K. Akkarachinorate et al. / Case Reports in Clinical Medicine 2 (2013) 530-534
532
spp. in humans, which are known to cause sparganosis of
subcutaneous and visceral larva migrans [8]. Spirometra
adult worms inhabit the small intestine of dogs, cats and
wild carnivores, but rarely humans (spirometrosis). Co-
pepods (freshwater crustaceans) are the first intermediate
host for development of procercoid; various kinds of
vertebrates (amphibians, reptiles, birds and mammals)
then serve as the second intermediate host for develop-
ment of plerocercoid, to complete the life cycle [9]. Spo-
radic cases of sparganosis in humans have been reported,
mainly because of their scarcity but also because of the
difficulties around identification; there were only 52
cases of human sparganosis reported in Thailand be-
tween 1943 and 2010 [10]. Although sparganosis is gen-
erally thought to be distributed all over the world, Spi-
rometra spp. seem to be responsible for the larval plero-
cercoid stage and in humans rarely develop to adulthood;
it appears parasitic in muscles or body cavities. However,
ocular and cerebral involvements have been reported in
relation to sparganosis lesions found in Thai patients
particularly cerebral sparganosis accompanied by brain
abscess, seizures, hemiparesis has poor prognosis [10].
The larval plerocercoid can mostly be seen as a white,
string-like creature in the muscles or body cavities of
birds (chickens, ducks), reptiles (snakes), amphibians
(frogs), and small rodents, which are considered to be
important sources of infection. In addition, these hosts
and humans can also be infected by drinking contami-
nated water with cyclops-carrying procercoids, consum-
ing inadequately cooked meat containing the second-
intermediate or paratenic host carrying plerocercoids,
and also suffer penetration of cutaneous tissues from
poultices made of the flesh of frogs or snakes as dress-
ings for open wounds and eye sores [9,11,12]. Lesions
and clinical symptoms of sparganosis have much in
