterococcus 5 4 4 2 7 Serratiamarcescens 6 4 5 9 24 Group B Streptococcus 1 1 1 1 7 Candida albican s 7 5 4 6 22 Total 170 44 103 131 484 but generally the infection rate had declined in our NICU (Ta bl e 2 ). The results of the present study are in agree- ment with previous study reported by Iwona et al., (2012) over the 6-year period, from 2005 to 2010, in which 2610 neonates were hospitalized in NICU and HAI was 7.32% [19]. Furthermore, a retrospective study done in the neo- natal intensive care unit of the Mexican institute in the period between 2004 and 2007, HAI was found 4.3% (514 out of 11,790 newborns) [20]. However, on the oth- er hand, a similar study conducted in Nigeria estimated HAI rate in university of Port Harcourt Teaching Hos- pital was 34.2%, [21,22]. Also in Korea, Jeong et al., [23] reported a HAI rate in NICU of 30.3% [24]. This vari- ability in HAI rate depends besides infection control mea- sure on many determinant factors such as the gestational age, birth weight distribution of the infants surveyed for the report, and on the specific environment and care prac- tices, [23]. In the present study, HAI rate differs among four birth weight groups. The highest rate (29.54%) was found in patients with weight below 1000 g. However it was sur- prising that the HAI rate was the higher in group III (1501 - 2500 g) than in group II (100 - 1500 g) which was found to be 28.7% and 26.65% respectively, while, the HAI rate among the fourth group was only 14%. With regards to the effect of gestational age on HAI in the present study was in line with that of birth weight (the highest in newborn less than 28 weeks), this may be re- lated to fact that low birth weight and premature labor mostly occur in combination. The majority of investiga- tors have indicated that the risk of developing HAI in- creased with lower birth weight. Stoll et al., [3] reported infection rates of 50% for infants weighting below 750 g, 33% for those between 751 and 1000 g, 21% for those between 1001 and 1250 g and 10% for those between 1251 and 1500 g [3]. During the study period, the most common pathogen incriminated for health care-associ- ated infection was klebseilla spp (128 isolates) followed by Enterobacter spp species, E coli and Acinetobacter spp (79, 78 and 72 isolates respectively), which means that Gram negative bacilli were the major causative pa- thogen in our NICU. The same findings were reported by Yilmaz et al., [25] where Klebsiella spp. And E. coli, to- gether, were responsible for 67% of HAI occurred in NICU [25]. Many investigators concur with our study in reporting that Gram-negative rods as