Surgical Science, 2013, 4, 543-546
Published Online December 2013 (http://www.scirp.org/journal/ss)
http://dx.doi.org/10.4236/ss.2013.412105
Open Access SS
Electro-Anatomical Approach to Membranous Septal
Aneurysm: Potential as a Focus of Critical
Ventricular Arrhythmias*
Hajime Imura1, Hiroshige Murata2, Masami Ochi1
1Department of Cardiovascular Surgery, Nippon Medical School Hospital, Tokyo, Japan
2Department of Cardiology, Nippon Medical School Hospital, Tokyo, Japan
Email: himura@nms.ac.jp
Received November 8, 2013; revised November 28, 2013; accepted December 5, 2013
Copyright © 2013 Hajime Imura et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In accor-
dance of the Creative Commons Attribution License all Copyrights © 2013 are reserved for SCIRP and the owner of the intellectual
property Hajime Imura et al. All Copyright © 2013 are guarded by law and by SCIRP as a guardian.
ABSTRACT
Membranous septal aneurysm (MSA) is a rare anomaly and known to cause ventricular tachycardia and atrioventricular
block. However, underlying mechanisms have not been addressed in its long history. We report first 3-D electro-ana-
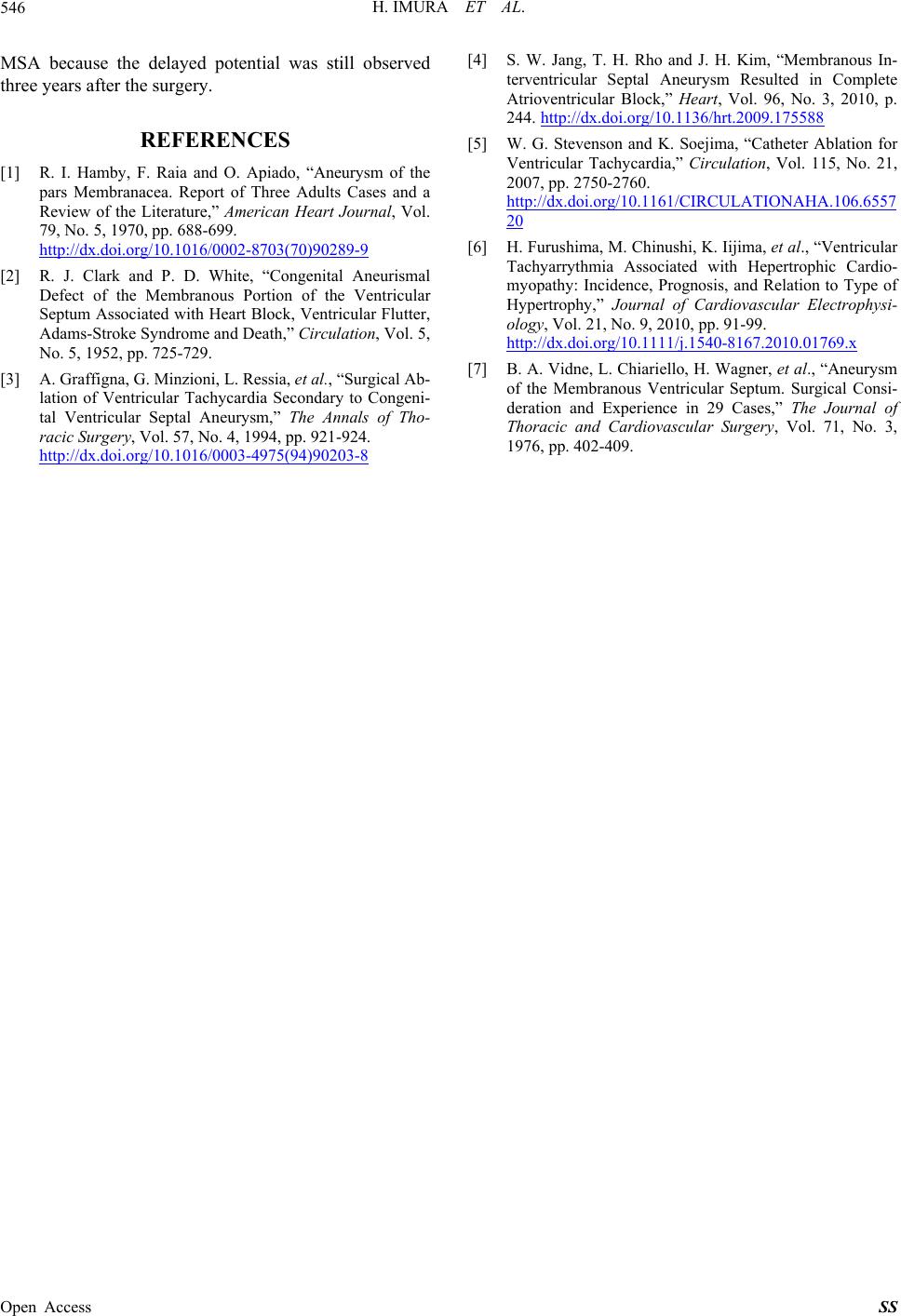
tomical mapping of MSA during and three years following the surgery. An elderly patient underwent a surgery for
MSA. In the map ping, we located the His b undle near MSA and observed delayed potentials arou nd MSA. Our report
showed that electrophysiological character of myocardium was changed around MSA and this change might be a reason
for ventricular tachycardia and atrioventricular block. An ordinary surgery for MSA might not resolve this problem
since we still observed delayed potentials three years after the surgery.
