F. Morbeck et al. / Case Reports in Clinical Medicine 2 (2013) 499-501
Copyright © 2013 SciRes. OPEN ACCESS
501
differential diagnosis with infection, infarction, and ab-
scess should be performed. The use of PET/CT has an
indeterminate finding, because both malignancies such as
infection and inflammation are often hypermetabolic.
These findings cause many false positives in endemic
areas [5]. Surgical treatment should not be the first op-
tion in cases of cryptococcal infection. However, when it
does not respond adequately to drug therapy, a resection
of the lesion (usually a lobectomy) should be performed.
by ultrasound.
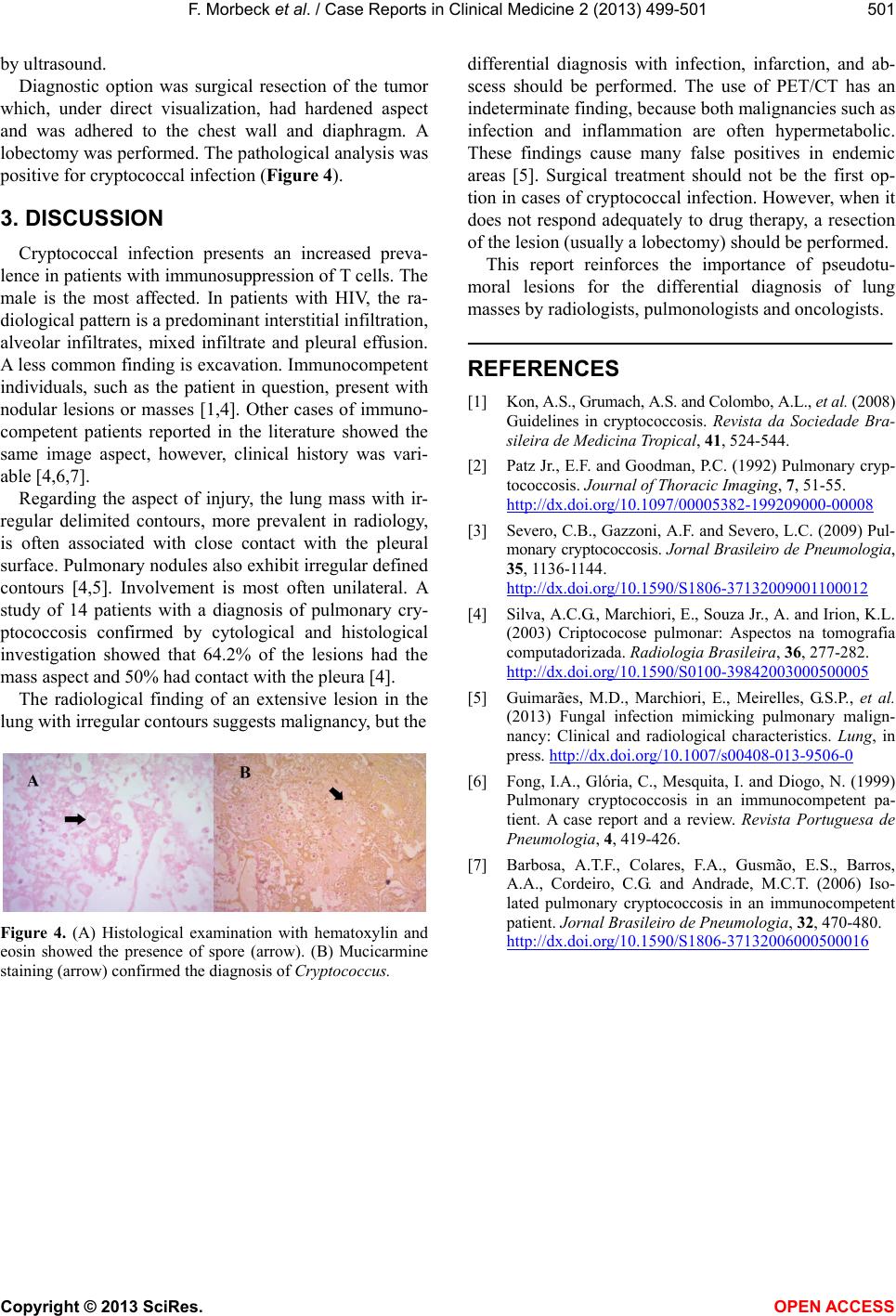
Diagnostic option was surgical resection of the tumor
which, under direct visualization, had hardened aspect
and was adhered to the chest wall and diaphragm. A
lobectomy was performed. The pathological analysis was
positive for cryptococcal infection (Figur e 4).
