 World Journal of Cardiovascular Diseases, 2013, 3, 523-528 WJCD http://dx.doi.org/10.4236/wjcd.2013.39083 Published Online December 2013 (http://www.scirp.org/journal/wjcd/) Hypertension and intracerebral hemorrhage in Brazzaville* Thierry Raoul Gombet1,2#, Paul Macaire Ossou-Nguiet1,3, Thibaut Naibe Gankama4, Bertrand Fikahem Ellenga-Mbolla1,4, Gilbert Fabrice Otiobanda5, Karen Obondzo-Aloba3, Benjamin Longo-Mbenza6 1Department of Medicine, Faculty of Health Sciences of Brazzaville, Brazzaville, Congo 2Service of Emergency University Hospital of Brazzaville, Brazzaville, Congo 3Service of Neurology University Hospital of Brazzaville, Brazzaville, Congo 4Service of Cardiology University Hospital of Brazzaville, Brazzaville, Congo 5Service of Reanimation University Hospital of Brazzaville, Brazzaville, Congo 6Faculty of Health Sciences, Walter Sisulu University, Mthatha, South Africa Email: #raoulgombet@yahoo.fr Received 25 October 2013; revised 26 November 2013; accepted 3 December 2013 Copyright © 2013 Thierry Raoul Gombet et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In accordance of the Creative Commons Attribution License all Copyrights © 2013 are reserved for SCIRP and the owner of the intellectual property Thierry Raoul Gombet et al. All Copyright © 2013 are guarded by law and by SCIRP as a guardian. ABSTRACT Hypertension is not only an important risk factor, but also an important cause of spontaneous intracerebral hemorrhage. Its high prevalence in Africa reflects a high incidence of cerebral hemorrhage ranging from 30% to 60% against 10% to 20% in industrialized countries. The aim of our study was to determine the role of hypertension before the onset of intracerebral hemorrhage and its variations during the first three months. This was a longitudinal study conducted at the University Hospital of Brazzaville from 1st Janu- ary to 31st August 2012 with all patients admitted for intracerebral hemorrhage. Patients with subarach- noid or pure intraventricular hemorrhage were ex- cluded. The study variables were: history of hyper- tension, knowledge of its history, treatment, blood pressure on admission and during the first 3 months and the relationship between blood pressure and evolution. Statistical analysis was performed using the software SPSSS 16.1. The significance level was set at p < 0.05. During the study 261 patients were hospitalized for stroke, of which 82 (31.42%) were for intracerebral hemorrhage. The mean age was 55 ± 11 years and sex ratio of 2 men:1 woman. Hypertension was found in 80.5% of cases, of which 65.2% had known hypertension, but 82.6% had discontinued treatment. The mean systolic blood pressure was 194 ± 41 mm Hg and dia stolic 104 ± 20 mm Hg. The loca- tion was deep in 85.71%. The normalization of blood pressure was obtained from the second week. After adjusting for confounders using logistic analysis, only uncontrolled hypertension was associated significantly and independently associated with a higher mortality rate (p = 0.042). Keywords: Hypertension; Cerebral Hemorrhage; Brazzaville 1. INTRODUCTION The hemorrhagic stroke or intra cerebral hematoma (ICH) is the extravasation of blood into the brain parenchyma. Its incidence is 9 - 15 cases per 100.000 persons [1]. There are racial variations of hypertension prevalence which is higher among blacks and Asians than the rest of the world [2,3]. It represents 10% to 