Vol.2, No.9, 513-516 (2013) Case Reports in Clinical Medicine
http://dx.doi.org/10.4236/crcm.2013.29134
Fungal sinusitis with ocular involvement: Case report
Achyut N. Pandey1*, Anil Kakde2
1Department of Ophthalmolog y, VCSG Medical College and Research Institute, Srinagar-Garhwal, Uttarakhand, India;
*Corresponding Author: achyutpandey@gmail.com
2Eye Q Super Speciality Eye Hospital, Gurgaon, India
Received 7 October 2013; revised 5 November 2013; accepted 3 December 2013
Copyright © 2013 Achyut N. Pandey, Anil Kakde. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In accordance of the Creative Commons Attribution License all Copyrights © 2013 are reserved for SCIRP and the owner of the
intellectual property Achyut N. Pandey, Anil Kakde. All Copyright © 2013 are guarded by law and by SCIRP as a guardian.
ABSTRACT
Rhino-orbital-cerebral mucormycosis (ROCM) is
an acute, often fatal, fungal infection caused by
members of the class Zygomycetes and the or-
der Mucorales. The genus Rhizopus accounts
for most cases of ROCM. The disease is char-
acterized by fungal hyphal invasion of blood
vessels resulting in thrombosis and i nfarction of
the nasal, paranasal sinus, orbital, and cerebral
tissues. The most commonly associated condi-
tion is diabetes mellitus; other associated con-
ditions include immunocompromised states, re-
nal disease, deferoxamine use and acidotic sta-
tes. The most frequent sites of infection are
pulmonary, rhinocerebral, cutaneous and dis-
seminated. Rhino-orbital and Rhino-cerebral are
two forms of the disease. As such the condition
is a medical emergency. Early recognition and
treatment are essential because it may lead to
