Vol.2, No.9, 521-524 (2013) Case Reports in Clinical Medicine
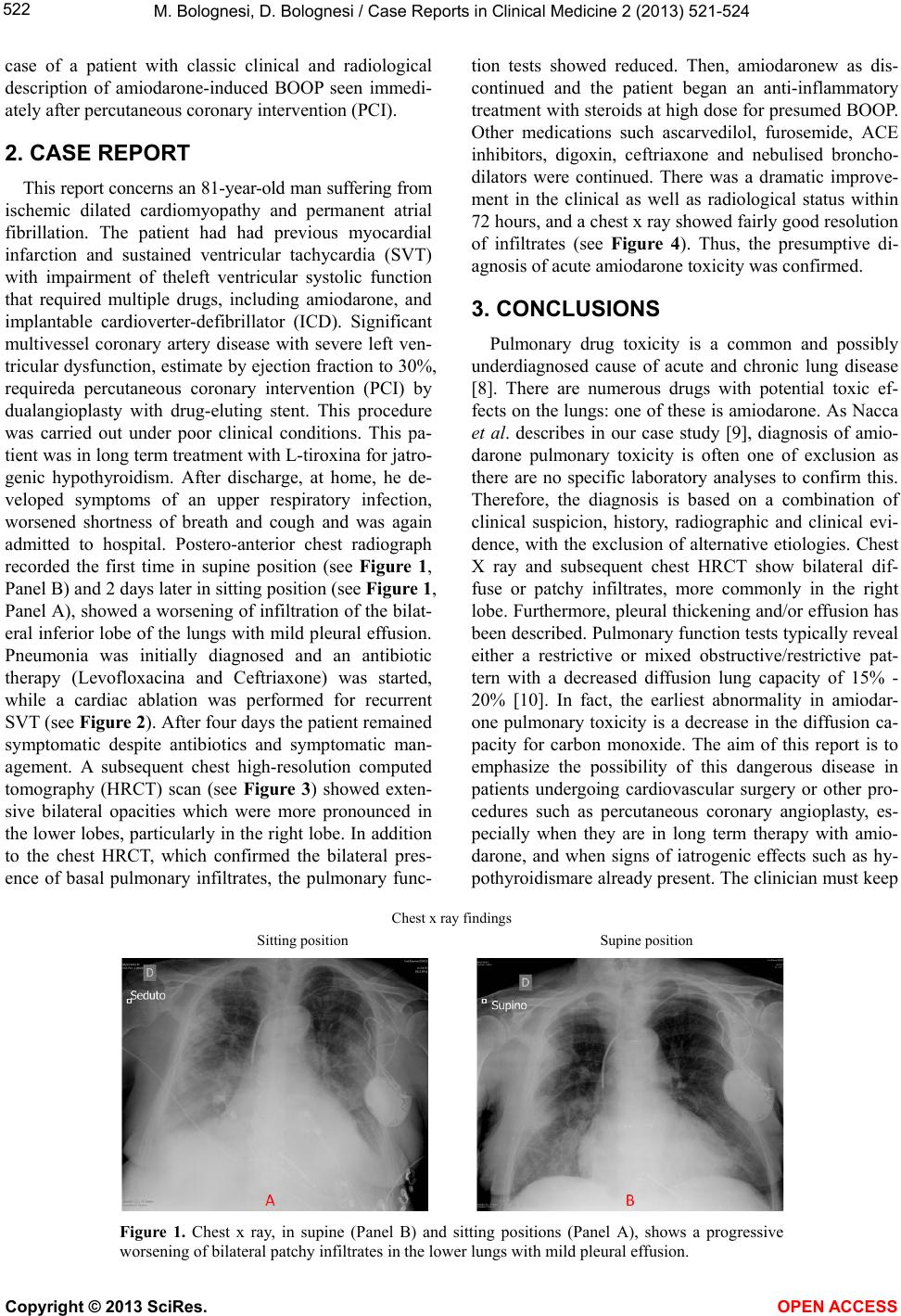
http://dx.doi.org/10.4236/crcm.2013.29136
Amiodarone-induced bronchiolitis obliterans
organizing pneumonia in patient following
percutaneous transluminal coronary angioplasty
Massimo Bolognesi1*, Diletta Bolognesi2
1General Practice Medicine-Primary Care , C esena, Ita ly; *Corresponding Author: massbolo1@tin.it
2Territorial Medicine-Primary Care, Cesena, Italy
Received 23 September 2013; revised 20 October 2013; accepted 18 November 2013
Copyright © 2013 Massimo Bolognesi, Diletta Bolognesi. This is an open access article distributed under the Creative Commons
Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited. In accordance of the Creative Commons Attribution License all Copyrights © 2013 are reserved for SCIRP and the
owner of the intellectual property Massimo Bolognesi, Diletta Bolognesi. All Copyright © 2013 are guarded by law and by SCIRP as
a guardian.