Keywords: Membranous Septal Aneurysm; Electro-Anatomical Mapping; Ventricular Tachycardia; Atrioventricular
Block
1. Introduction
The interventricular septum consists of muscular and
membranous components. Aneurysm of the membranous
portion, which was first described in 1826, is a cong enit-
al structure protruding into the right ventricle and can be
associated with various pathologies such as rupture, ob-
struction in the right ventricle and arrhythmias [1]. Ven-
tricular tachycardia (VT) and complete atrioventricular
block (AVB) were presented as complications of mem-
branous septal aneurysm (MSA) in old reports [2] and
still described as crucial problems in current literatures
[3,4], however, only few studies performed electrophy-
siological investigation for MSA in its long history. To
address the underlying mechanisms of such arrhythmias,
both anatomical and electrophysiological approaches are
indispensable, however, they have not been implemented
due to the rarity and difficulty to approach.
A 3-D electroanatomical mapping system (CARTO)
constructs a 3-D structure of the heart and draws a col-
or-coded map of impulse propagation and voltage on the
figure using electromagnetic technology. The system has
been well-established in describing the arrhythmogenic
substrate during open-heart surgery as well as catheter
ablation for VT. Here we report the first CARTO map-
ping during and three years following surgery for a case
of this rare pathology.
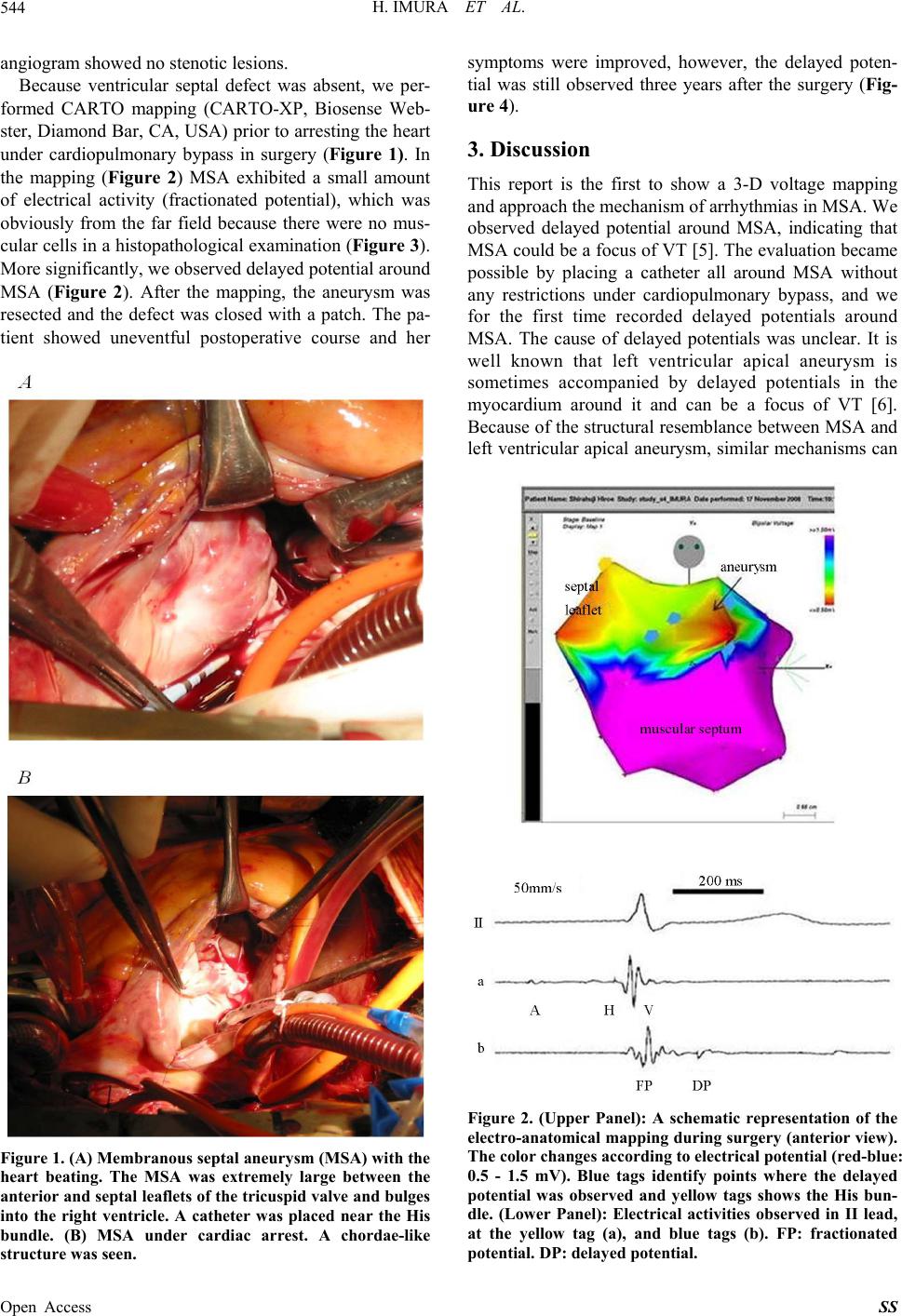
2. Case Presentation and Scientific Findings
An elderly patient was referred to our hosp ital for surgic-
al treatment of MSA. Because MSA’s size significantly
increased and she became symptomatic (chest discomfort
and palpitation), she elected to undergo surgical treat-
ment. She had no other medical history. In preoperative
examinations, her resting electrocardiogram showed
normal sinus rhythm with no abnormalities. No signifi-
cant ventricular or other arrhythmias were observed dur-
ing 24 hours of electrocardiogram monitoring. Also,
blood examination yielded no abnormal data. An echo-
cardiogram disclosed a large MSA (3.5 cm in height)
while ventricular septal defect was absent. Her coronary
*Conflict of interest: none declared.