death in a few days. CROP usually begins in the
palate or paranasal sinuses and rapidly spreads
to the orbital contents. Proptosis, loss of vision
and ophthalmoplegia occur and death from ce-
rebral involvement commonly ensues. The fun-
gus tends to invade arteries and cause throm-
bosis and tissue infarction. Rhizopus is the
most commonly isolated genus in CROP, ac-
counting for almost all cases. The diagnosis can
be strongly suspected by the characteristic
clinical manifestations. Therapy includes the
treatment of the underlying disease, surgical
excision of the necrotic tissue containing fungal
element s and the systemic administr ation of am-
photericin-B. Here we report the clinical fea-
tures of a 32-years-old man presented mucor-
mycosis.
Keywords: Diabetes Mellitus; Mucormycosis;
Rhizopus spp.
1. CASE REPORT
A 32-years-old male patient presented a history of pain
in the nose and defective vision in the left eye since one
week. The pain was not relieved. He was apparently all
right one week prior. He was a diabetic incidientally
found one week back only. On admission, he was found
to be a afebrile, conscious and well oriented to the time
and place, with a BP of 140/90 mmHg, a pulse of 82/min
and with a swelling on the nose. Vision is in RE 6/18 and
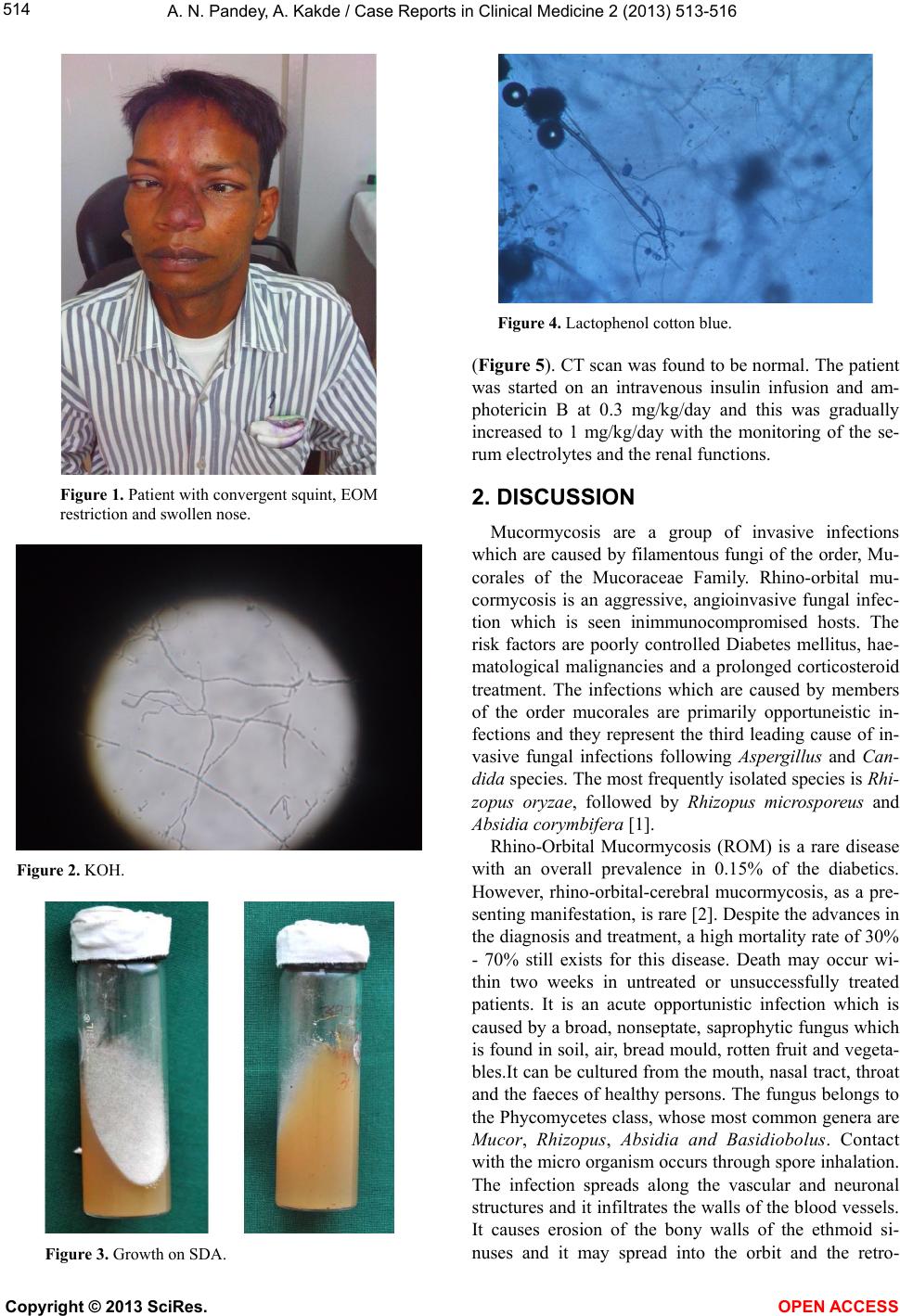
LE 6/HM. On examination patient is found to have con-
vergent squint. Extra ocular movements were restricted
in all six gazes, indicating the involvement of 3, 5 and 6
cranial nerve (Figure 1). Corneal sensation is decreased
in BE .There was no proptosis presented. IOP is in RE
22.4 and LE 18.9. People in both eyes were round, re-
acting to light both direct and consensual light reaction.