common with those of gnathostomiasis spinigerum; the
subcutaneous migrans is usually found as a migrating
nodule, varying in size, with occasional slow migration.
Gnathostomiasis is an important zoonosis with wide
distribution from tropical to temperate zones; it can be
fatal to humans if vital organs are affected [3]. The dis-
ease is widespread across Ecuador and Mexico in Latin
America [13,14], and Laos, Vietnam and Thailand in
Southeast Asia [2,15]. Gnathostoma spinigerum is par-
ticularly prevalent, yet remains the only etiologic agent
of human infection in Thailand so far [16]. Adult worms
are generally 2 - 3 cm long, with spines covering the
cephalic bulb to the posterior end, and inhabit tumors of
the gastrointestinal wall in fish-eating mammals. Com-
mon intermediate hosts are cyclops and freshwater fish
(eels, catfish, snake-head fish), reptiles (snakes) and
amphibians (frogs), which develop by hatching from
eggs into infective advanced third-stage larvae, which
themselves sometimes may be transferred to paratenic
hosts such as chickens, ducks, or pigs. Humans mostly
get infected accidentally by eating the infected flesh of
intermediate and paratenic hosts, in whom worms do not
develop into the adult stage. There are two other routes
of infection, as well, via skin penetration and prenatal
infection [2]. The most common manifestation is inter-
mittent migratory circumscribed swelling, with associ-
ated redness, pain and itching in the subcutaneous tissues;
this tends to subside and reappear elsewhere near the
original site. In rare cases, the pa tient may suffer seizures,
paralysis, unconsciousness, or even death due to severe
damage of the CNS; invasion of the eye can also result in
visual impairment [17]. Meanwhile, immature worms
have been found using excisional biopsy methods in
some patients, as migratory swelling tracks have been
left behind after the worms’ movement. Although worm
removal is a good method of treating gnathostomiasis, it