the most common etiological factors [26]. Whereas, Gaynes et al., [27] and Stoll et al., [3], differ as they found that co-agulase-nega- tive staphylococci were the most common pathogen, pre- senting in 51% and 55% of cases, respectively [3,27]. The similar observation had Yelda et al., [20], they found that Gram-positive cocci account for 55.4% of HAI, and the most common organisms were Staphylococci [20]. Most of these isolates showed multiple antibiotics re- sistance. Results showed that approximately one-third of Klebsiella species (42/128) and E. coli (26/78) were ESBL producers .These results are in agreement with Di- nesh et al., (2011) who described a widespread problem of ESBL-producing multidrug-resistant strains of Kleb- siella and E. coli in hospital [28]. Also Amita et al., (2003) reported that more than 78% of Gram-negative isolates were positive in the screening test for ESBL pro- duction in blood borne neonatal infections [29]. The mortality rate was relatively high in the present study (27%); since all fatality cases were associated with Gram-negative pathogens. Gram-negative HAI often pre- sents with a more rapid clinical deterioration and is com- monly associated with shock and coagulation problems. According to Makhoul et al., [30] mortality after Gram- negative sepsis (26.2%) and Candida sepsis (27.6%) is similar and significantly higher than with Gram-positive sepsis (8.7%) [30]. Although other authors show that mor- tality caused by Gram positive pathogens is lower, about 2.83% to 6.98% [31]. However, organisms like co-agu- lase-negative Staphylococci may be underestimated be- cause many cultures that grow Gram-positive bacteria re- present skin contaminants rather than true blood stream infections. Open Access AID  Healthcare Associated Infection in the Neonatal Intensive Care Unit of King Abdl Aziz Specialist Hospital, Taif, KSA 304 5. Conclusion The overall HAI rate in our NICU over years 2006 - 2012 was relatively high although declining in the recent years due to application of strict infection control meas- ures, and the most prevalent organism was klebseilla spp, followed by other gram negative bacilli which commonly associated with shock and coagulation problems. There- fore, these organisms are blamed for relatively high mor- tality rate. 6. Acknowledgements I would like to express my sincere thanks and apprecia- tion to the microbiology laboratory members in King Ab- del Aziz Specialized Hospital (KAASH) for their support to complete of this research. REFERENCES [1] E. B. Daynia, N. Trusha, S. Charlotte and A. C. Peter, “Bacterial Bloodstream Infections in Neonates