Pt was dilated for fundus examination, and BE fundus
found to be normal. His fasting blood sugar was 296
mg/dl, sodium was 12 mEq/L, potassium was 2.5 mEq/L.,
urea was 47 mg/dl, creatinin e was 0.9 mg/dl and haemo-
globin was 11.7 gm%. All other lab investigations are
found to be normal. His nasal swab and maxillary and eth-
moid sinus curettages were received in the microbiology
laboratory for KOH mounts and fungal cultures to check
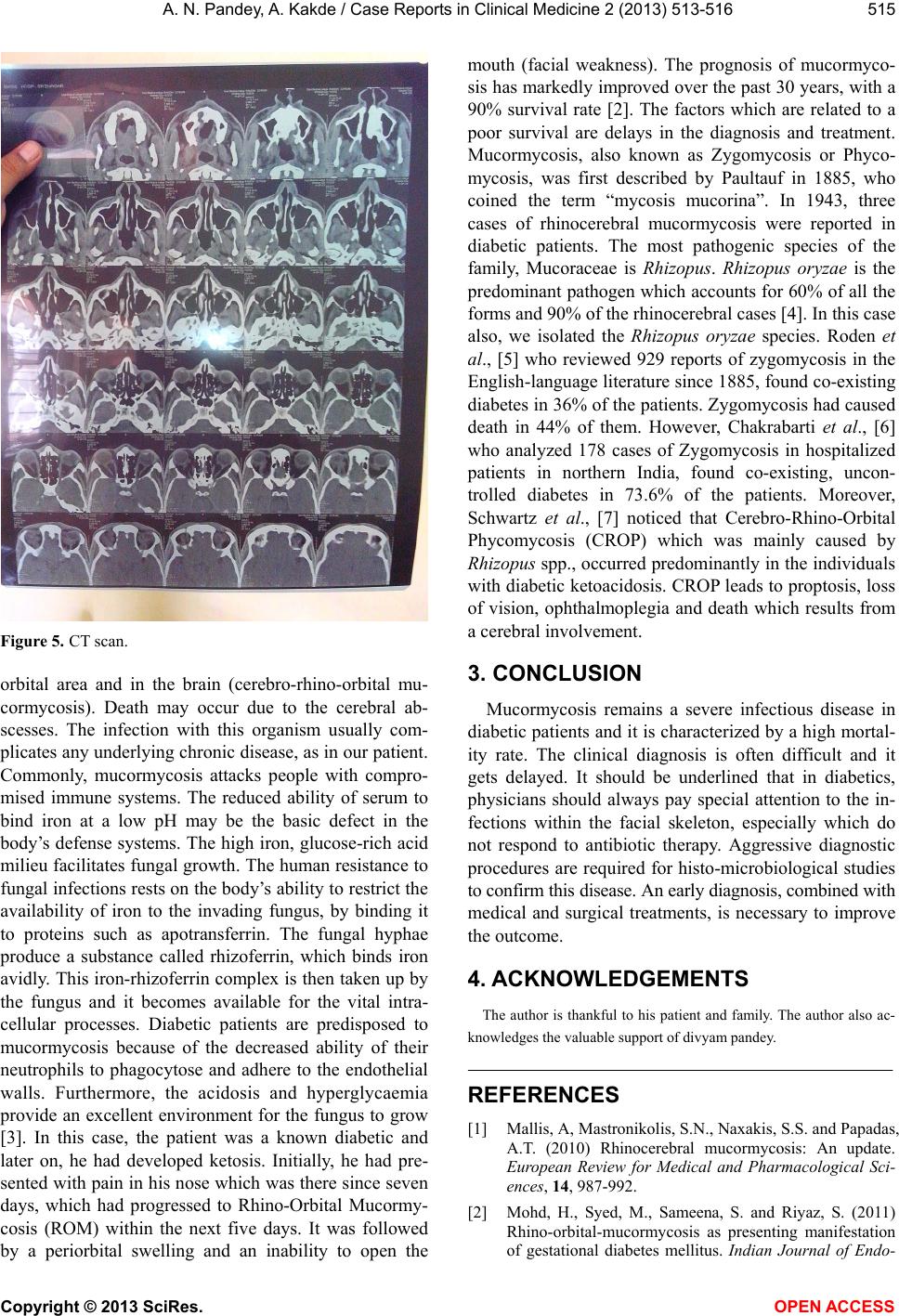
for mucormycosis. The microscopic examination of the
