D. HIRANO ET AL.
192
In a cohort of 539 patients with systemic lupus ery-
thematosus, Zonana-Nacach et al. found no association
between intravenous steroid therapy and osteoporotic
fractures, but did find an association with high dose oral
steroids, reporting a strong association between cumula-
tive prednisolone dose and adverse effects [20]. In our
study, we fortunately did not experience late-onset ad-
verse effects such as osteoporotic fractures, steroid dia-
betes mellitus, and short stature. This might be because
we administered a lower dose of oral mPSL (1 mg/kg/d,
maximum 30 mg/d) on alternate days after LDMPT.
The minimum effective dose of mPSL is unclear.
While one study has suggested that doses as low as 320
mg administered intravenously or intramuscularly are as
effective as 1 g of intravenous mPSL [21], another study
has shown that reducing the intravenous mPSL dose
from 1 g to 500 mg results in a substantial loss of effi-
cacy [22]. Our findings suggest that LDMPT could be a
potentially effective and safe alternative for pediatric pa-
tients with various glomerular diseases. However, more
studies are needed to further characterize the optimal
dosages and mechanisms of action of MPT.
5. Limitations
The present study was a retrospective analysis of treat-
ment performed at a single center, so there may be some
selection bias in the cohort. The single center cohort de-
sign also limits the external validity of our findings. In
addition, we could not determine the true frequency of
minor adverse effects such as metallic taste and facial
flushing because of the manner in which this retrospec-
tive study was performed. However, we are confident
that we did not miss any serious treatment complications.
6. Conclusion
This case series indicated that LDMPT might have an
acceptably low risk of significant adverse effects and
therefore can be an effective treatment modality for pe-
diatric patients with various glomerular diseases.
7. Tables
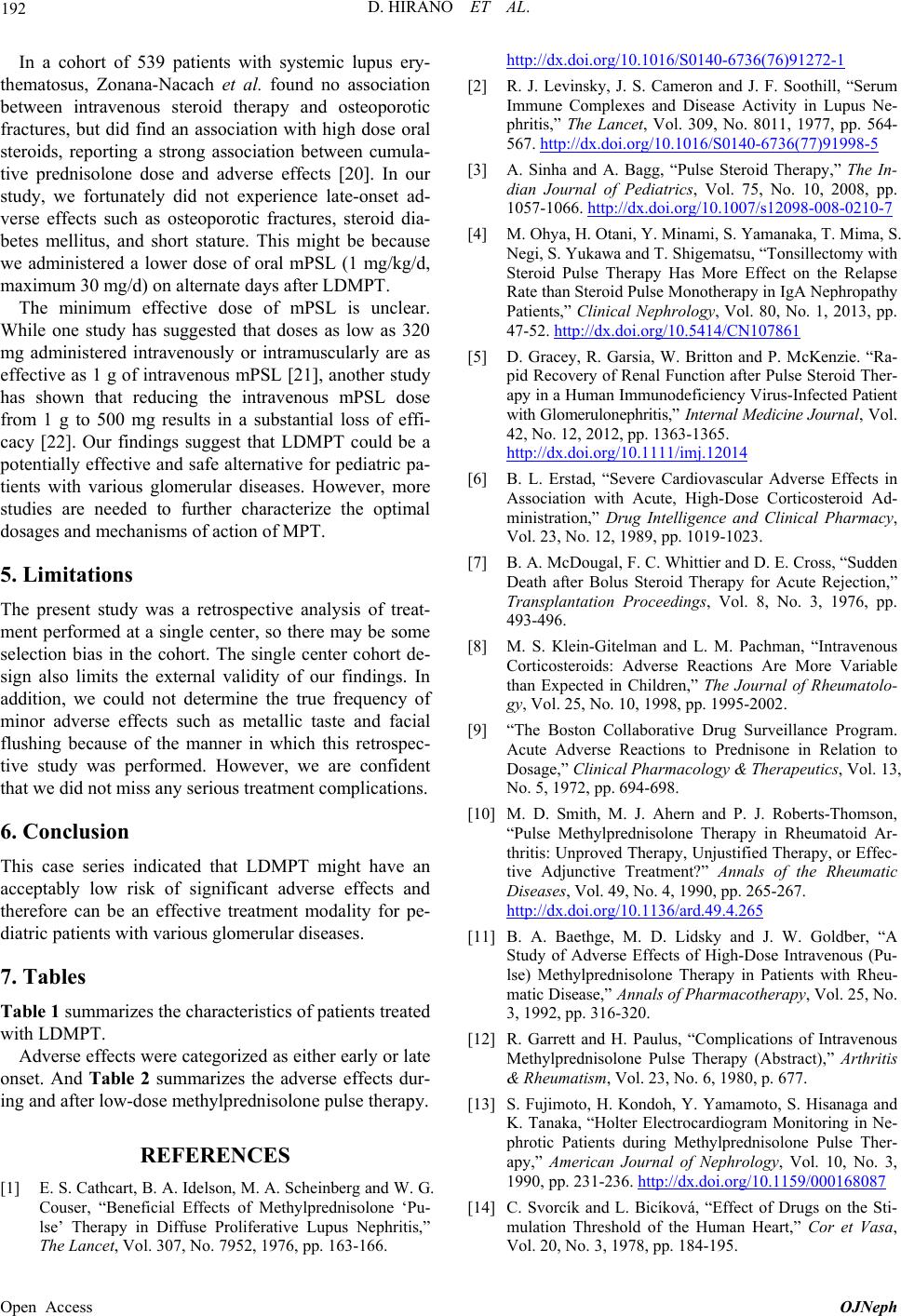
Table 1 summarizes the characteristics of patients treated
with LDMPT.