30% of stroke [4,5]. ICH is the most severe and the most deadly subtype. Chronic hypertension is not only the first risk factor, but also the primary cause of ICH in 60% of cases [6,7]. Ar- teriosclerosis and micro-Charcot-Bouchard aneurysms which may rupture at deep penetrating arterioles explain the hematoma [8,9]. A high blood pressure is regularly observed in the acute phase of ICH [10], most often as- sociated with an increase in the volume of hematoma, or a poor prognosis [6]. Although studies have been con- ducted on the management of blood pressure in ICH [11, 12], however, in sub-Saharan Africa, the prevalence of hypertension is high with a lower prevalence of stroke in general populations [13]. In Brazzaville (Congo), 32.5% of the population are hy- pertensive [14]. Furthermore, stroke is a frequent reason *Conflict of interest: The authors declare no conflict of interest #Corresponding author. OPEN ACCESS  T. R. Gombet et al. / World Journal of Cardiovascular Diseases 3 (2013) 523-528 524 for hospitalization, and represents the first hypertensive emergency in Brazzaville University Hospital [15]. The aim of our study was to assess the role of hyper- tension before the onset of ICH, and its variations during the first three months, as well as its impact on prognosis. 2. METHODS This is a longitudinal study conducted at the University Hospital of Brazzaville, services of Neurology, Emer- gency and Intensive Care Unit from 1st January to 31st August 2012 for a period of 8 months. The study popula- tion consisted of patients admitted for ICH in these ser- vices. We included all patients hospitalized for hemor- rhagic stroke confirmed by CT scan without contrast injection, regardless of age and sex. Informed consent was obtained either from the patient when he was not conscious and aphasic, either from a close family mem- ber when the patient was unconscious or in case of se- vere aphasia. We excluded all patients hospitalized for suspicion of stroke not confirmed by brain CT-scan, pa- tients with normal scan or signs of ischemic stroke, iso- late subarachnoid hemorrhage, intraventricular hemor- rhage, hemorrhagic infarction, head trauma, brain tumor- induced hemorrhage, or patients in whom informed con- sent was not obtained. The diagnosis of hemorrhagic stroke was confirmed by the presence of an intraparen- chymal hyperdensity with or without spontaneous ven- tricular break. The study variables were: age, sex, vascu- lar risk factors such as the history of hypertension de- fined as systolic blood pressure(SBP or PAS in french) ≥ 140 mmHg and/or diastolic blood pressure (DBP or PAD in French) ≥90 mmHg or the existence of antihyperten- sive treatment in. Knowledge of hypertension, its dura- tion, the time between ICH onset and the time of hospi- talization, adherence, control, daily monitoring, the loca- tion and the site of the hematoma, the severity of hyper- tension at admission, the initial severity stroke by the NIHSS score, the progression of the disease and out- comes(death or survivorship) of patient. The evolution was evaluated on the third day (D3 or J3 in French) on the seventh day (D7 or J7 in French), the fourteenth day (D14 or J14 in French), one month (M1), two months (M2) and three months (M3 or J90 in French). 