3. DISCUSSION
Cryptococcal infection presents an increased preva-
lence in patients with immunosuppression of T cells. The
male is the most affected. In patients with HIV, the ra-
diological pattern is a predomin ant interstitial infiltration,
alveolar infiltrates, mixed infiltrate and pleural effusion.
A less common finding is excavation. Immunocompetent
individuals, such as the patient in question, present with
nodular lesions or masses [1,4]. Other cases of immuno-
competent patients reported in the literature showed the
same image aspect, however, clinical history was vari-
able [4,6,7].
This report reinforces the importance of pseudotu-
moral lesions for the differential diagnosis of lung
masses by radiologists, pulmonologists and oncologists.
REFERENCES
[1] Kon, A.S., Grumach, A.S. and Colombo, A.L., et al. (2008)
Guidelines in cryptococcosis. Revista da Sociedade Bra-
sileira de Medicina Tropical, 41, 524-544.
[2] Patz Jr., E.F. and Goodman, P. C. (1992) Pulmonary cryp-
tococcosis. Journal of Thoracic Imaging, 7, 51-55.
http://dx.doi.org/10.1097/00005382-199209000-00008
Regarding the aspect of injury, the lung mass with ir-
regular delimited contours, more prevalent in radiology,
is often associated with close contact with the pleural
surface. Pulmonary nodules also exhibit irregular defined
contours [4,5]. Involvement is most often unilateral. A
study of 14 patients with a diagnosis of pulmonary cry-
ptococcosis confirmed by cytological and histological
investigation showed that 64.2% of the lesions had the
mass aspect and 50% had contact with the pleura [4].
[3] Severo, C.B., Gazzoni, A.F. and Severo, L.C. (2009) Pul-
monary cryptococcosis. Jornal Brasileiro de Pneumologia,
35, 1136-1144.
http://dx.doi.org/10.1590/S1806-37132009001100012
[4] Silva, A.C.G., Marchiori, E., Souza Jr., A. and Irion, K.L.
(2003) Criptococose pulmonar: Aspectos na tomografia
computadorizada. Radiologia Brasileira, 36, 277-282.
http://dx.doi.org/10.1590/S0100-39842003000500005
[5] Guimarães, M.D., Marchiori, E., Meirelles, G.S.P., et al.
(2013) Fungal infection mimicking pulmonary malign-
nancy: Clinical and radiological characteristics. Lung, in
press. http://dx.doi.org/10.1007/s00408-013-9506-0
The radiological finding of an extensive lesion in the
lung with irregular contours suggests malignancy, but the
[6] Fong, I.A., Glória, C., Mesquita, I. and Diogo, N. (1999)
Pulmonary cryptococcosis in an immunocompetent pa-
tient. A case report and a review. Revista Portuguesa de
Pneumologia, 4, 419-426.
[7] Barbosa, A.T.F., Colares, F.A., Gusmão, E.S., Barros,
A.A., Cordeiro, C.G. and Andrade, M.C.T. (2006) Iso-
lated pulmonary cryptococcosis in an immunocompetent
patient. Jornal Brasileiro de Pneumologia, 32, 470-480.
http://dx.doi.org/10.1590/S1806-37132006000500016
Figure 4. (A) Histological examination with hematoxylin and
eosin showed the presence of spore (arrow). (B) Mucicarmine
staining (arrow) confirmed the diagnosis of Cryptococcus.