in a De- veloping Country,” ISRN Pediatrics, 2012, pp. 508-512. [2] N. Zafar, C. M. Wallace, P. Kieffer and P. Schroeder, “Improving Survival of Vulnerable Infant Increases Neo- natal. Intensive Care Unit Nosocomial Infection Rate,” Archives of Pediatrics & Adolescent Medicine, Vol. 155, No. 10, 2001, p. 1098. http://dx.doi.org/10.1001/archpedi.155.10.1098 [3] B. J. Stoll, N. Hansen, A. Fanaroff, L. Wright, W. Carlo and E. Dnovan, “Late-Onset Sepsis in Very Low Birth Weight Neonates: The Experience of the NICHD Neona- tal Research Network,” Pediatric NLM MEDLINE, Vol. 110, No. 2, 2002, pp. 285-286. http://dx.doi.org/10.1542/peds.110.2.285 [4] E. Hotoura, V. Giapros, A. Kostoula, P. Spirou and S. Andronikou, “Tracking Changes of Lymphocyte Subsets and Pre-Inflammatory Mediators in Full-Term Neonates with Suspected or Documented Infection,” Scandinavian Journal of Immunity, Vol. 73, No. 3, 2011, pp. 250-255. http://dx.doi.org/10.1111/j.1365-3083.2010.02499.x [5] S. K. Iwona, J. Aldona and K. Andrzej, “Healthcare-As- sociated Infections in a Neonatal Intensive Care Unit,” Archives of Medical Science, Vol. 8, No. 5, 2012, pp. 854-858. [6] W. H. Sheng, W. C. Chie, Y. C. Chen, C. C. Hung, J. T. Wang and S. C. Chang, “Impact of Nosocomial Infections on Medical Costs, Hospital Stay, and Outcome in Hospi- talized Patients,” Journal of the Formosan Medical Asso- ciation, Vol. 104, No. 5, 2005, pp. 318-326. [7] J. S. Yogaraj and A. M. Elward, “Risk Factors and Out- come of Nosocomial Bloodstream Infection in Neonatal ICU. Washington University, School of Medicine, USA,” Pediatrics, Vol. 110, No. 3, 2000, pp. 481-485. http://dx.doi.org/10.1542/peds.110.3.481 [8] A. Jaiswal, S. Murki, P. Gaddam and A. Reddy, “Early Neonatal Morbidities in Late Preterm Infants,” Indian Pe- diatrics, Vol. 48, No. 8, 2011, pp. 607-611. http://dx.doi.org/10.1007/s13312-011-0105-y [9] V. G. Hemming, J. C. Overall and M. R. Britt, “Nosoco- mial Infection in a Newborn Intensive Care Unit,” Infec- tion Control and Hospital Epidemiology, Vol. 21, No. 2, 2000, pp. 80-87. [10] A. P. Richard and M. R. Tara, “Biomarkers for Late-On- set Neonatal Sepsis,” Genome Medicine, Vol. 2, No. 9, 2010, 2010, pp. 58-60. http://dx.doi.org/10.1186/gm179 [11] T. B. Hyde, T. M. Hilger, A. Reingold, M. M. Farley, K. L. O’Brien and A. Schuchat, “Trends in Incidence and Antimicrobial Resistance of Early-Onset Sepsis: Popula- tion-Based Surveillance in San Francisco and Atlanta,” Pediatrics, Vol. 110, No. 4, 2002, pp. 690-695. http://dx.doi.org/10.1542/peds.110.4.690 [12] J. N. Baptiste, K. D. Benjamin, M. C. Wolkowiez, V. G. Fowler, M. Laughon and