3. STATISTICAL ANALYSIS The data collected were entered in Excel, and then ana- lyzed using the SPSSS version 16.1 on Windows. The qualitative variables were expressed as frequency (n) or proportions (%) and quantitative variables as mean ± standard deviation(SD). The chi-square test was used to compare proportions, while Student-t test was used to compare means. Statistical significance was set for the probability p ≤ 0.05. 4. RESULTS Of 689 patients in these services, 261(37.88%) were ad- mitted for stroke, among them 86 (32.95%) cases of ICH with 82 cases of intra-parenchymal hemorrhage (31.42%) and 4 cases (1.53%) of subarachnoid hemorrhage. A total of 82 cases of ICH, there were 51 (63.4%) men and 31 (36.6%) women with a sex ratio of 2 men: 1 woman. The mean age of patients was 55 ± 11 years (range 26 to 83 years). Table 1 shows the frequency of various risk factors. In terms of frequency of risk factors, hypertension was the first with 80.5 % of patients. Twenty-three hyperten- sive patients were adherent to hyp 19 (82.6%) had dis- continued treatment before hospitalization. Hypertension was found in 80.5% of cases whose 65.2% had known hypertension but 82.6% had discontinued treatment. Only 4 (17.4%) had not interrupted the assessment of the longitudinal follow-up. On admission, the mean systolic blood pressure (SBP) was 194.51 ± 41.31 mmHg, with a range from 100 to 270mmHg. Diastolic blood pressure (DBP) averaged 104.51 ± 20.44 mmHg, with a range from 70 to 170 mmHg. Figure 1 shows the levels of blood pressure on admission. In terms of initial severity, the NIHSS score at admis- sion average was 14.9 ± 7.3, with a range from 2 to 30. The electrocardiogram had revealed left ventricular hypertrophy (LVH) in 42 (63.6%) on 66 hypertensive. The average time for completion of the CT scan was 2.4 ± 2 days, with ranging from 1 to 14 days. Ventricular break of hemorrhage was noted in 24 (29.4%) patients. The hematoma was supratentoriel in 92.7% and 6.1% in infratentorial. The average volume of the hematoma was 24 ± 17 ml. The deep site was the most frequent (55%) followed by lobar site in 29% (Figure 2). The management of blood pressure involved the ad- ministration of intravenous nicardipin for all patients with blood pressure ≥ 160/110 mmHg, and all known hypertensive patient were treated by combination of Enalapril and Hydrochlorothiazide. Figure 3 depicts the changes of SBP and DBP across the time of the monitoring which showed a constant nor- malization of blood pressure from the second week to the end of the follow-up (3 months). The incident mortality rate was 37.8% (n = 31/82 pa- tients). After adjusting for age, sex, history of hyperten- sion, and initial severity, multivariate analysis identified only uncontrolled hypertension was associated signifi- cantly and independently associatedwith higher mortality rate (p = 0.042) (Table 2). 5. DISCUSSION We conducted a prospective study, including all patients Copyright © 2013 SciRes. OPEN ACCESS 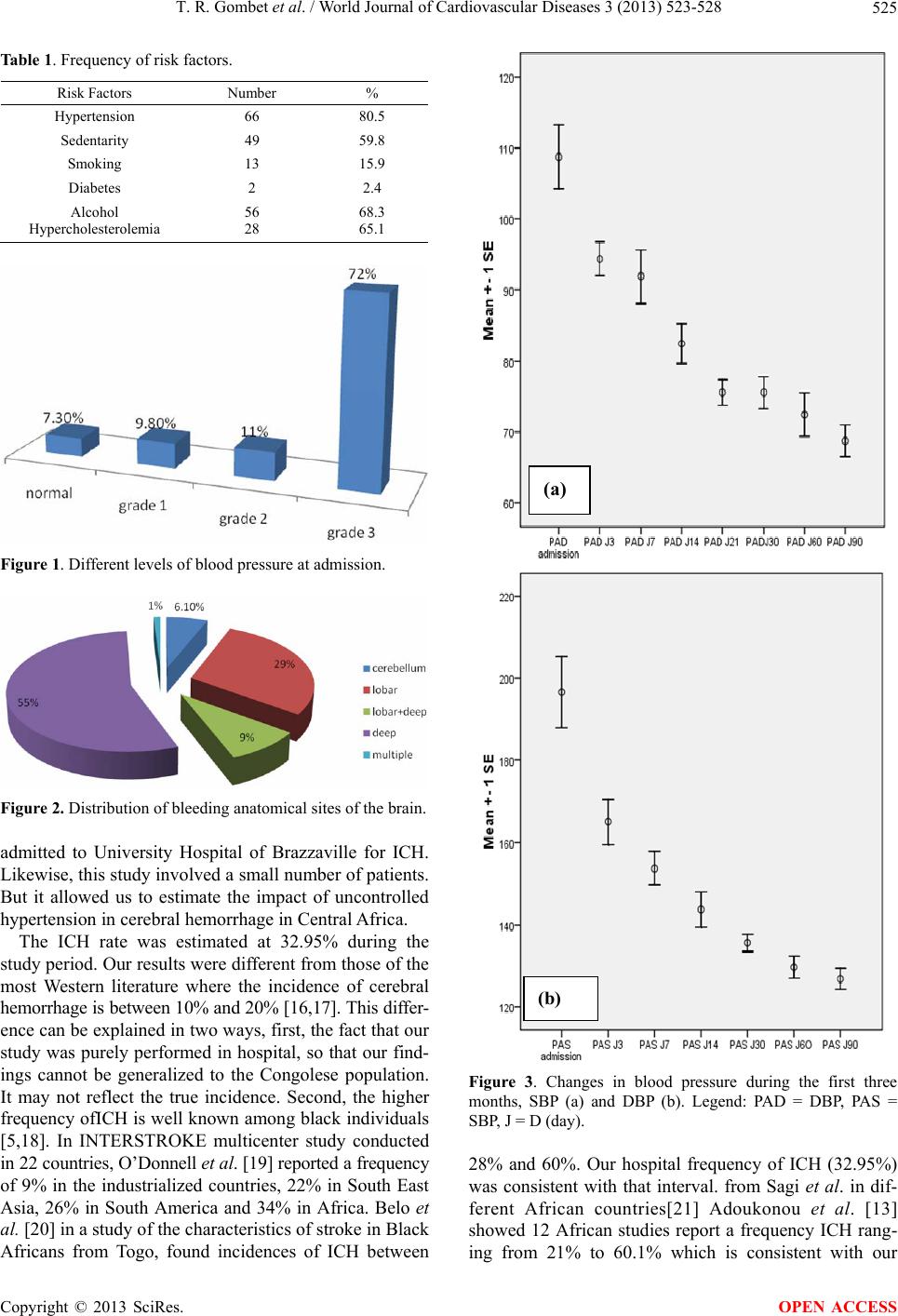 T. R. Gombet et al. / World Journal of Cardiovascular Diseases 3 (2013) 523-528 525 Table 1. Frequency of risk factors. Risk Factors Number % Hypertension 66 80.5 Sedentarity 49 59.8 Smoking 13 15.9 Diabetes 2 2.4 Alcohol Hypercholesterolemia 56 28 68.3 65.1 Figure 1. Different levels of blood pressure at admission. Figure 2. Distribution of bleeding anatomical sites of the brain. admitted to University Hospital of Brazzaville for ICH. Likewise, this study involved a small number of patients. But