Invasive Fungal Sinusitis in Immunocompromised Patients:
A Multicenter, University Hospital Experience in Shiraz 267
ed morbidity and mortality in high risk patients.
5. Conclusion
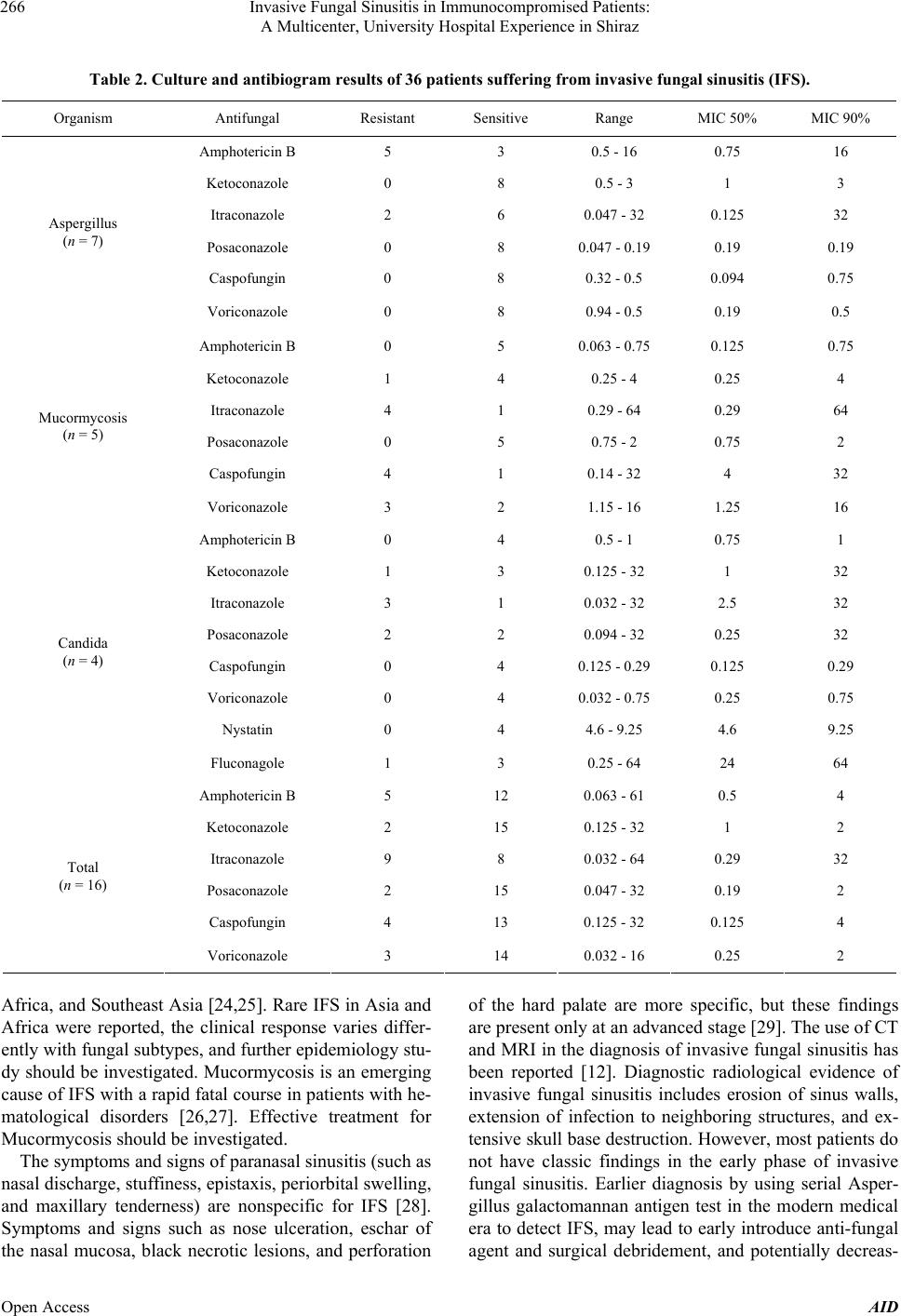
In conclusion, DM is the most common predisposing fac-
tor for IFS followed by ALL and AML. The most com-
mon aetiology of IFS was found to be Aspergillus fumi-
gant followed by M ucorm y c osi s and Candida. None of an-
tifungal agents could successfully cover all the species.
6. Acknowledgments
This research project was financially supported by Health
Policy Research Center affiliated with Shiraz University
of Medical Sciences. Also, there is no conflict of interest
to be declared regarding this manuscript.
REFERENCES
[1] J. Crawford, D. C. Dale and G. H. Lyman, “Chemothera-
py-Induced Neutropenia: Risks, Consequences, and New
Directions for Its Management,” Cancer, Vol. 100, 2004,
pp. 228-237. http://dx.doi.org/10.1002/cncr.11882
[2] S. Vento and F. Cainelli, “Infections in Patients with Can-
cer Undergoing Chemotherapy: Etiology, Prevention, and
Treatment,” Lancet Oncology, Vol. 4, 2003, pp. 595-604.
http://dx.doi.org/10.1016/S1470-2045(03)01218-X
[3] E. J. Bow, “Management of the Febrile Neutropenic Can-
cer Patient: Lessons from 40 Years of Study,” Clin Mi-
crobiol Infect, Vol. 11, No. S5, 2005, pp. 24-29.