Adverse effects were categorized as either early or late
onset. And Table 2 summarizes the adverse effects dur-
ing and after low-dose methylprednisolone pulse therapy.
REFERENCES
[1] E. S. Cathcart, B. A. Idelson, M. A. Scheinberg and W. G.
Couser, “Beneficial Effects of Methylprednisolone ‘Pu-
lse’ Therapy in Diffuse Proliferative Lupus Nephritis,”
The Lancet, Vol. 307, No. 7952, 1976, pp. 163-166.
http://dx.doi.org/10.1016/S0140-6736(76)91272-1
[2] R. J. Levinsky, J. S. Cameron and J. F. Soothill, “Serum
Immune Complexes and Disease Activity in Lupus Ne-
phritis,” The Lancet, Vol. 309, No. 8011, 1977, pp. 564-
567. http://dx.doi.org/10.1016/S0140-6736(77)91998-5
[3] A. Sinha and A. Bagg, “Pulse Steroid Therapy,” The In-
dian Journal of Pediatrics, Vol. 75, No. 10, 2008, pp.
1057-1066. http://dx.doi.org/10.1007/s12098-008-0210-7
[4] M. Ohya, H. Otani, Y. Minami, S. Yamanaka, T. Mima, S.
Negi, S. Yukawa and T. Shigematsu, “Tonsillectomy with
Steroid Pulse Therapy Has More Effect on the Relapse
Rate than Steroid Pulse Monotherapy in IgA Nephropathy
Patients,” Clinical Nephrology, Vol. 80, No. 1, 2013, pp.
47-52. http://dx.doi.org/10.5414/CN107861
[5] D. Gracey, R. Garsia, W. Britton and P. McKenzie. “Ra-
pid Recovery of Renal Function after Pulse Steroid Ther-
apy in a Human Immunodeficiency Virus-Infected Patient
with Glomerulonephritis,” Internal Medicine Journal, Vol.
42, No. 12, 2012, pp. 1363-1365.
http://dx.doi.org/10.1111/imj.12014
[6] B. L. Erstad, “Severe Cardiovascular Adverse Effects in
Association with Acute, High-Dose Corticosteroid Ad-
ministration,” Drug Intelligence and Clinical Pharmacy,
Vol. 23, No. 12, 1989, pp. 1019-1023.
[7] B. A. McDougal, F. C. Whittier and D. E. Cross, “Sudden
Death after Bolus Steroid Therapy for Acute Rejection,”
Transplantation Proceedings, Vol. 8, No. 3, 1976, pp.
493-496.
[8] M. S. Klein-Gitelman and L. M. Pachman, “Intravenous
Corticosteroids: Adverse Reactions Are More Variable
than Expected in Children,” The Journal of Rheumatolo-
gy, Vol. 25, No. 10, 1998, pp. 1995-2002.
[9] “The Boston Collaborative Drug Surveillance Program.
Acute Adverse Reactions to Prednisone in Relation to
Dosage,” Clinical Pharmacology & Therapeutics, Vol. 13,
No. 5, 1972, pp. 694-698.
[10] M. D. Smith, M. J. Ahern and P. J. Roberts-Thomson,
“Pulse Methylprednisolone Therapy in Rheumatoid Ar-
thritis: Unproved Therapy, Unjustified Therapy, or Effec-
tive Adjunctive Treatment?” Annals of the Rheumatic
Diseases, Vol. 49, No. 4, 1990, pp. 265-267.
http://dx.doi.org/10.1136/ard.49.4.265
[11] B. A. Baethge, M. D. Lidsky and J. W. Goldber, “A
Study of Adverse Effects of High-Dose Intravenous (Pu-
lse) Methylprednisolone Therapy in Patients with Rheu-
matic Disease,” Annals of Pharmacotherapy, Vol. 25, No.
3, 1992, pp. 316-320.
[12] R. Garrett and H. Paulus, “Complications of Intravenous
Methylprednisolone Pulse Therapy (Abstract),” Arthritis
& Rheumatism, Vol. 23, No. 6, 1980, p. 677.
[13] S. Fujimoto, H. Kondoh, Y. Yamamoto, S. Hisanaga and
K. Tanaka, “Holter Electrocardiogram Monitoring in Ne-
phrotic Patients during Methylprednisolone Pulse Ther-
apy,” American Journal of Nephrology, Vol. 10, No. 3,
1990, pp. 231-236. http://dx.doi.org/10.1159/000168087
[14] C. Svorcík and L. Bicíková, “Effect of Drugs on the Sti-
mulation Threshold of the Human Heart,” Cor et Vasa,
Vol. 20, No. 3, 1978, pp. 184-195.
Open Access OJNeph