it allowed us to estimate the impact of uncontrolled hypertension in cerebral hemorrhage in Central Africa. The ICH rate was estimated at 32.95% during the study period. Our results were different from those of the most Western literature where the incidence of cerebral hemorrhage is between 10% and 20% [16,17]. This differ- ence can be explained in two ways, first, the fact that our study was purely performed in hospital, so that our find- ings cannot be generalized to the Congolese population. It may not reflect the true incidence. Second, the higher frequency ofICH is well known among black individuals [5,18]. In INTERSTROKE multicenter study conducted in 22 countries, O’Donnell et al. [19] reported a frequency of 9% in the industrialized countries, 22% in South East Asia, 26% in South America and 34% in Africa. Belo et al. [20] in a study of the characteristics of stroke in Black Africans from Togo, found incidences of ICH between (a) (b) Figure 3. Changes in blood pressure during the first three months, SBP (a) and DBP (b). Legend: PAD = DBP, PAS = SBP, J = D (day). 28% and 60%. Our hospital frequency of ICH (32.95%) was consistent with that interval. from Sagi et al. in dif- ferent African countries[21] Adoukonou et al. [13] showed 12 African studies report a frequency ICH rang- ing from 21% to 60.1% which is consistent with our Copyright © 2013 SciRes. OPEN ACCESS 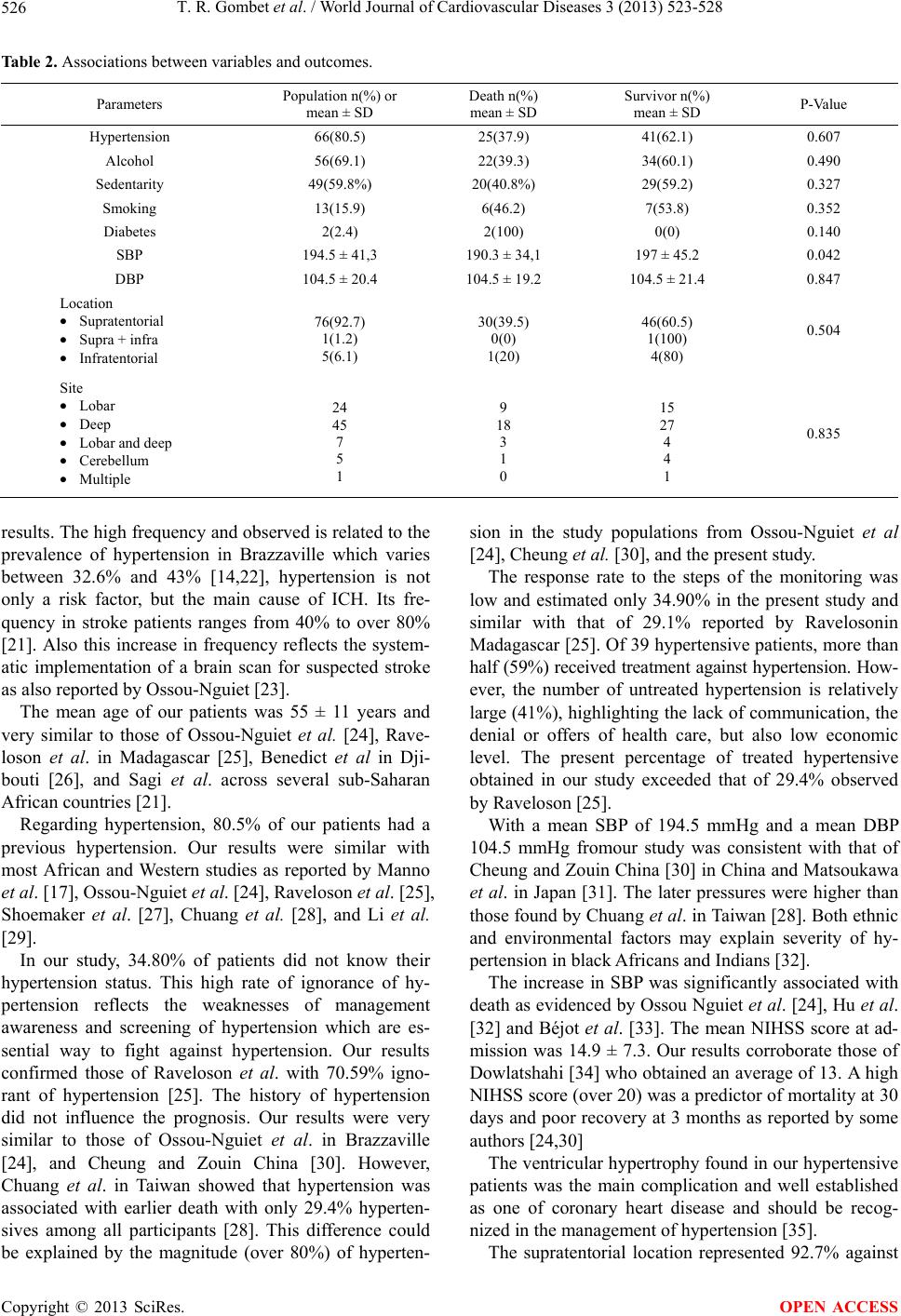 T. R. Gombet et al. / World Journal of Cardiovascular Diseases 3 (2013) 523-528 Copyright © 2013 SciRes. 526 OPEN ACCESS Table 2. Associations between variables and outcomes. Parameters Population n(%) or mean ± SD Death n(%) mean ± SD Survivor n(%) mean ± SD P-Value Hypertension 66(80.5) 25(37.9) 41(62.1) 0.607 Alcohol 56(69.1) 22(39.3) 34(60.1) 0.490 Sedentarity 49(59.8%) 20(40.8%) 29(59.2) 0.327 Smoking 13(15.9) 6(46.2) 7(53.8) 0.352 Diabetes 2(2.4) 2(100) 0(0) 0.140 SBP 194.5 ± 41,3 190.3 ± 34,1 197 ± 45.2 0.042 DBP 104.5 ± 20.4 104.5 ± 19.2 104.5 ± 21.4 0.847 Location • Supratentorial • Supra + infra • Infratentorial 76(92.7) 1(1.2) 5(6.1) 30(39.5) 0(0) 1(20) 46(60.5) 1(100) 4(80) 0.504 Site • Lobar • Deep • Lobar and deep • Cerebellum • Multiple 24 45 7 5 1 9 18 3 1 0 15 27 4 4 1 0.835 results. The high frequency and observed is related to the prevalence of hypertension in Brazzaville which varies between 32.6% and 43% [14,22], hypertension is not only a risk factor, but the main cause of ICH. Its fre- quency in stroke patients ranges from 40% to over 80% [21]. Also this increase in frequency reflects the system- atic implementation of a brain scan for suspected stroke as also reported by Ossou-Nguiet [23]. The mean age of our patients was 55 ± 11 years and very similar to those of Ossou-Nguiet et al. [24], Rave- loson et al. in Madagascar [25], Benedict et al in Dji- bouti [26], and Sagi et al. across several sub-Saharan African countries [21]. Regarding hypertension, 80.5% of our patients had a previous hypertension. Our results were similar with most African and Western studies as reported by Manno et al. [17], Ossou-Nguiet et al. [24], Raveloson et al. [25], Shoemaker et al. [27], Chuang et al. [28], and Li et al. [29]. In our study, 34.80% of patients did not know their hypertension status. This high rate of ignorance of hy- pertension reflects the weaknesses of management awareness and screening of hypertension which are es- sential way