Open Journal of Orthopedics, 2013, 3, 311-313
Published Online November 2013 (http://www.scirp.org/journal/ojo)
http://dx.doi.org/10.4236/ojo.2013.37057
Open Access OJO
311
Unusual Combination of Monteggia, Radius Shaft, and
Scaphoid Fractures*
A. Mechchat#, A. Mardy, M. Shimi, A. Elibrahimi, A. Elmrini
Department of Orthopaedics and Trauma Surgery B4, UH Hassan II, Fez, Morocco.
Email: #atif.mechchat@hotmail.fr, mr_titeuf82@hotmail.com, traumajid@yahoo.fr
Received September 5th, 2013; revised October 8th, 2013; accepted October 21st, 2013
Copyright © 2013 A. Mechchat et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
A rare combination of an ulnar fracture with posterior dislocation of the head of the radius and fracture of the radius
shaft concomitant with an ipsilateral scaphoid fracture is presented. To the best of our knowledge, no such case has
been reported. The mechanism of this fracture combination is discussed with respect to its role in producing the
Monteggia type II fracture. Treatment consisted of a combination of closed and open reduction with external fixation.
Keywords: Monteggia; Scaphoid; Radius; Posterior; Herbert
1. Introduction
The case of a young adult who sustained a posterior
Monteggia lesion with fracture of radius shaft and an
ipsilateral navicular fracture is presented. This is an ex-
tremely unusual injury. The mechanism of injury is dis-
cussed.
2. Case Report
A 26-year-old man fell backwards off a tree onto his
outstretched left arm. He described a twisting injury to
the arm at the time. The patient presented to a tertiary
trauma centre was seen with an obvious deformity of the
distal forearm and tenderness over the ipsilateral elbow.
Movements at the wrist and elbow were painful and re-
stricted, and no neurological or vascular deficits were
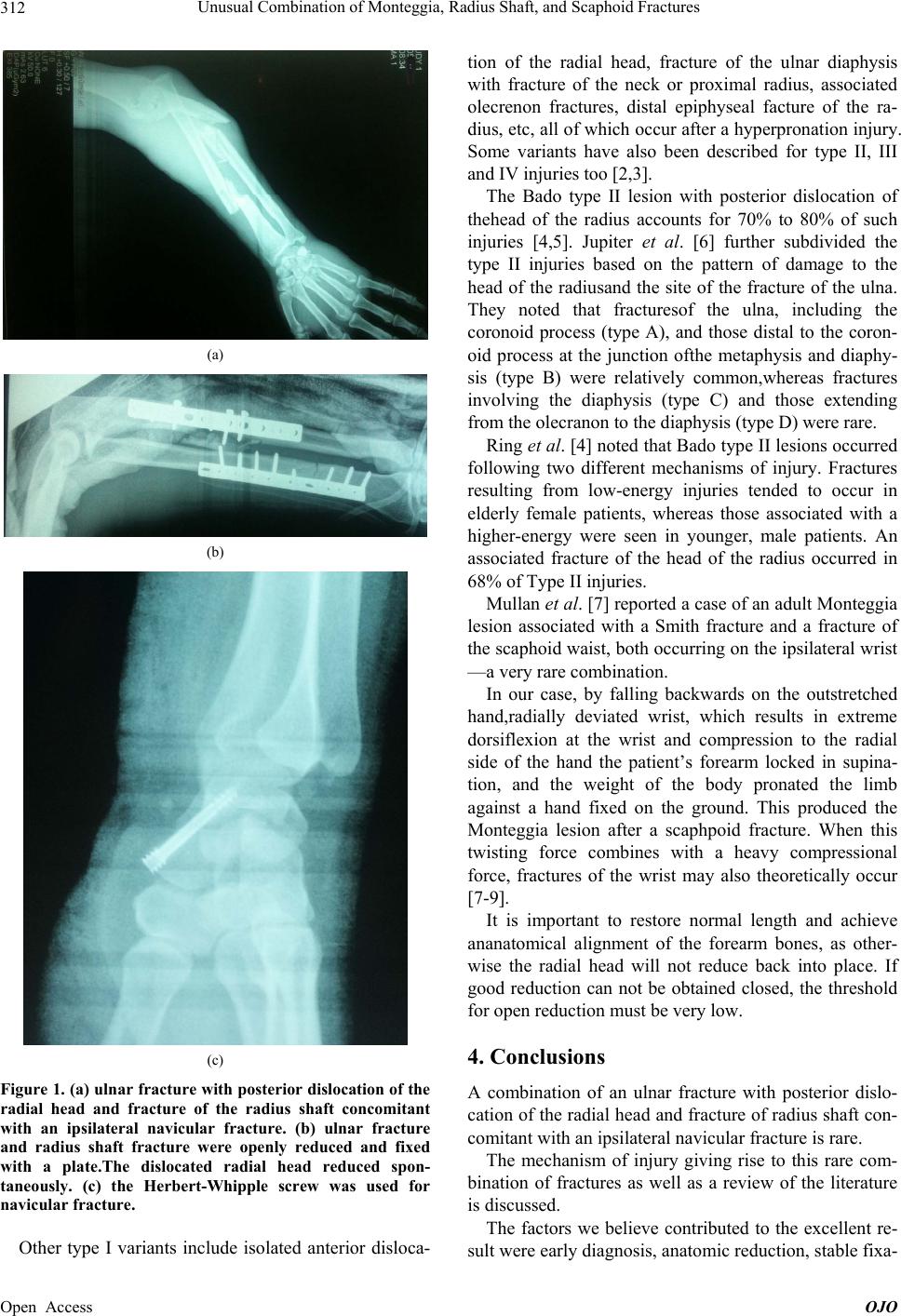
noted. Radiographs showed anulnar fracture with poste-
rior dislocation of the radial head and fracture of the ra-
dius shaft concomitant with an ipsilateral navicular frac-
ture. At the elbow the radial head was dislocated
posteriorly (Figure 1(a)). All injuries were of the closed
type. At surgery, the ulnar fracture was openly reduced
and fixed with a plate.The dislocation wasreduced by
manipulation after open reduction of the radial shaft
fracture, which was then fixed with a plate. The dislo-
cated radial head reduced spontaneously, and the wound
was sutured (Figure 1(b)). Open reduction and internal
fixation with the Herbert-Whipple screw was used for
navicular fracture (Figure 1(c)). The upper lumb was im-
mobilized in a light, above-elbow, full cast. The patient
made an uneventful recovery, and the cast was removed
at three weeks. Then active mobilization was started.
Consolidation was observed in 10 weeks. At his last re-
view eighteen month after injury, he had excellent wrist
and elbow movement, with full range of pronation and
supination.
3. Discussion
Any dislocation of the radial head with an ulnar fracture
constitutes a Monteggia lesion. Of the various classifica-
tions available, Bado’s [1] is the one that is almost uni-
versally in use.
Type I: anterior dislocation of the radial head, fracture
of the ulnar diaphysis at any level with anterior (volar)
angulation.
Type II: posterior or posterolateral dislocation of the
radial head, fracture of the ulnar diaphysis with posterior
(dorsal) angulation.
Type III: lateral or anterolateral dislocation of the ra-
dial head with fracture of the ulnar metaphysis or diaphy-
sis.
*Conflit of interest: No benefits in any form have been received or will
e received from a commercialparty related directly or indirectly to the
subject of this article.
#Corresponding author.
Type IV: anterior dislocation of the radial head, frac-
ture proximal third radius and fracture of the ulna at the
same level.