remains impractical as it often fails to remove all of the
etiologic worms present. Therefore, indirect investigation
in the laboratory is performed to g ive a tentative diagno-
sis of gnathostomiasis. One method is to use specific
monoclonal antibodies to detect circulating antigens to
the Gnathostoma worm; another is to use Western blot to
detect specific antibodies. However, such tests are not
available in remote areas of Thailand. Indeed, tests like
these are most frequently carried out in university ho spi-
tals, such as the Hospital for Tropical Diseases, Mahidol
University. About 1000 suspected cases are diagnosed
clinically each year after being sent for confirmatory
tests of gnathostomiasis, according to the annual report
of the Faculty of Tropical Medicine [18]. Clinicians
might decide to start treatment with albendazole (800 mg)
for 21 days [19], and observe clinical symptoms with a
follow-up drop in Gnathostoma antibody titer. It is chal-
lenging to perform an excisional biopsy at the swelling
area, as worms can always escape from the swollen mi-
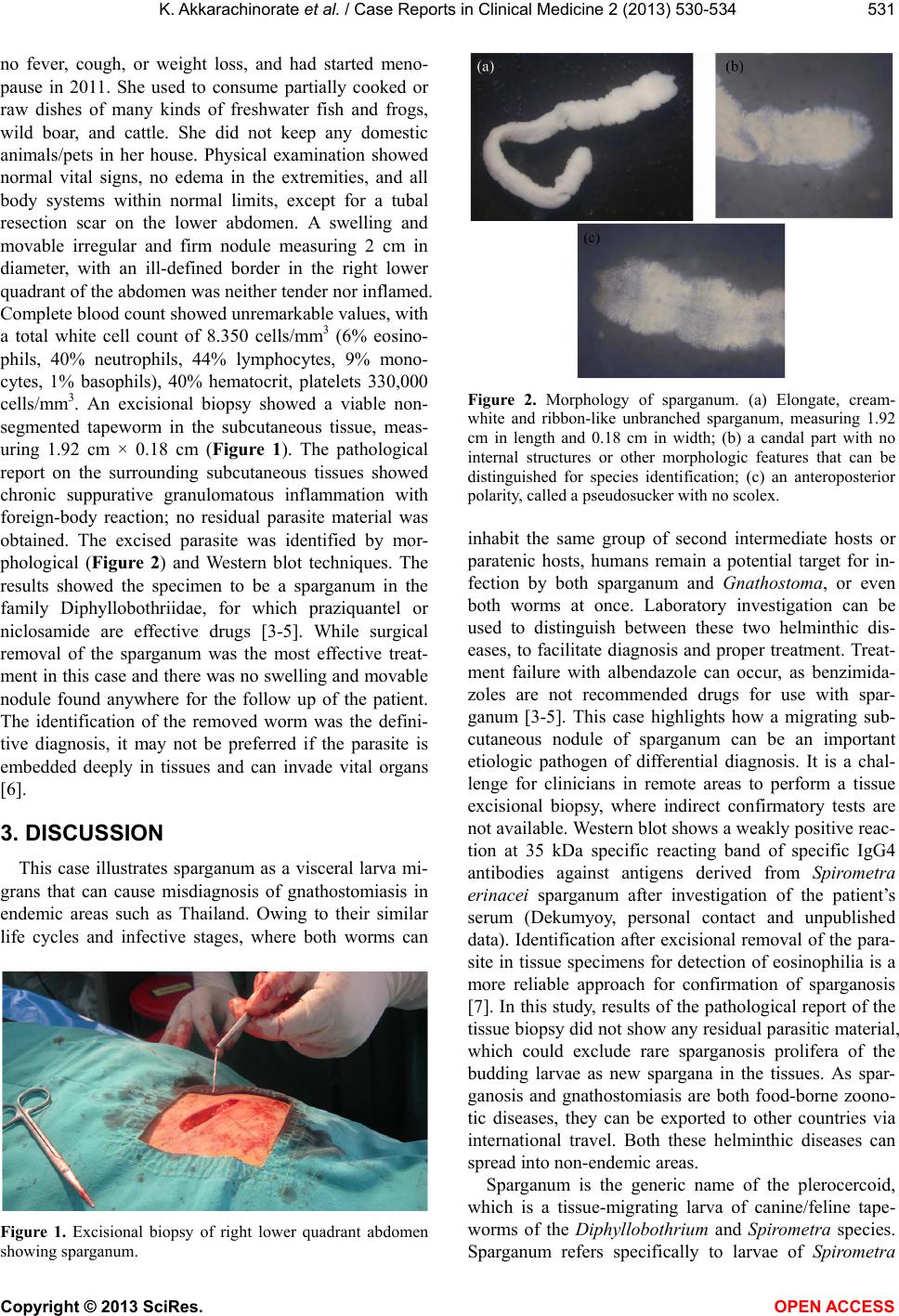
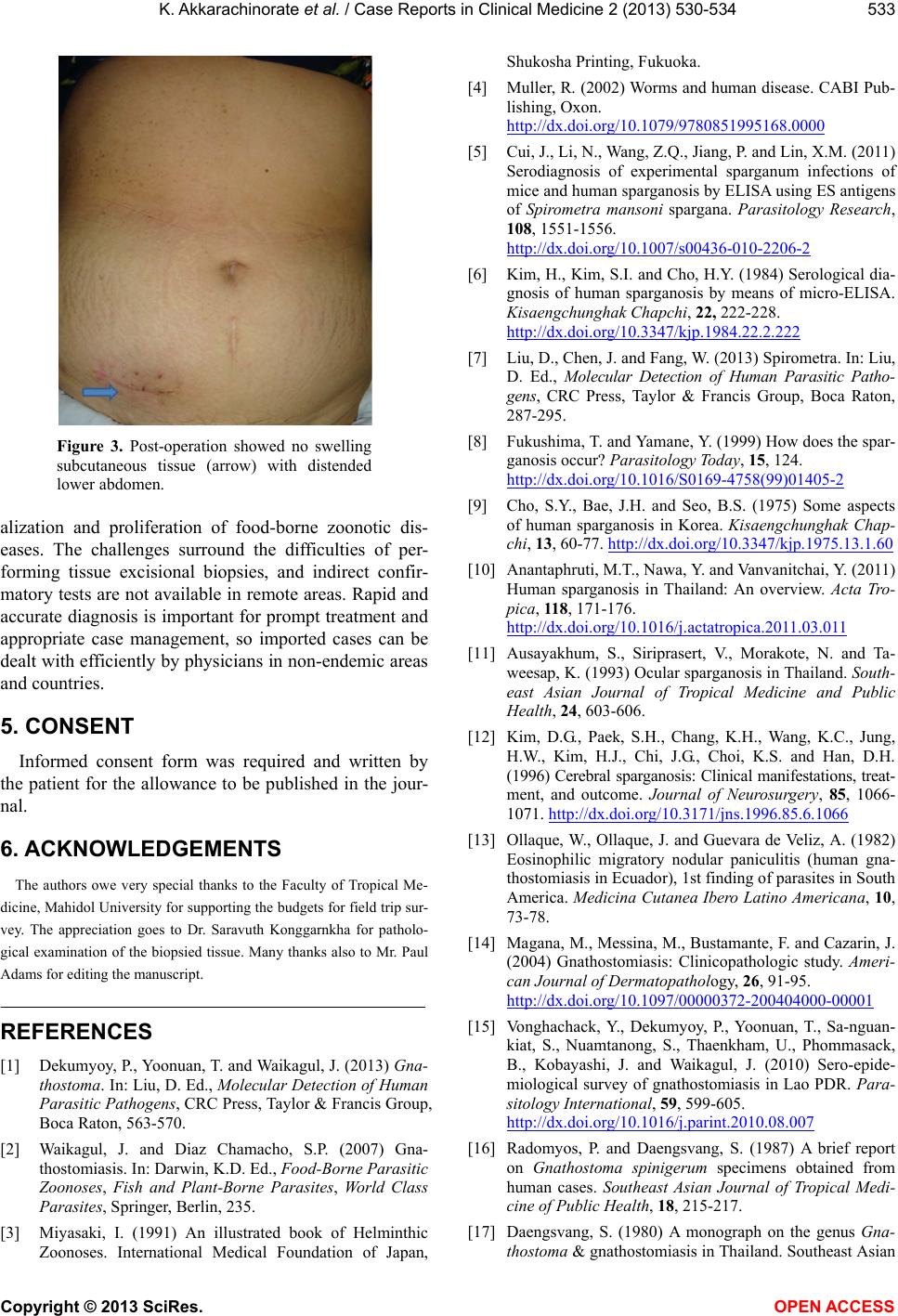
gration tracks. For our patient, who had been residing in
rural areas of Ban Luang District, Nan Province, Thai-
land, an excisional biopsy was attempted, and was suc-
cessful in removing the invading sparganum (Figure 3).
Recently, an alternative treatment with praziquantel (75
mg/kg/day), given in three consecutive doses, has been
attempted and the result was successful for visceral spar-
ganosis [5].
4. CONCLUSION
The sparganum can be an important etiologic pathogen
of differential diagnosis in migrating subcutaneous nod-
ules in endemic areas like Thailand. Clinical manifesta-
tions of gnathostomiasis and sparganosis are alike, in
terms of the migration of the immature worm, known as
subcutaneous larva migrans. This remains a cause of
migratory swelling in patients, which is the common
symptoms presented, and is the result of increased glob-
Copyright © 2013 SciRes. OPEN ACCESS