to fight against hypertension. Our results confirmed those of Raveloson et al. with 70.59% igno- rant of hypertension [25]. The history of hypertension did not influence the prognosis. Our results were very similar to those of Ossou-Nguiet et al. in Brazzaville [24], and Cheung and Zouin China [30]. However, Chuang et al. in Taiwan showed that hypertension was associated with earlier death with only 29.4% hyperten- sives among all participants [28]. This difference could be explained by the magnitude (over 80%) of hyperten- sion in the study populations from Ossou-Nguiet et al [24], Cheung et al. [30], and the present study. The response rate to the steps of the monitoring was low and estimated only 34.90% in the present study and similar with that of 29.1% reported by Ravelosonin Madagascar [25]. Of 39 hypertensive patients, more than half (59%) received treatment against hypertension. How- ever, the number of untreated hypertension is relatively large (41%), highlighting the lack of communication, the denial or offers of health care, but also low economic level. The present percentage of treated hypertensive obtained in our study exceeded that of 29.4% observed by Raveloson [25]. With a mean SBP of 194.5 mmHg and a mean DBP 104.5 mmHg fromour study was consistent with that of Cheung and Zouin China [30] in China and Matsoukawa et al. in Japan [31]. The later pressures were higher than those found by Chuang et al. in Taiwan [28]. Both ethnic and environmental factors may explain severity of hy- pertension in black Africans and Indians [32]. The increase in SBP was significantly associated with death as evidenced by Ossou Nguiet et al. [24], Hu et al. [32] and Béjot et al. [33]. The mean NIHSS score at ad- mission was 14.9 ± 7.3. Our results corroborate those of Dowlatshahi [34] who obtained an average of 13. A high NIHSS score (over 20) was a predictor of mortality at 30 days and poor recovery at 3 months as reported by some authors [24,30] The ventricular hypertrophy found in our hypertensive patients was the main complication and well established as one of coronary heart disease and should be recog- nized in the management of hypertension [35]. The supratentorial location represented 92.7% against 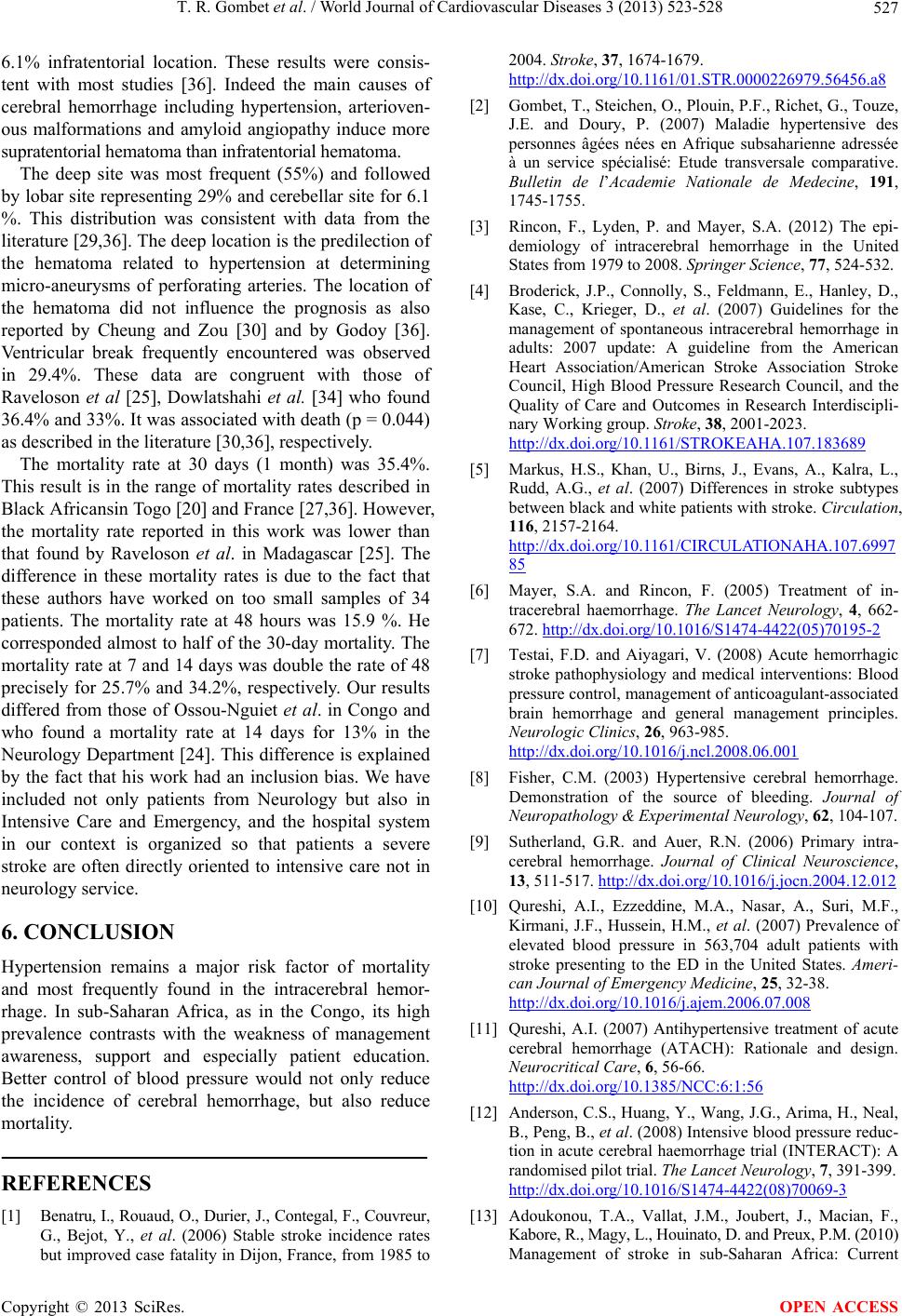 T. R. Gombet et al. / World Journal of Cardiovascular Diseases 3 (2013) 523-528 527 6.1% infratentorial location. These results were consis- tent with most studies [36]. Indeed the main causes of cerebral hemorrhage including hypertension, arterioven- ous malformations and amyloid angiopathy induce more supratentorial hematoma than infratentorial hematoma. The deep site was most frequent (55%) and followed by lobar site representing 29% and cerebellar site for 6.1 %. This distribution was consistent with data from the literature [29,36]. The deep location is the predilection of the hematoma related to hypertension at determining micro-aneurysms of perforating arteries. The location of the hematoma did not influence the prognosis as also reported by Cheung and Zou [30] and by Godoy [36]. Ventricular break frequently encountered was observed in 29.4%. These data are congruent with those of Raveloson et al [25], Dowlatshahi et al. [34] who found 36.4% and 33%. It was associated with death (p = 0.044) as described in the literature [30,36], respectively. The mortality rate at 30 days (1 month) was 35.4%. This result is in