J. J. Wang et al. / J. Biomedical Science and Engineering 4 (2011) 122-129
128
complicated conductive components, compared to the
present study. In the present study, we apply an alternat-
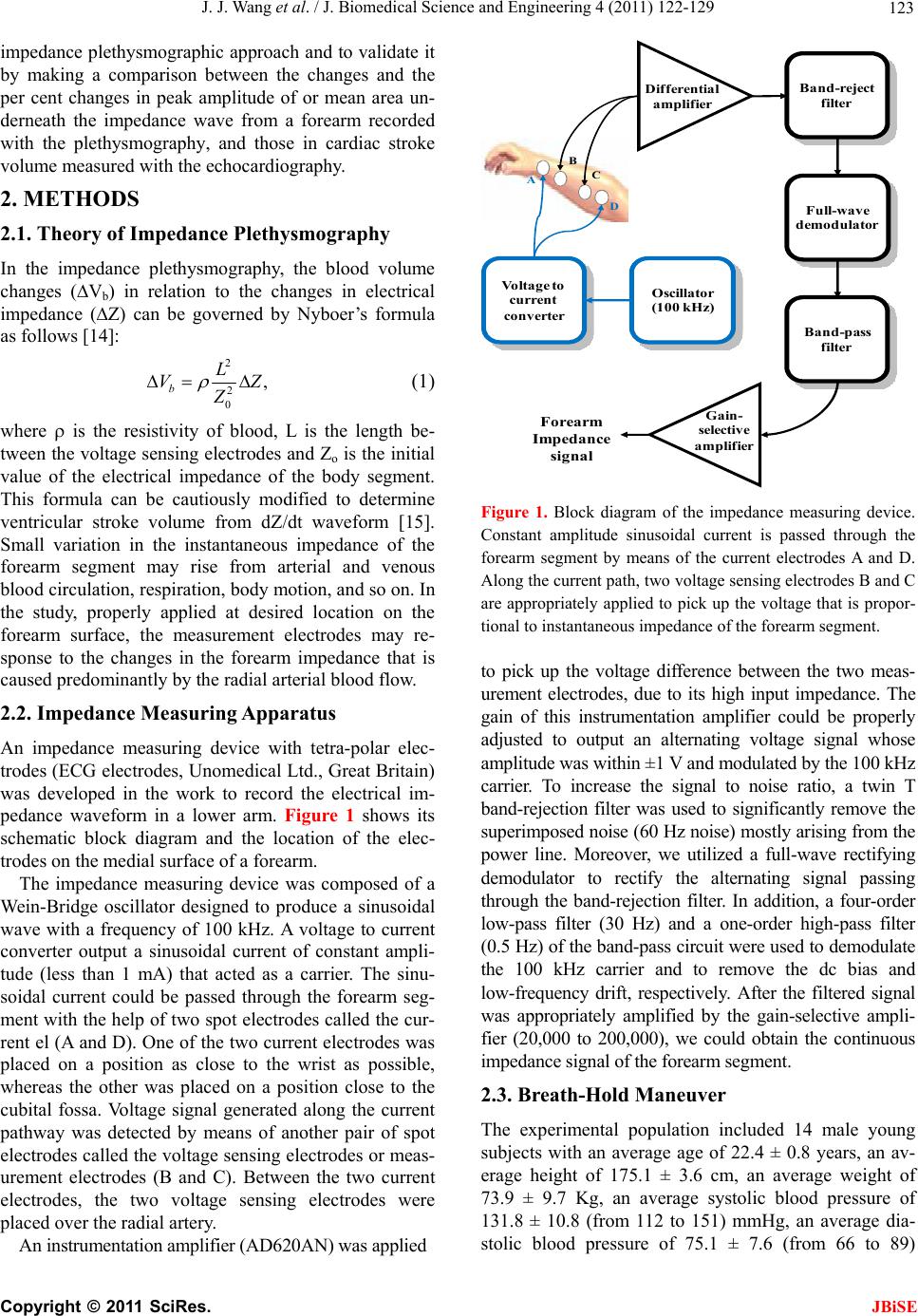
ing current of 100 KHz to the circle-type current elec-
trodes placed directly on the top of the radial artery,
which may result in a higher current density in the radial
lumen. Thus, the change in the forearm impedance am-
plitude may probably follow the change in the radial
blood flow. It suggests that the change in the impedance
amplitude can be more specifically reflected the change
in the stroke volume.