P. B. Smith, “Coagulase-Nega- tive Staphylococcal Infections in the Neonatal Intensive Care Unit,” Infection Control and Hospital Epidemiology, Vol. 32, No. 7, 2012, pp. 679-686. http://dx.doi.org/10.1086/660361 [13] T. Horan, M. Andrus and A. Dudeck, “Surveillance Defi- nition of Health Care Associated Infection and Criteria for Specific Types of Infections in the Acute Care Set- ting,” American Journal of Infection Control, Vol. 36, 2008, pp. 309-332. | http://dx.doi.org/10.1016/j.ajic.2008.03.002 [14] H. Vishal, S. Marcel, H. Wil, O. Alewijn, G. Ronald, W. Peter and F. K. René, “Coagulase-Negative Staphylococ- cal Skin Carriage among Neonatal Intensive Care Unit Personnel: From Population to Infection,” Journal of Cli- nical Microbiology, Vol. 48, No. 11, 2010, pp. 3876-3879. http://dx.doi.org/10.1128/JCM.00967-10 [15] E. K. Samuel, Q. Lawrence, S. Kenneth, B. Z. Juventus, I. B. Patricia and A. A. Anthony, “Susceptibility of Bacte- rial Etiological Agents to Commonly-Used Antimicrobial Agents in Children with Sepsis at the Tamale Teaching Hospital,” BMC Infectious Disease, Vol. 13, 2013, pp. 89-91. http://dx.doi.org/10.1186/1471-2334-13-89 [16] K. C. Iregbu, O. Y. Elegba and I. B. Babaniyi, “Bacterio- logical Profile of Neonatal Septicaemia in a Tertiary Hospital in Nigeria,” African Health Science, Vol. 6, No. 3, 2006, pp. 151-153. [17] M. L. Wilson, M. Mitchell and A. J. Morris, “Principles and Producers for Blood Culture; Approved Guidelines,” CLSI, 2007, pp. 7-10. [18] D. C. Kasper, I. Altiok, T. P. Mechtler, J. Böhm, J. Straub, Langgartner, et al., “Molecular Detection of Late-Onset Neonatal Sepsis in Premature Infants Using Small Blood Volumes: Proof-of-Concept,” Neonatology, Vol. 103, No. 4, 2013, pp. 268-273. http://dx.doi.org/10.1159/000346365 [19] S. K. Iwona and K. Piotr, “Healthcare-Associated Blood- stream Infection in Neonatal Intensive Care Unit,” Ar- chives of Perinatal Medicine, Vol. 15, No. 1, 2009, pp. 26-30. [20] A. L. Yelda, A. N. José, R. V. Juan, R. Q. Ulises, D. R. Ni- dia, P. B. Etna, et al., “Risk Factors and Prognosis for Ne- onatal Sepsis in Southeastern Mexico: Analysis of a Four- Open Access AID 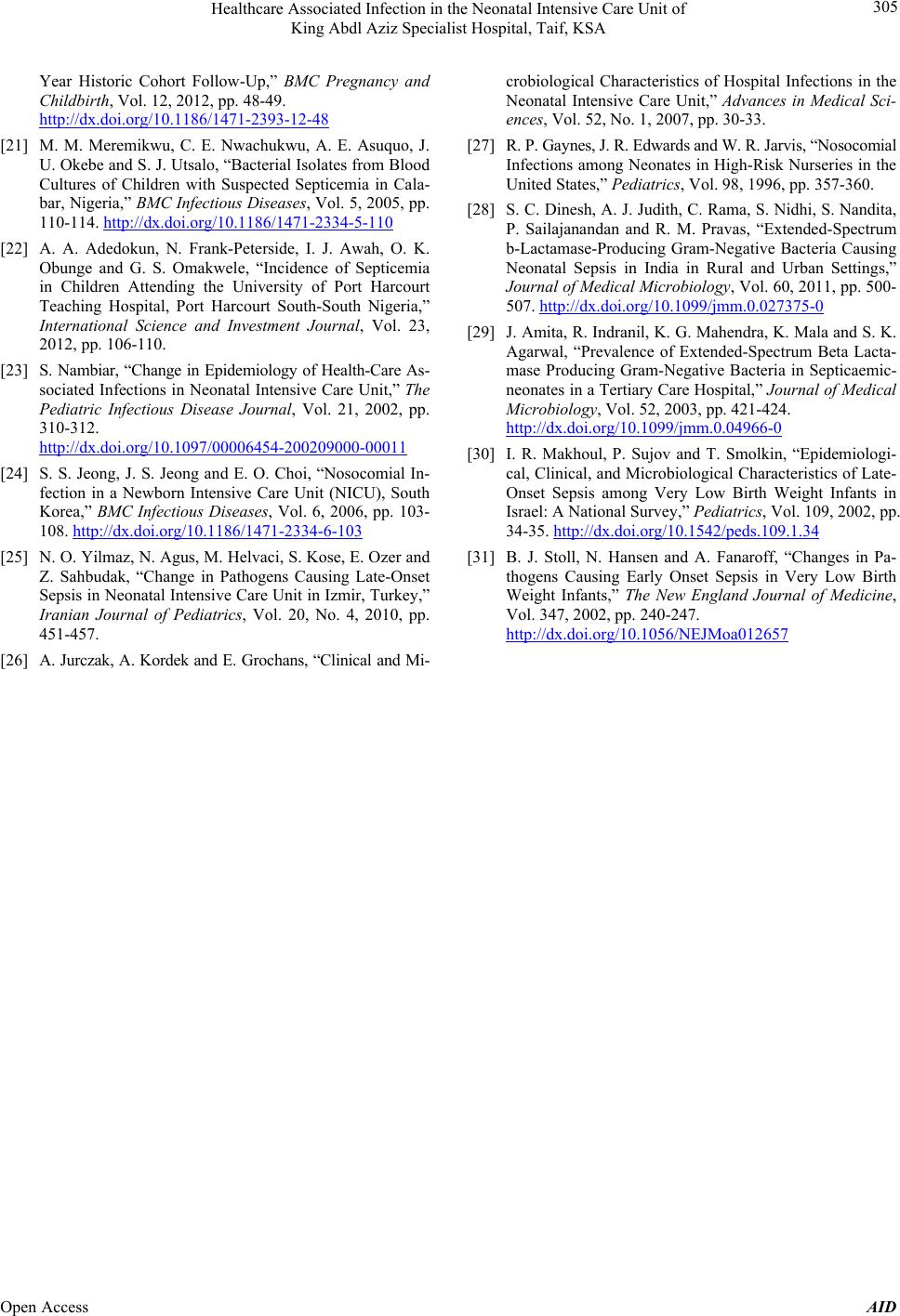 Healthcare Associated Infection in the Neonatal Intensive Care Unit of King Abdl Aziz Specialist Hospital, Taif, KSA Open Access AID 305 Year Historic Cohort Follow-Up,” BMC Pregnancy and Childbirth, Vol. 12, 2012, pp. 48-49. http://dx.doi.org/10.1186/1471-2393-12-48 [21] M. M. Meremikwu, C. E. Nwachukwu, A. E. Asuquo, J. U. Okebe and S. J. Utsalo, “Bacterial Isolates from Blood Cultures of Children with Suspected Septicemia in