the range of mortality rates described in Black Africansin Togo [20] and France [27,36]. However, the mortality rate reported in this work was lower than that found by Raveloson et al. in Madagascar [25]. The difference in these mortality rates is due to the fact that these authors have worked on too small samples of 34 patients. The mortality rate at 48 hours was 15.9 %. He corresponded almost to half of the 30-day mortality. The mortality rate at 7 and 14 days was double the rate of 48 precisely for 25.7% and 34.2%, respectively. Our results differed from those of Ossou-Nguiet et al. in Congo and who found a mortality rate at 14 days for 13% in the Neurology Department [24]. This difference is explained by the fact that his work had an inclusion bias. We have included not only patients from Neurology but also in Intensive Care and Emergency, and the hospital system in our context is organized so that patients a severe stroke are often directly oriented to intensive care not in neurology service. 6. CONCLUSION Hypertension remains a major risk factor of mortality and most frequently found in the intracerebral hemor- rhage. In sub-Saharan Africa, as in the Congo, its high prevalence contrasts with the weakness of management awareness, support and especially patient education. Better control of blood pressure would not only reduce the incidence of cerebral hemorrhage, but also reduce mortality. REFERENCES [1] Benatru, I., Rouaud, O., Durier, J., Contegal, F., Couvreur, G., Bejot, Y., et al. (2006) Stable stroke incidence rates but improved case fatality in Dijon, France, from 1985 to 2004. Stroke, 37, 1674-1679. http://dx.doi.org/10.1161/01.STR.0000226979.56456.a8 [2] Gombet, T., Steichen, O., Plouin, P.F., Richet, G., Touze, J.E. and Doury, P. (2007) Maladie hypertensive des personnes âgées nées en Afrique subsaharienne adressée à un service spécialisé: Etude transversale comparative. Bulletin de l’Academie Nationale de Medecine, 191, 1745-1755. [3] Rincon, F., Lyden, P. and Mayer, S.A. (2012) The epi- demiology of intracerebral hemorrhage in the United States from 1979 to 2008. Springer Science, 77, 524-532. [4] Broderick, J.P., Connolly, S., Feldmann, E., Hanley, D., Kase, C., Krieger, D., et al. (2007) Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: A guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdiscipli- nary Working group. Stroke, 38, 2001-2023. http://dx.doi.org/10.1161/STROKEAHA.107.183689 [5] Markus, H.S., Khan, U., Birns, J., Evans, A., Kalra, L., Rudd, A.G., et al. (2007) Differences in stroke subtypes between black and white patients with stroke. Circulation, 116, 2157-2164. http://dx.doi.org/10.1161/CIRCULATIONAHA.107.6997 85 [6] Mayer, S.A. and Rincon, F. (2005) Treatment of in- tracerebral haemorrhage. The Lancet Neurology, 4, 662- 672. http://dx.doi.org/10.1016/S1474-4422(05)70195-2 [7] Testai, F.D. and Aiyagari, V. (2008) Acute hemorrhagic stroke pathophysiology and medical interventions: Blood pressure control, management of anticoagulant-associated brain hemorrhage and general management principles. Neurologic Clinics, 26, 963-985. http://dx.doi.org/10.1016/j.ncl.2008.06.001 [8] Fisher, C.M. (2003) Hypertensive cerebral hemorrhage. Demonstration of the source of bleeding. Journal of Neuropathology & Experimental Neurology, 62, 104-107. [9] Sutherland, G.R. and Auer, R.N. (2006) Primary intra- cerebral hemorrhage. Journal of