Several factors associated with the impedance changes
are present between individuals. One is the position of
surface electrodes. In most cases, the distance between
the two inner or outer electrodes is different from each
other in the measurement situation, resulting in a con-
siderable change in impedance amplitude. Second is due
to the distinct diameters of radial arteries and different
peripheral tissue compositions. Third is related to the
variation in biological impedance of tissue of interest.
Unfortunately, the present device fails to directly deter-
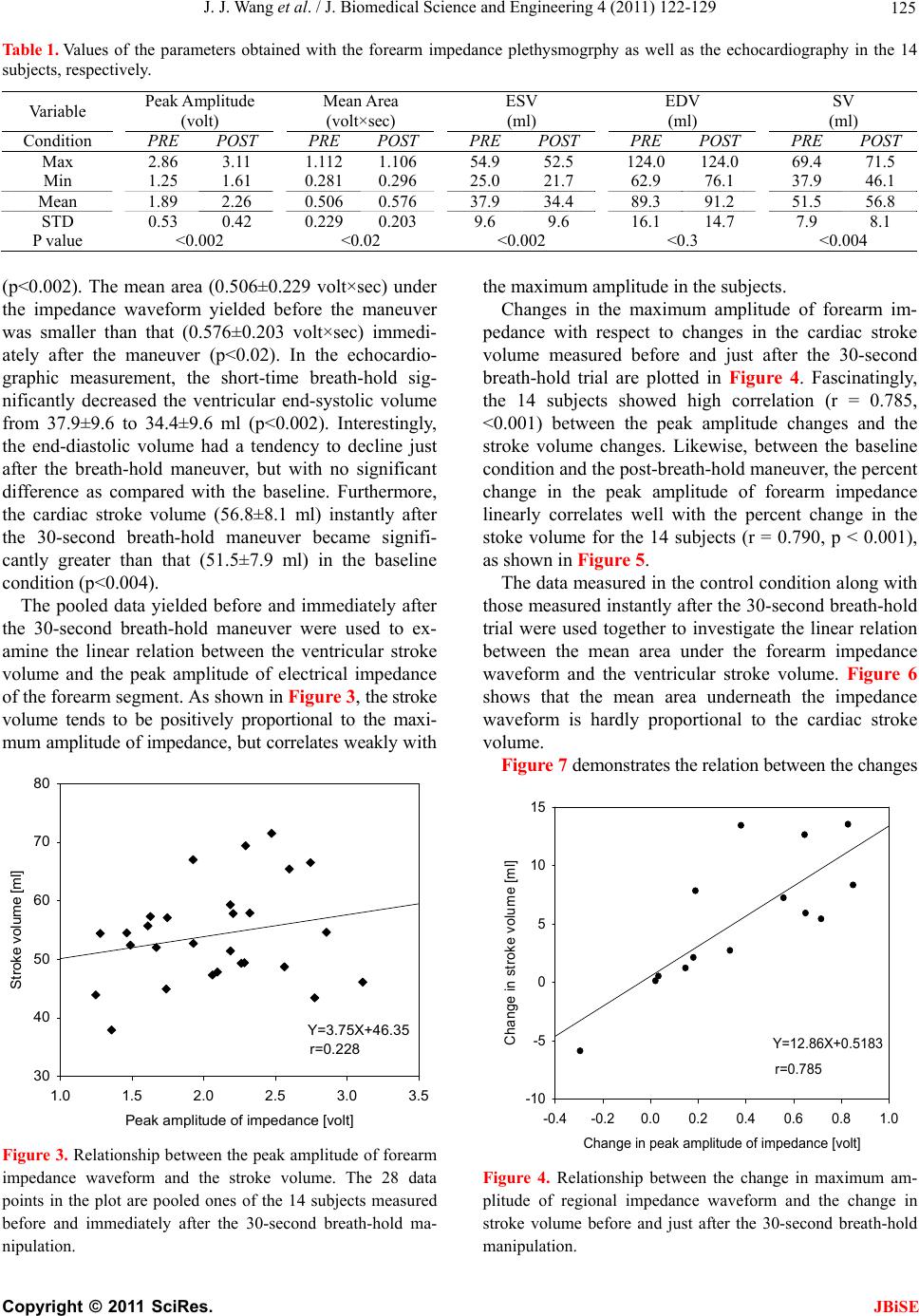
mine the absolute stroke volume. Our results show a
correlation coefficient of less than 0.3 between the
maximum impedance amplitude and stroke volume, with
a similar low coefficient between the underneath area of
the impedance wave and the stroke volume.