ABSTRACT
Background: Many patients are affected by idio-
pathicbronchiolitis obliterans organizing pneu-
monia (BOOP). There are several know n causes
of BOOP, and several systemic disorders have
BOOP as an associated primary pulmonary le-
sion. Numerous agents including cytotoxic and
noncytotoxic drugs have the potential to cause
pulmonary toxicity. Descriptions of amiodarone-
related BOOP continue to be reported through-
out the world. Case Report: We reported a pa-
tient with original clinical presentation who de-
veloped recurrent sustained ventricular tachy-
cardia (SVT) despite the presence of implant able
cardioverter-defibrillator (ICD), hypoxaemia and
interstitial pneumonitis in both lung bases. After
percutaneous transluminal coro nary angioplasty,
he developed bronchiolitis obliterans organizing
pneumonia (BOOP). Conclusions: To our know-
ledge, such complications after percutaneous
coronary procedure in patients with amiodarone
therapy for arrhythmia prophylaxis, are not very
frequent in literature.
Keywords: Percutaneous Tr ansluminal Coronary
Angioplasty; Amiodarone; BOOP
1. INTRODUCTION
Bronchiolitis obliterans organizing pneumonia (BOOP)
is a distinct entity with various clinical, rad iographic and
histologic features [1]. The term Bronchiolitis obliterans
organizing pneumonia was first described in the early
1980s as a clinical pathologic syndrome characterized
symptomatically by subacute and chronic respiratory
illness, histopathologically by granulation tissue in the
bronchiolar lumen, alveolar ducts with some alveoli as-
sociated with a variable degree of interstitial and air
space infiltration by mononuclear cells with foamy
macrophages [2]. In most cases, the aetiology remains
unknown, although it has been associated with specific
diseases and causes including bacterial or viral infections,
diseases of the connective tissue, radiation therapy, mye-
lodysplastic syndrome, cocaine abuse, human immuno-
deficiency virus (HIV) infection, gastrointestinal disor-
ders, coronary artery bypassing grafting, and more vari-
ous pharmaceutical drugs [3]. Amiodarone is one of the
principal drugs involved in pulmonary toxicity, espe-
cially in patients undergoing cardiac surgery [4]. The
manifestations of pulmonary toxicity from amiodarone,
described in the literature include bronchiolitis obliter-
ans with or without sign s of organizing pneumonia, with
or without chronic interstitial fibrosis, pulmonary solitary
or multiple masses or respiratory distress syndrome [5-
11]. A tissue biopsy specimen is needed for a precise
diagnosis, but clinicoradiologic characteristics deter-
mined through biopsy-based studies may provide suffi-
cient diagnostic information. In fact, the ch est radiograph
showed the typical bilateral patchy (alveolar) infiltrate
and even more, the chest computed tomographic scan
showed the same findings, with bilateral areas of con-
solidation and ground glass opacities, usually with a pe-
ripheral location [6]. High-resolution chest computed
tomographic scans showed two types of linear opacities
that usually occurred in the lower lobes, frequently asso-
ciated with multifocal areas of consolidation, and usually
completely resolved with treatment [7]. We report here a
Copyright © 2013 SciRes. OPEN ACCESS