biopsy material and the nasal discharge was done in 10%
KOH wet mounts. It showed the characteristic broad,
aseptate, branched hyphae (Figures 2, 3). The fungus
was grown on Sabouraud’s dextrose agar at 37˚C. A mi-
croscopic examination of the growth which was done in
a lactophenol cotton blue mount, revealed that it was Rhi-
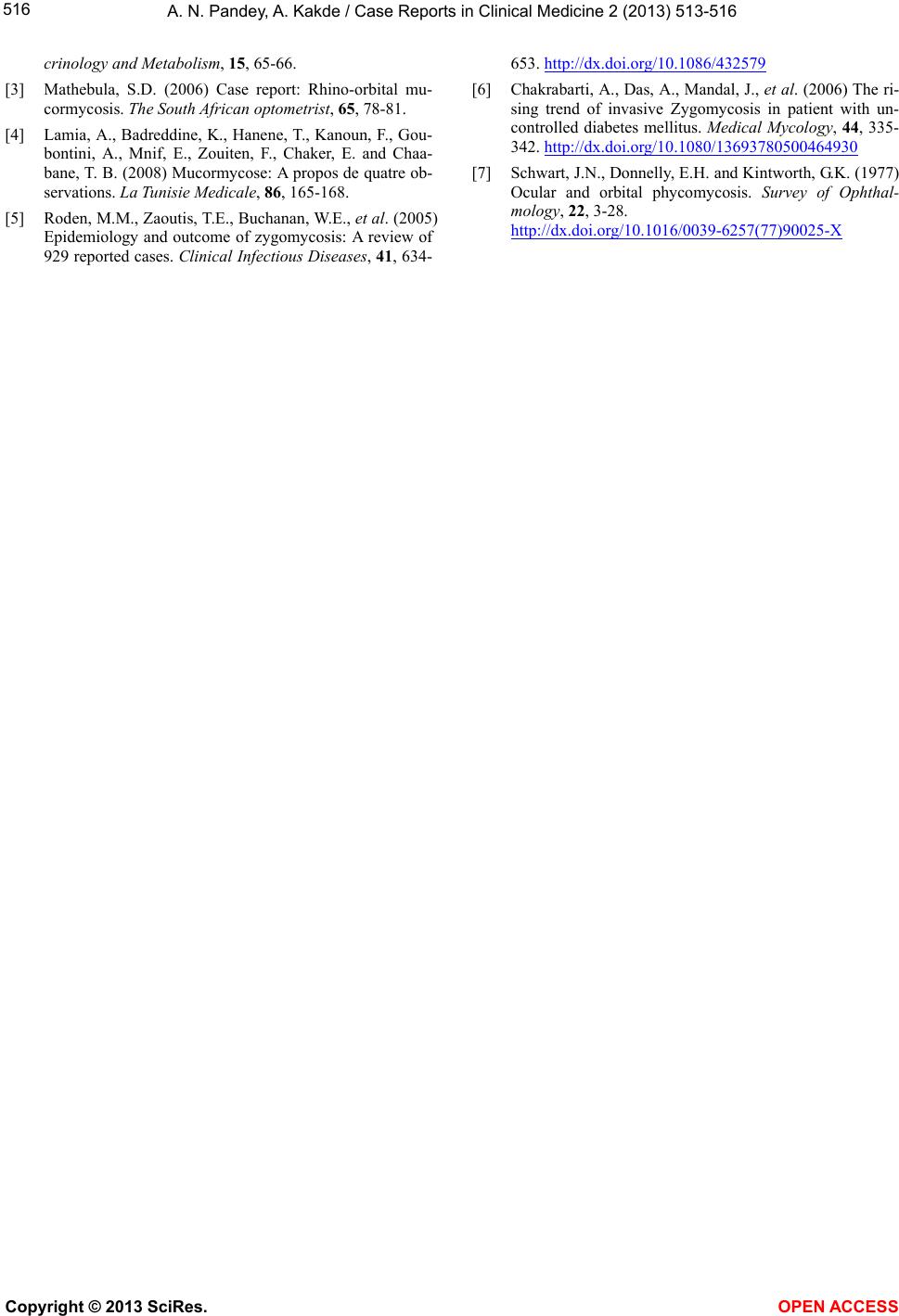
zopus (Figure 4). Further patient is advised for CT scan
orbit and para nasal sinuses for orbital or cerebral spread
Copyright © 2013 SciRes. OPEN A CCESS