5. CONCLUSION
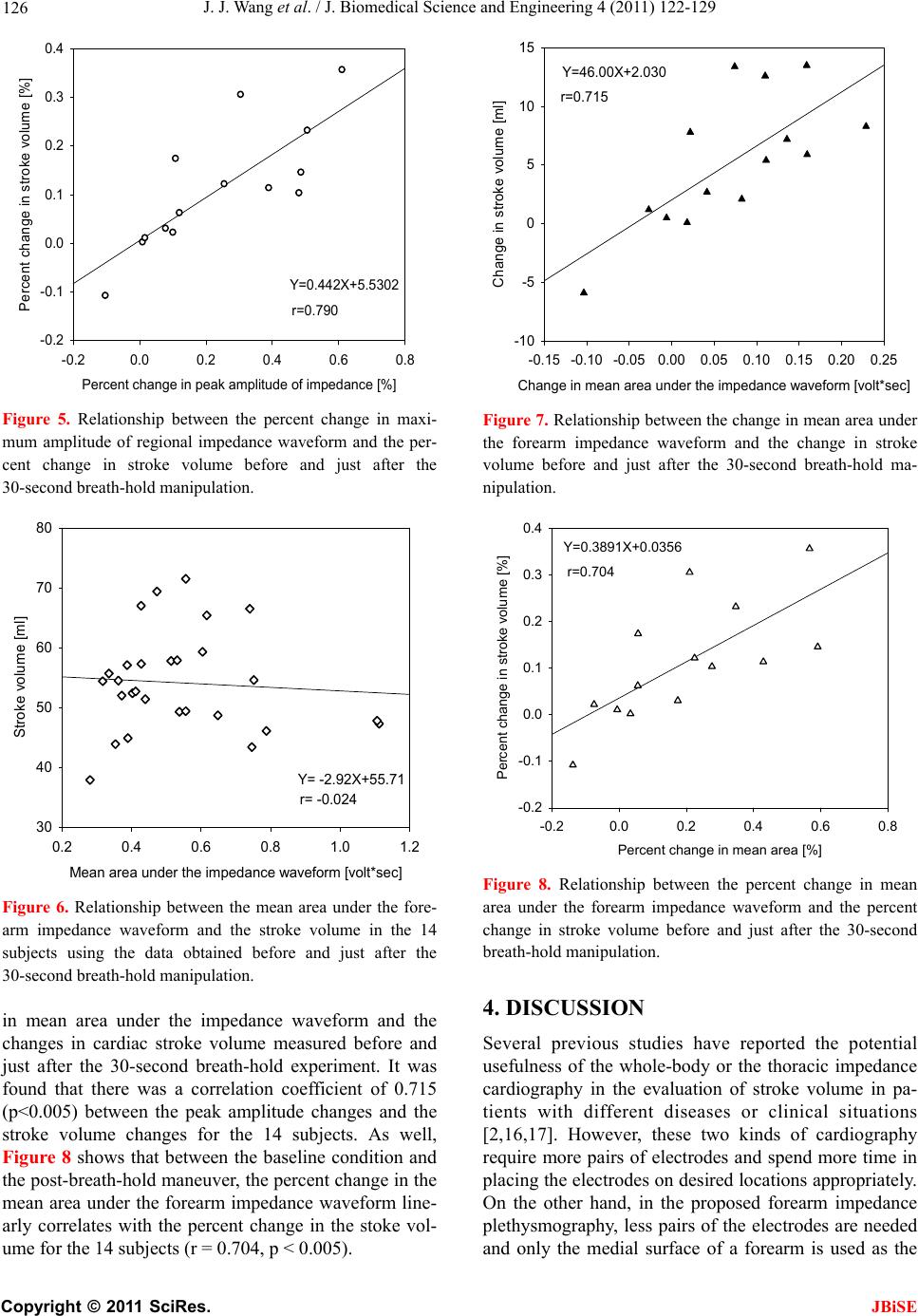
Linear relationships between the changes in amplitude of
and in the area under the forearm impedance waveform
and the changes in stroke volume are shown. Thus, the
forearm impedance plethysmography proposed may be
utilized to assess the beat-to-beat change in cardiac
stroke volume, suggesting its potential for long-term
monitoring ventricular pumping function.
6. ACKNOWLEDGEMENTS
This study was supported by the National Science Council, Taiwan, the
Republic of China, under grant numbers NSC 98-2221-E-214-005-
MY3 and NSC 98-2221-E-075B-001-MY2.