Clinical Neuroscience, 13, 511-517. http://dx.doi.org/10.1016/j.jocn.2004.12.012 [10] Qureshi, A.I., Ezzeddine, M.A., Nasar, A., Suri, M.F., Kirmani, J.F., Hussein, H.M., et al. (2007) Prevalence of elevated blood pressure in 563,704 adult patients with stroke presenting to the ED in the United States. Ameri- can Journal of Emergency Medicine, 25, 32-38. http://dx.doi.org/10.1016/j.ajem.2006.07.008 [11] Qureshi, A.I. (2007) Antihypertensive treatment of acute cerebral hemorrhage (ATACH): Rationale and design. Neurocritical Care, 6, 56-66. http://dx.doi.org/10.1385/NCC:6:1:56 [12] Anderson, C.S., Huang, Y., Wang, J.G., Arima, H., Neal, B., Peng, B., et al. (2008) Intensive blood pressure reduc- tion in acute cerebral haemorrhage trial (INTERACT): A randomised pilot trial. The Lancet Neurology, 7, 391-399. http://dx.doi.org/10.1016/S1474-4422(08)70069-3 [13] Adoukonou, T.A., Vallat, J.M., Joubert, J., Macian, F., Kabore, R., Magy, L., Houinato, D. and Preux, P.M. (2010) Management of stroke in sub-Saharan Africa: Current Copyright © 2013 SciRes. OPEN ACCESS  T. R. Gombet et al. / World Journal of Cardiovascular Diseases 3 (2013) 523-528 Copyright © 2013 SciRes. 528 OPEN ACCESS issues. Revue Neurologique, 166, 882-893. http://dx.doi.org/10.1016/j.neurol.2010.06.004 [14] Kimbally-Kaky, G., Gombet, T., Bolanda, D., Voumbo, Y., Okili, B., Ellenga-Mbolla, B. et al. (2006) Prévalence de l’HTA à Brazzaville. Cardiologie Tropicale, 32, 43- 46. [15] Ellenga-Mbolla, B.F., Gombet, T.R., Mahoungou-Guimbi, K.C., Otiobanda, G.F., Ossou-Nguiet, P.M., Ikama, M.S., KimballyKaky, G. and Etitiele, F. (2011) Les urgences hypertensives au Centre Hospitalier et Universitaire de Brazzaville (Congo). Médecine Tropicale, 71, 97-98. [16] Elliott, J. and Smith, M. (2010) The acute management of intracerebral hemorrhage: A clinical review. Anesthesia & Analgesia, 110, 1419-1427. http://dx.doi.org/10.1213/ANE.0b013e3181d568c8 [17] Manno, E.M. (2012) Update on intracerebral hemorrhage. CONTINUUM: Lifelong Learning in Neurology, 18, 598- 610. http://dx.doi.org/10.1212/01.CON.0000415430.99394.3e [18] Lotufo, P.A., Goulart, A.C. and Bensenor, I.M. (2007) Race, gender and stroke subtypes mortality in Sao Paulo, Brazil. Arquivos de Neuro-Psiqui atria, 65, 752-757. [19] O’Donnell, M.J., Xavier, D., Liu, L., Zhang, H., Chin, S.L., Rao-Melacini, P., et al. (2010) (INTERSTROKE investigators). Risk factors for ischaemic and intracere- bral haemorrhagic stroke in 22 countries (the INTER- STROKE study): A case-control study. The Lancet, 376, 112-123. http://dx.doi.org/10.1016/S0140-6736(10)60834-3 [20] Belo, M., Balogou, A.A.K., Goeh-Akue, E., Sognigbe, N., Kumako, V., Djibril, M., et al. (2007) Particularitée des accidents vasculaires cérébraux au Togo et en Afrique Noire. Journal de la Recherche Scientifique de l’Univer- site de Lome, 9, 21-27. [21] Sagui, E. (2007) Les accidents vasculaires cérébraux en Afrique subsaharienne. Médecine Tropicale, 6, 596-600. [22] Lessive, P., Mughnetsyan, V. and Kessy, G.S. (2009) Etude épidémiologique lors d’une campagne de dépistage du diabète, de l’hypertension et de l’obésité androïde à Brazzaville. Medecine des Maladies Metab oliques, 3, 438- 441. [23] Ossou-Nguiet, P.M., Otiobanda, G.F., ObondzoAloba, K., Ellenga-Mbolla, B.F., Bandzouzi-Ndamba, B. and Ma- kosso, E. (2013) Contribution on epidemiology and man- agement of stroke in a central African