http://dx.doi.org/10.1111/j.1469-0691.2005.01240.x
[4] N. G. Almyroudis and B. H. Segal, “Prevention and Treat-
ment of Invasive Fungal Diseases in Neutropenic Pa-
tients,” Current Opinion in Infectious Diseases, Vol. 22,
2009, pp. 385-393.
http://dx.doi.org/10.1097/QCO.0b013e32832e074d
[5] S. Ascioglu, J. H. Rex, B. de Pauw, J. E. Bennett, J. Bille,
F. Crokaert, et al., “Invasive Fungal Infections Coopera-
tive Group of the European Organization for Research
and Treatment of Cancer; Mycoses Study Group of the
National Institute of Allergy and Infectious Diseases. De-
fining Opportunistic Invasive Fungal Infections in Immu-
nocompromised Patients with Cancer and Hematopoietic
Stem Cell Transplants: An International Consensus,” Cli-
nical Infectious Diseases, Vol. 34, 2002, pp. 7-14.
http://dx.doi.org/10.1086/323335
[6] B. De Pauw, T. J. Walsh, J. P. Donnelly, D. A. Stevens, J.
E. Edwards, T. Calandra, et al., “European Organization
for Research and Treatment of Cancer/Invasive Fungal
Infections Cooperative Group; National Institute of Aller-
gy and Infect ious Diseases Mycose s Study Group (EORTC/
MSG) Consensus Group. Revised Definitions of Invasive
Fungal Disease from the European Organization for Re-
search and Treatment of Cancer/Invasive Fungal Infec-
tions Cooperative Group and the National Institute of Al-
lergy and Infectious Diseases Mycoses Study Group
(EORTC/MSG) Consensus Group,” Clinical Infectious
Diseases, Vol. 46, 2008, pp. 1813-1821.
http://dx.doi.org/10.1086/588660
[7] R. Martino and M. Subira, “Invasive Fungal Infections in
Hematology: New Trends,” Annals of Hematology, Vol.
81, 2002, pp. 233-243.
http://dx.doi.org/10.1007/s00277-002-0466-3
[8] E. J. Anaissie, “Diagnosis and Therapy of Fungal Infec-
tion in Patients with Leukemia—New Drugs and Immu-
notherapy,” Best Practice & Research Clinical Haemato-
logy, Vol. 21, 2008, pp. 683-690.
http://dx.doi.org/10.1016/j.beha.2008.10.001
[9] R. D. deShazo, K. Chapin and R. E. Swain, “Fungal Sinu-
sitis,” The New England Journal of Medicine, Vol. 337,
1997, pp. 254-259.
http://dx.doi.org/10.1056/NEJM199707243370407
[10] S. L. Parikh, G. Venkatraman and J. M. DelGaudio, “In-
vasive Fungal Sinusitis: A 15-Year Review from a Single
Institution,” American Journal of Rhinology, Vol. 18,
2004, pp. 75-81.
[11] W. T. Anselmo-Lima, R. P. Lopes, F. C. Valera and R. C.
Demarco, “Invasive Fungal Rhinosinusitis in Immuno-
compromised Patients,” Rhinology, Vol. 42, 2004, pp.
141-144.
[12] R. C. Howells and H. H. Ramadan, “Usefulness of Com-
puted Tomography and Magnetic Resonance in Fulmi-
nant Invasive Fungal Rhinosinusitis,” American Journal
of Rhinology, Vol. 15, 2001, pp. 255-261.
[13] C. Y. Chen, W. H. Shen g, A. Ch eng, Y. C. Chen, W. Tsay ,
J. L. Tang, et al., “Invasive Fungal Sinusitis in Patients
with Hematological Malignancy: 15 Years Experience in
a Single University Hospital in Taiwan,” BMC Infect Di-
sease, Vol. 11, 2011, p. 250.
http://dx.doi.org/10.1186/1471-2334-11-250
[14] P. C. Iwen, M. E. Rupp and S. H. Hinric hs, “I nvasi ve Mold
Sinusitis: 17 Cases in Immunocompromised Patients and
Review of the Literature,” Clinical Infectious Diseases,
Vol. 24, 1997, pp. 1178-1184.
http://dx.doi.org/10.1086/513662
[15] P. E. Drakos, A. Nagler, R. Or, E. Naparstek, J. Kapelu-
shnik, D. Engelhard, G. Rahav, D. Ne’emean and S. Sla-
vin, “Invasive Fungal Sinusitis in Patients Undergoing
Bone Marrow Transplantation,” Bone Marrow Transplant,
Vol. 12, 1993, pp. 203-208.
[16] D. Saah, P. E. Drakos, J. Elidan, I. Braverman, R. Or and
A. Nagler, “Rhinocerebral Aspergillosis in Patients Un-
dergoing Bone Marrow Transplantation,” Annals of Oto-
logy, Rhinology, and Laryngology, Vol. 103, 1994, pp.
306-310.
[17] G. H. Talbot, A. Huang and M. Provencher, “Invasive
Aspergillus Rhinosinusitis in Patients with Acute Leuke-
mia,” Reviews of Infectious Diseases, Vol. 13, 1991, pp.
219-232. http://dx.doi.org/10.1093/clinids/13.2.219
[18] R. S. Weber and G. Lopez-Berestein, “Treatment of Inva-
sive Aspergillus Sinusitis with Liposomal-Amphotericin
B,” Laryngoscope, Vol. 97, 1987, pp. 937-941.
http://dx.doi.org/10.1288/00005537-198708000-00010
[19] A. Wald, W. Leisen ring, J. A. van Burik and R. A. Bow-
den, “Epidemiology of Aspergillus Infections in a Large
Open Access AID