REFERENCES
[1] Absi, M.A., Lutterman, J. and Wetzel, G.T. (2010)
Noninvasive cardiac output monitoring in the pediatric
cardiac Intensive Care Unit. Current Opinion in
Cardiology, 25, 77-79.
doi:10.1097/HCO.0b013e3283362452
[2] Cohen, A.J., Arnaudov, D., Zabeeda, D., Schultheis, L.,
Lashinger, J. and Schachner, A. (1998) Non-invasive
measurement of cardiac output during coronary artery
bypass grafting. European Journal of Cardio-Thoracic
Surgery, 14, 64-69. doi:10.1016/S1010-7940(98)00135-3
[3] Cotter, G., Schachner, A., Sasson, L., Dekel, H. and
Moshkovitz, Y. (2006) Impedance cardiography revisited.
Physiological Measurement, 27, 817-827.
doi:10.1088/0967-3334/27/9/005
[4] Peng, Z.Y., Critchley, L.A., Fok, B.S. and James, A.E.
(2004) Evaluation of impedance based indices of cardiac
contractility in dogs. Journal of Clinical Monitoring and
Computing, 18, 103-109.
doi:10.1023/B:JOCM.0000032720.02801.e6
[5] Woltjer, H.H., Bogaard, H.J., Scheffer, G.J., van der
Spoel, H.I., Huybregts, M.A. and de Vries, P.M. (1996)
Standardization of non-invasive impedance cardiography
for assessment of stroke volume: comparison with
thermodilution. British Journal of Anaesthesia, 77,
748-752.
[6] Atallah, M.M. and Demain, A.D. (1995) Cardiac output
measurement: lack of agreement between thermodilution
and thoracic electric bioimpedance in two clinical
settings. Journal of Clinical Anesthesia, 7, 182-185.
doi:10.1016/0952-8180(94)00050-E
[7] Hahn, G., Sipinkova, I., Baisch, F. and Hellige, G. (1995)
Changes in the thoracic impedance distribution under
different ventilatory conditions. Physiological Measure-
ment, 16, A161-A173.
doi:10.1088/0967-3334/16/3A/016
[8] Imhoff, M., Lehner, J.H. and Lohlein, D. (2000)
Noninvasive whole-body electrical bioimpedance cardiac
output and invasive thermodilution cardiac output in
high-risk surgical patients. Critical Care Medicine, 28,
2812-2818. doi:10.1097/00003246-200008000-00022
[9] Kubicek, W.G., Kottke, J., Ramos, M.U., Patterson, R.P.,
Witsoe, D.A., Labree, J.W., Remole, W., Layman, T.E.,
Schoening, H. and Garamela, J. T. (1974) The Minnesota
impedance cardi ograph-theory and applications. Biomedical
Engineering, 9, 410-416.
[10] Leitman, M. , Sucher, E., Kalu ski, E., Wolf, R., Pele g, E.,
Moshkovitz, Y., Milo-Cotter, O., Vered, Z. and Cotter, G.
(2006) Non-invasive measurement of cardiac output by
whole-body bio-impedance during dobutamine stress
echocardiography: clinical implications in patients with
left ventricular dysfunction and ischaemia. European
Journal of Heart Failure, 8, 136-140.
doi:10.1016/j.ejheart.2005.06.006
[11] Cotter, G., Moshkovitz, Y., Kaluski, E., Cohen, A.,
Miller, J. H., Goor, D. and Vered, Z. (2004) Accurate,
noninvasive continuous monitoring of cardiac output by
whole-body electrical bioimpedance. Chest, 125,
1431-1440. doi:10.1378/chest.125.4.1431
[12] Critchley, L.A., Peng, Z.Y., Fok, B.S. and James, A.E.
(2005) The effect of peripheral resistance on impedance
cardiography measurements in the anesthetized dog.
Anesthesia and Analgesia, 100, 1708-1712 .
doi:10.1213/01.ANE.0000150602.40554.EB
[13] Wong, K.L. and Hou, P.C. (1996) The accuracy of
bioimpedance cardiography in the measurement of
cardiac output in comparison with thermodilution
method. Acta Anaesthesiologica Sinica, 34, 55-59.
[14] Nyboer, J. (1960) Regional pulse volume and perfusion
flow measurements: electrical impedance plethysmography.
Archives of Internal Medicine, 105, 264-276.
[15] Patterson, R.P., Wang, L. and Raza, S.B. (1991)
Impedance cardiography using band and regional
electrodes in supine, sitting, and during exercise. IEEE
C
opyright © 2011 SciRes. JBiSE