Cala- bar, Nigeria,” BMC Infectious Diseases, Vol. 5, 2005, pp. 110-114. http://dx.doi.org/10.1186/1471-2334-5-110 [22] A. A. Adedokun, N. Frank-Peterside, I. J. Awah, O. K. Obunge and G. S. Omakwele, “Incidence of Septicemia in Children Attending the University of Port Harcourt Teaching Hospital, Port Harcourt South-South Nigeria,” International Science and Investment Journal, Vol. 23, 2012, pp. 106-110. [23] S. Nambiar, “Change in Epidemiology of Health-Care As- sociated Infections in Neonatal Intensive Care Unit,” The Pediatric Infectious Disease Journal, Vol. 21, 2002, pp. 310-312. http://dx.doi.org/10.1097/00006454-200209000-00011 [24] S. S. Jeong, J. S. Jeong and E. O. Choi, “Nosocomial In- fection in a Newborn Intensive Care Unit (NICU), South Korea,” BMC Infectious Diseases, Vol. 6, 2006, pp. 103- 108. http://dx.doi.org/10.1186/1471-2334-6-103 [25] N. O. Yilmaz, N. Agus, M. Helvaci, S. Kose, E. Ozer and Z. Sahbudak, “Change in Pathogens Causing Late-Onset Sepsis in Neonatal Intensive Care Unit in Izmir, Turkey,” Iranian Journal of Pediatrics, Vol. 20, No. 4, 2010, pp. 451-457. [26] A. Jurczak, A. Kordek and E. Grochans, “Clinical and Mi- crobiological Characteristics of Hospital Infections in the Neonatal Intensive Care Unit,” Advances in Medical Sci- ences, Vol. 52, No. 1, 2007, pp. 30-33. [27] R. P. Gaynes, J. R. Edwards and W. R. Jarvis, “Nosocomial Infections among Neonates in High-Risk Nurseries in the United States,” Pe di at r ic s, Vol. 98, 1996, pp. 357-360. [28] S. C. Dinesh, A. J. Judith, C. Rama, S. Nidhi, S. Nandita, P. Sailajanandan and R. M. Pravas, “Extended-Spectrum b-Lactamase-Producing Gram-Negative Bacteria Causing Neonatal Sepsis in India in Rural and Urban Settings,” Journal of Medical Microbiology, Vol. 60, 2011, pp. 500- 507. http://dx.doi.org/10.1099/jmm.0.027375-0 [29] J. Amita, R. Indranil, K. G. Mahendra, K. Mala and S. K. Agarwal, “Prevalence of Extended-Spectrum Beta Lacta- mase Producing Gram-Negative Bacteria in Septicaemic- neonates in a Tertiary Care Hospital,” Journal of Medical Microbiology, Vol. 52, 2003, pp. 421-424. http://dx.doi.org/10.1099/jmm.0.04966-0 [30] I. R. Makhoul, P. Sujov and T. Smolkin, “Epidemiologi- cal, Clinical, and Microbiological Characteristics of Late- Onset Sepsis among Very Low Birth Weight Infants in Israel: A National Survey,” Pediatrics, Vol. 109, 2002, pp. 34-35. http://dx.doi.org/10.1542/peds.109.1.34 [31] B. J. Stoll, N. Hansen and A. Fanaroff, “Changes in Pa- thogens Causing Early Onset Sepsis in Very Low Birth Weight Infants,” The New England Journal of Medicine, Vol. 347, 2002, pp. 240-247. http://dx.doi.org/10.1056/NEJMoa012657
|