country. Interna- tional Journal of Stroke, 8, E27. http://dx.doi.org/10.1111/ijs.12118 [24] Ossou-Nguiet, P.M., Otiobanda, G.F., Bandzouzi-Ndamba, B., Ellenga-Mbolla, B.F., Mahoungou-Guimbi, K.C., Gn- onlonfoun, D., et al. (2011) Devenir des patients ayant présenté une hémorragie cérébrale au CHUB de Braz- zaville. RAMUR Tome, 16, 37-43. [25] Raveloson, N.E., Zodali, N., Rakotoarivoni, S.T., Mbol- ambena, R.L. and Randriamiarana, J.M. (2011) Aspects épidémio-cliniques, évolutifs et tomodensitométriques des accidents vasculaires cérébraux hémorragiques. Re- vue d’Anesthésie-Réanimation et de Médecine d’Urgences, 3, 15-19. [26] Benoît, A., Raynaud, A., Coton, L., Petitjans, F., Hassan, A., Ilah, A., et al. (2009) Morbi-mortalité des accidents vasculaires cérébraux hémorragiques. Médecine Tropic- ale, 69, 41-44. [27] Cordonnier, C., Rutgers, M.P., Dumont, F., Pasquini, M., Le Jeune, J.P., Garrigue, D., et al. (2009) Intracerebral haemorrhages: Are there differences in baseline charac- teristics and intra-hospital mortality between hospital and population-based registred? Journal of Neurology, 256, 198-202. http://dx.doi.org/10.1007/s00415-009-0030-3 [28] Chuang, Y.C., Chen, Y.M., Peng, S.K. and Peng, S.Y. (2009) Risk stratification for predicting 30-day mortality of intracerebral hemorrhage. International Journal for Quality in Health Care, 21, 441-447. http://dx.doi.org/10.1093/intqhc/mzp041 [29] Li, Q., Qin, X.Y., Zhang, J.H. and Yang, J. (2011) Prog- nosis study of 324 cases with spontaneous intracerebral hemorrhage in Chongqing, China. Acta Neurochirurgica Supplementum, 111, 399-402. http://dx.doi.org/10.1007/978-3-7091-0693-8_68 [30] Cheung, R.T. and Zou, L.Y. (2003) Use of the original, modified or new intracerebral hemorrhage score to pre- dict mortality and morbidity after intracerebral hemor- rhage. Stroke, 34, 1717-1712. http://dx.doi.org/10.1161/01.STR.0000078657.22835.B9 [31] Matsukawa, H., Shinoda, M., Fujii, M., Takahashi, O., Yamamoto, D., Murakata, A., et al. (2012) Relationships among hematoma diameter, location categorized by vas- cular territory, and 1-year outcome in patients with cere- bellar hemorrhage. World Neurosurgery, 77, 507-511. http://dx.doi.org/10.1016/j.wneu.2011.05.018 [32] Hu, X., Zhang, J.H. and Qin, X. (2011) Risk factors of early death in patients with hypertensive intracerebral hemorrhage during hospitalisation. Acta Neurochirurgica Supplementum, 11, 387-391. http://dx.doi.org/10.1007/978-3-7091-0693-8_66 [33] Bejot, Y., Rouaud, O., Benatru, I., Froment, A., Couvreur, G., Cailler, M., et al. (2008) Les apports du registre dijonnais des accidents vasculaires cérébraux en 20 ans d’activité. Revue Neurologique, 164, 138-147. http://dx.doi.org/10.1016/j.neurol.2007.06.003 [34] Dowlatshahi, D., Demuchuk, A.M., Flaherty, M.L., Ali, M., Lyden, P.L., Faan, E.E., et al. (2011) Defining he- matoma expansion in intracerebral hemorrhage: Relation- ship with patient outcomes. Neurology, 76, 1238-1244. http://dx.doi.org/10.1212/WNL.0b013e3182143317 [35] Gosse, P. and Cremer, A. (2011) Hypertrophie ventricul- aire gauche chez l’hypertendu: Mise au point et point de vue. AMC-Pratique, 202, 16-20. [36] Godoy, D.A., Piñero, G. and Di Napoli, M. (2006) Pre- dicting mortality in spontaneous intracerebral hemorrhage: Can modification to original score improve the prediction? Stroke, 37, 1038-1044. http://dx.doi.org/10.1161/01.STR.0000206441.79646.49
|